 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
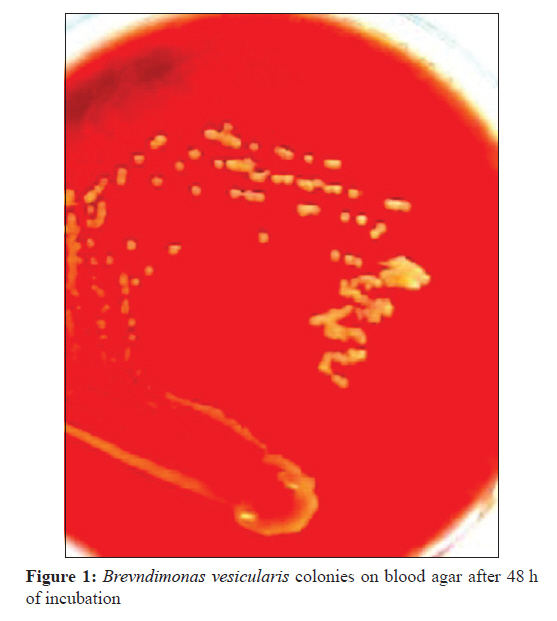
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 420-422 Case Report Brevundimonas vesicularis bacteremia: A rare case report in a female infant SM Bhatawadekar1, J Sharma2 1 Department of Microbiology, Bharati Vidyapeeth Deemed University Medical College, Pune, India Date of Submission: 04-Sep-2010 Code Number: mb11101 PMID: 22120807 Abstract Brevundimonas vesicularis has rarely been isolated from clinical specimens. We report here a case of B. vesicularis bacteremia in a female infant who presented with fever, vomiting and altered sensorium. USG abdomen showed mild hepatomegaly, moderate ascitis with bilateral mild basal pleural effusion. Blood culture was processed by BACTEC BD. Isolate was identified as B. vesicularis, by API ID 32 GN automated system. We have come across only one report of neonatal sepsis caused by B. vesicularis from India. To the best of our knowledge, this is one of the rare case reports of B. vesicularis bacteremia in a female infant. Keywords: Bacteremia, B. vesicularis , immunocompetent infant Introduction Brevundimonas vesicularis, formerly grouped with Pseudomonas, is an aerobic nonsporing and nonfermenting, slowly growing gram-negative bacillus. There are few reports in the literature of infections caused by B. vesicularis in immunocopromised as well as in healthy patients. Source of infection is either hospital environment or community. These organisms are infrequently isolated in clinical microbiology laboratories. Recently three cases of B. vesicularis infection have been reported. [1],[2],[3] This might be due to increasing use of better culture and identification facilities, especially automated system. In most of the reports of B. vesicularis infection isolates have been identified by Mini API-automated system, using ID 32 GN strip. We have come across only one report of neonatal sepsis caused by B. vesicularis from India. [3] Case Report A 1-year-old female child presented with moderate intermittent fever of 15 days duration and vomiting, decreased oral intake and altered sensorium since 1 day. There was no history of seizures. On examination, the infant was drowsy and irritable, afebrile, with pulse rate of 118/min and respiratory rate of 24/min. Per abdomen examination showed mild hepatomegaly with ascitis. Examination of the respiratory, cardiovascular and central nervous systems was within normal limits. Relevant laboratory findings were: Hb 9.5 g/dl, PCV 28.3%, platelets 35 000/mm 3 . Over the next two days the Hb decreased to 8.2 g/dl and platelet count reduced to 20 000/mm 3 . Other investigations were: Serum bilirubin - total 2.3 mg/dl, direct 1.2 mg%, aspartate aminotransferase (AST) - 525 U/l, alanine aminotransferase (ALT) - 225 U/l. USG abdomen showed mild hepatomegaly, moderate ascitis with bilateral mild basal pleural effusion. A provisional diagnosis of dengue fever with differentials of viral hepatitis and leptospirosis were considered. Rapid ELISA test was negative for dengue IgG, IgM and NS1 antigen and for Leptospira IgM antibodies. Blood culture sample was processed by the automated and computerized blood culture system (BACTEC BD). The blood culture medium used was soybean casein digest broth. Growth was detected on second day. Positive blood culture sample was subcultured on blood agar and MacConkeys agar. Dark yellow orange coloured colonies were grown on blood agar after 48 h incubation [Figure - 1]. On MacConkeys agar there was no growth. The organism was a motile gram-negative bacillus. It was oxidase positive. The isolate was identified as B. vesiculararis on the basis of the biochemical characteristics tested by the API ID 32 GN automated identification system (bioMιrieux, Marcy I′ Ιtoile, France). These included the characteristics of positive activity of d-maltose/d-glucose oxidation; negative activity of inositol/d-sorbitol/l-arabinose oxidation; negative activity of l-alanine/capric acid/potassium 5-ketogluconate/trisodium citrate decarboxylation; negative activity of nitrate reduction and indole production. Antibiotic sensitivity was tested by API ATBTM G-5, automated system. The organism was resistant to ceftazidime, cefoxitin, cotrimaxazole, tobramycin, netilmicin. In view of hemoconcentration, thrombocytopenia, pleural effusion and ascitis a provisional diagnosis of dengue fever was made with differential diagnosis of leptospirosis and viral hepatitis. With working diagnosis of dengue fever child was managed with intravenous fluids and cefotaxime. Later with increase in liver enzyme and negative dengue test leptospirosis was thought, in view of which crystalline penicillin was started. During the course of stay patient′s sensorium gradually improved and patient became hemo dynamically stable. She was discharged after 7 days. Discussion There have been only few descriptions of bacteremia caused by B. vesicularis reported in literature. Its isolation from blood sample was reported in few cases. [1],[3],[4],[5],[6],[7] Few cases of B. vesicularis infection were attributed to nosocomial sources [1],[2],[5],[6] and some cases to community sources. [4],[7],[8],[9] In majority of the cases underlying diseases or predisposing factors such as biliary pancreatitis, acute myelogenous leukemia, mitral valve stenosis, sickle cell anaemia with functional asplenia and end-stage renal disease treated by haemodialysis contributed to B. vesicularis infections due to the patients′ immunocompromised state. [1],[5],[6],[7],[10] B. vesicularis infection has, therefore, been classified as opportunistic. Few cases have been reported in immunocompetent patients. [4],[8],[9] B. vesicularis has been isolated from other samples also; in the case of keratitis following in situ keratomileusis, cutaneous infection, septic arthritis, peritonitis. [2],[8],[9],[10] The low number of cases reported of B. vesicularis infection in humans limits the body of knowledge on the spectrum of disease caused by this pathogen as well as optimal treatment regimens. In this case, blood culture sample was received 2 days after admission of the patient. B. vesicularis bacteremia was confirmed on the 7 th day, during this period in view of hemoconcentration, thrombocytopenia, pleural effusion and ascitis a provisional diagnosis of dengue fever was made with differential diagnosis of leptospirosis and viral hepatitis B. vesicularis in our case was sensitive to amoxicillin, piperacillin, ticaracillin, 1 st generation cephalosporins, imepenem meropenem, amikacin, gentamicin, ciprofloxacin, cefotaxime. The isolate was resistant to ceftazidime, cefoxitin, cotrimaxazole, tobramycin, netilmicin. B. vesicularis resistant to aztreonam meropenem, piperacillin-tazobactam, ciprofloxacin, ceftazidime, ceftrioxone have been reported. [5],[6] It is difficult to decide on the best antimicrobial for invasive infection due to B. vesicularis, because of the low number of reported cases in humans caused by this pathogen; the fact that isolates come from various countries or findings from different laboratories. Almost all cases of B. vesicularis infection reported in the literature are from other countries. We have come across only one report of neonatal sepsis caused by B. vesicularis in Indian patient. [3] Most of the cases of B. vesicularis infection have been reported in adult age group. This infection was very rarely reported in neonates and infants. Our case is one of the rare case reports of community acquired B. vesicularis infection in an immunocompetent child. In conclusion, since cases of infections due to B. vesicularis are reported with increasing frequency, our case report reinforces the hypothesis that B. vesicularis can cause disease in a person without predisposing disease. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11101f1.jpg] |
| |||||||||
{kind=link}