 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
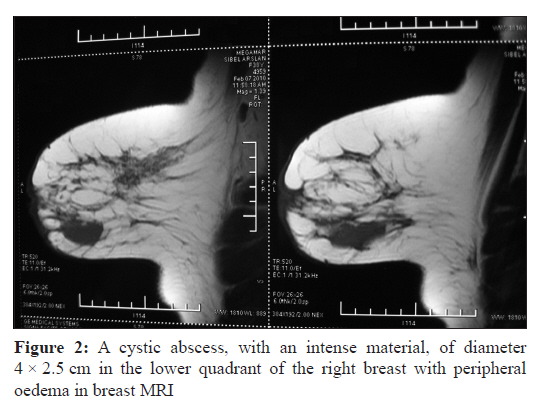
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 425-427 Case Report Successfully treated Mycobacterium abscessus mastitis: A rare cause of breast masses KK Yasar1, F Pehlivanoglu1, G Sengoz1, N Cabioglu2 1 Department of Clinical Microbiology and Infectious Diseases, Haseki Training and Research Hospital, Adnan Adivar Cad. Aksaray, Istanbul 343, Turkey Date of Submission: 28-Apr-2011 Code Number: mb11103 PMID: 22120809 Abstract Rapidly growing mycobacteria are pathogens responsible for cutaneous or subcutaneous infections especially occurring after injection, trauma or surgery. We describe a patient with Mycobacterium abscessus mastitis that presented as a mass lesion and haemorrhagical discharge. It was initially diagnosed and treated as fibrocystic disease and non-specific abscess. Full recovery was obtained with combination therapy of clarithromycin, linezolid and amikacin without surgical debridement followed by several abscess aspirations. Atypical mycobacteria should be considered in diagnosis of chronic breast lesions in endemic areas. This is the first reported case of mastitis due to M. abscessus in Turkey. Keywords: Breast mass, M. abscessus, rapidly growing mycobacteria Introduction Breast tuberculosis (TB) is a rare form of TB. The incidence of the disease is less than 0.1% of all breast lesions in Western countries and 4% in TB endemic countries. [1] In Turkey, TB is an endemic disease but breast TB is very rarely reported. [2] Breast lesions caused by atypical mycobacteria have recently been reported only after year 2000. [3],[4] Mycobacterium abscessus, a rapidly growing mycobacterium, is ubiquitous in soil and aqueous environments. The most common clinical picture of disease caused by M. abscessus is pulmonary and skin and soft tissue infections. [5] Postinjection abscesses were also the first disease due to rapidly growing mycobacteria to be recognized in an epidemic form. [6] M. abscessus is rarely implicated in mastitis. [4] Breast TB even caused by atypical mycobacteria should be considered in patients with breast swellings, discharge and chronic abscesses that non-responsible to broad-spectrum antibiotics. We report a patient with M. abscessus mastitis that was initially presumed as fibrocystic disease and abscess. To our knowledge, mastitis due to M. abscessus has not been yet reported in Turkey. Case Report A 38-year-old HIV negative woman with a 3-year history of bilaterally fibrocystic disease and breast abscess presented with a change in characteristics in her right breast abscess in last 2 months. Her right breast mass got bigger with associated pain, redness and haemorrhagic discharge from a fistula. Non-specific mastitis was the initial diagnosis 1 year ago and was unresponsive to antimicrobial agents. The patient had undergone aspiration for drainage and sampling many times during this period but cultures for both non-specific micro-organisms and mycobacteria were sterile. She denied having history of fever, night sweats, weight loss and respiratory symptoms. There was no family history for breast cancer and no personal history of tuberculosis. Physical examination revealed a 3-cm, mobile and painful mass in the lower outer quadrant of her right breast and palpable lymph nodes in the ipsilateral axilla. Since her complaints for the right breast mass changed during last 2 months, the surgeon thought a specific lesion and consulted the patient with our clinic. There was discharge from a fistula and skin retraction [Figure - 1]. Mammography and sonographic images showed a local asymmetric density and a cystic lesion around areola with a 14 × 5 mm diameter and another associated cystic lesion localized profoundly with a 30 × 18 mm diameter. Breast MRI [Figure - 2] revealed a cystic abscess, with an intense material, of diameter 4 × 2.5 cm in the lower quadrant of the right breast with peripheral oedema, and axillary lymph nodes. The pathological examination of the aspiration sample showed suppurative inflammation but non-specific cultures were sterile. Aspiration sample culture was repeated for mycobacteria on the Lφwenstein-Jensen medium. Acid-fast bacilli were not found on acid-fast staining and PCR for mycobacterium was also negative but a non-pigmented mycobacterium was isolated from the Lφwenstein-Jensen medium within 10 days from inoculation. The isolate was confirmed to be M. abscessus with the GenoType Mycobacterium CM/AS assay (Hain Lifescience® , Germany). There was no evidence for pulmonary lesion or disseminated mycobacterial disease. The patient was diagnosed having mastitis due to M. abscessus and therapy consisting of linezolid (600 mg twice a day), clarithromycin (500 mg twice a day) and amikacin (1 g a day). Amikacin was discontinued after 3 weeks; linezolid was administered for 2 months and clarithromycin for 4 months. Her complaints remarkably regressed after 4 weeks. At the end of week 8, control MRI images showed full recovery [Figure - 3] and the mass in the right breast and axillary lymph nodes had totally disappeared. The therapy was completed by 4 months and the patient was followed up for 1 year. There was no recurrence or any problem within this period. Discussion M. abscessus is the most common agent isolated from infections due to rapidly growing mycobacteria. [5] One of the most common forms of disease caused by M. abscessus is post-traumatic/postinjection abscesses. [6],[7] But breast abscess caused by M. abscessus is extremely rare. Our patient had several fine needle aspirations within the last year before her specific lesion in the right breast was found. Of 125 cases with infections due to rapidly growing bacteria, 54% of cutaneous infections occurred after the patients had undergone a surgical procedure such as mammoplasty. [8] Nosocomial infections due to M. abscessus may result from local skin trauma or cutaneous injection, and the organism may result in nosocomial outbreaks of postinjections. [6],[9] Villanueva et al. [6] reported the largest outbreak of postinjections due to M. abscessus and they found that the incubation period ranged from 7 to 121 days. The inoculation of the agent into the breast of our patient through fine needle aspiration may be the probable way of contamination. The time between the first aspiration procedure and clinical picture was too long. In addition, she had had bilaterally fibrocystic disease and abscess for 3 years and all samples obtained within this period were sterile. Therefore, the initial diagnosis was unclear and the chronic disease due to M. abscessus was an undetected occult reason for 3 years. The isolation of the responsible agent in the Lφwenstein-Jensen medium within shorter time was a suspect sign for atypical mycobacteria in our patient. So, a molecular method for identifying nontuberculous mycobacteria was performed. The GenoType Mycobacterium CM/AS assay is a rapid identification method for a broad spectrum of clinically significant Mycobacterium species. Optimal antimicrobial treatment of rapidly growing mycobacterial infections remains poorly established. [10] There is a lack of prospective controlled studies demonstrating a correlation between in vitro antimicrobial susceptibility pattern and clinical response for atypical mycobacteria. Clarithromycin has been successful in many reports and should be included as the core of combination therapy. Linezolid, imipenem, cefoxitin, amikacin and fluoroquinolones were also reported as effective agents for rapidly growing mycobacteria and skin and soft tissue infections may be successfully treated with combination therapies in 3-6 months with an excellent change for cure either with or without concomitant surgical debridement. [11] Combination therapy with clarithromycin, linezolid and amikacin was effective and full recovery was obtained for this patient without surgical debridement following abscess aspiration in the present report. Since breast lesions of this patient disappeared at the end of the second month, the therapy was completed in 4 months. During the follow-up period, there was no relapse or any other problem suggesting treatment failure. Therefore, the duration of treatment was considered adequate. Surgical therapy is an important adjunctive tool in treating these infections. A combined therapeutic approach including skilled surgical drainage, debridement and prolonged (longer than 3 months) treatment with combined antimicrobial agents has been suggested as optimal therapy and has good outcomes for these infections. M . abscessus and other mycobacteria should be kept in mind for differential diagnosis in patients who have no response to standard antibiotic therapy with chronic breast or soft tissue infections including recurrent breast abscess. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11103f3.jpg] [mb11103f1.jpg] [mb11103f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}