 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
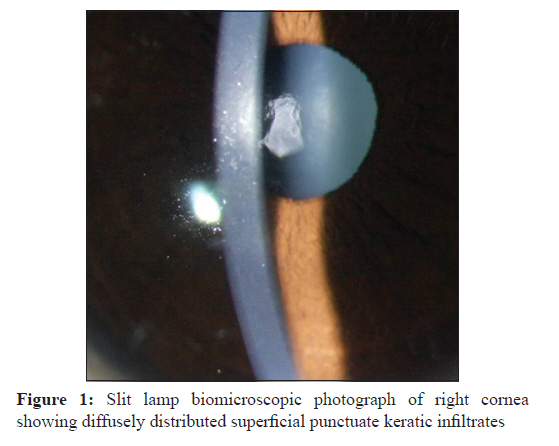
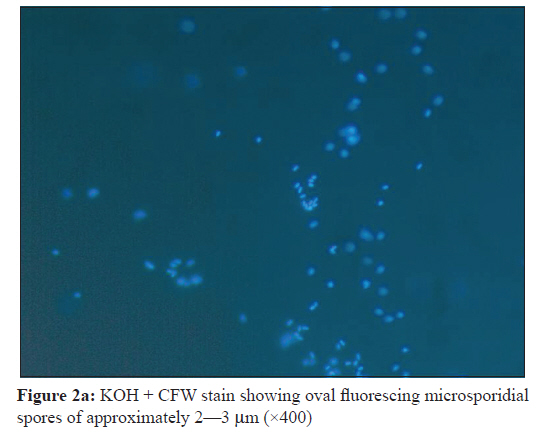
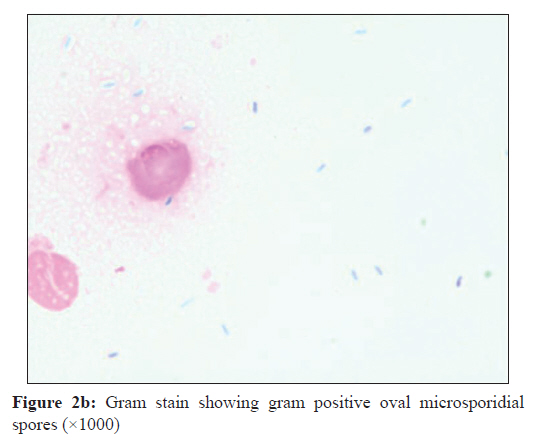
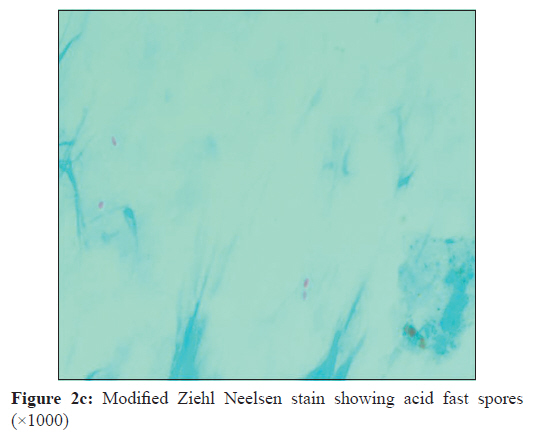
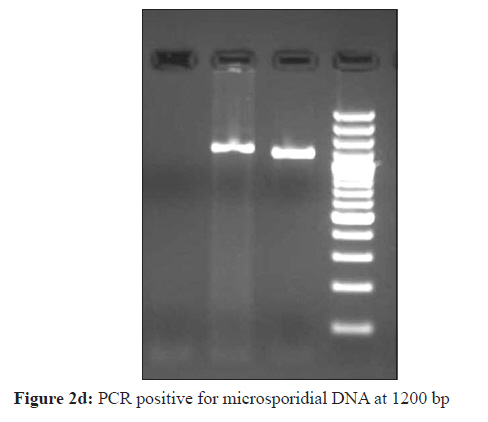
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 428-430 Case Report Microsporidial keratoconjunctivitis in an immunocompetent patient with a past history of laser in situ keratomilieusis surgery ML Bommala1, S Nalamada1, S Sharma2, P Garg3 1 Jhaveri Microbiology Centre, Brien Holden Eye Research Centre, Hyderabad 500 034, India Date of Submission: 20-Feb-2011 Code Number: mb11104 PMID: 22120810 Abstract Ocular infection with microsporidia has been documented in both immunocompetent and immunocompromised patients. Sources and mode of human infection with microsporidia have been difficult to ascertain although exposure to water may be an important risk factor. Of four genera that have been reported in human disease, only the genera Nosema, Encephalitozoon and Septata are documented to cause ocular infection. Here, in our case a healthy 30-year-old man who had undergone bilateral laser in situ keratomilieusis surgery two and half years back presented with a 10-day history of redness and 4-day history of blurring of vision in the right eye. On presentation, his best-corrected visual acuity was 20/20 partial in both eyes. Slit lamp examination revealed multiple pin head shaped infiltrates in the right cornea. Examination of the left eye was unremarkable. Based on microscopic demonstration of numerous microsporidial spores in the corneal scrapings, a diagnosis of microsporidial keratitoconjunctivitis was made. On treatment with oral albendazole, the cornea became clear with complete resolution of symptoms and signs within two weeks. Keywords: Albendazole, keratitoconjunctivitis, laser in situ keratomilieusis, microsporidia Introduction Laser in situ keratomilieusis (LASIK) is a common surgical refractive error correction procedure. Although the safety of LASIK surgery is well proven, it can be complicated by sight-threatening infection. Case reports of late onset microbial keratitis after LASIK have been reported in the literature. [1] Gram positive organisms and Mycobacterium spp. are the common organisms isolated followed by gram negative organisms, fungi, Nocardia, Acanthamoeba. [1] Microsporidial keratoconjunctivitis and stromal keratitis have been reported worldwide including India, however, post LASIK infection due to microsporidia are rare. A literature search showed one case reported from Texas, USA in January 2003. No case has been reported from India so far although LASIK is a common procedure done in most advanced ophthalmology setups across India. We report a case of late onset Microsporidial keratitis in an immunocompetant patient with a history of LASIK surgery. Case Report A healthy 30-year old man who had bilateral LASIK surgery two and half years back was referred to our institute on 11 th October 2010 with a 10-day history of redness and 4-day history of blurring of vision in the right eye. He had been treated with occupol (polymixin B and chloramphenicol) and refresh tears for 1 week before being referred to the corneal clinic of our institute for increased epithelial opacities with sub epithelial infiltrates in the right eye. His visual acuity was 20/20 in both eyes. In the right eye, the conjunctiva had trace hyperemia. Slit lamp examination of right cornea revealed multifocal, minute, round to oval superficial punctate keratic infiltrates diffusely distributed throughout the corneal epithelium [Figure - 1]. The corneal stroma was clear. The anterior chamber was quiet. Fundus examination was unremarkable. Examination of the left eye was unremarkable. There was no history of head/ocular injury in the past. There was no history of wearing contact lenses after LASIK surgery. His family history was insignificant. Based on these findings, a diagnosis of microbial keratitis was made. Corneal scraping was collected under topical anesthesia with the help of slit lamp magnification with a sterile blade no. 15 on a Bard Parker handle and was submitted for microbiologic evaluation according to institute protocol. The scraped material was smeared on presterilized glass slides for microscopic examination using Gram stain, Giemsa stain, 10% potassium hydroxide with 0.1% calcofluor white preparation (KOH + CFW) and modified Ziehl Neelsen stain (1% H 2 SO 4 ). The corneal scraping was also collected for microsporidial PCR in 300 ml of phosphate-buffered saline (pH 7.2). The detailed description of PCR method followed and various primers used has been explained in our previous publications. [2] On direct microscopy, oval fluorescing bodies measuring approximately 2-3 mm characteristic of Microsporidia spores were seen in KOH + CFW stain [Figure - 2]a. Gram stain of the corneal scraping also revealed gram positive oval shaped spores of approx 2-3 mm [Figure - 2]b and spores were acid fast [Figure - 2]c. PCR was positive for microsporidial DNA [Figure - 2]d. Based on the above findings, a diagnosis of microsporidial keratitoconjunctivitis was made and the patient was put on artificial tears and oral albendazole twice a day, and he was followed up after 2 weeks. On review after 2 weeks, the symptoms had improved and cornea was clear with complete resolution of symptoms and signs. Discussion Infectious keratitis after LASIK is a sight threatening complication caused by various bacteria including atypical mycobacteria, fungi, Acanthamoeba, Nocardia. [1] A search of English Medical literature (PUB MED) revealed only one case of microsporidial keratitis in a healthy patient with a history of LASIK surgery done 3 years back in Texas, USA. [3] He was a healthy 49-year-old man who had undergone LASIK in both eyes 3 years back and was referred to their eye institute with a 2 month history of irritated left eye. Visual acuity was 20/20 and 20/25 in right and left eye, respectively. On slit lamp biomicroscopy, there were superficial punctuate epithelial opacities distributed diffusely throughout the corneal epithelium in the left eye. Modified trichrome stain of corneal scrapings revealed intracellular and extracellular organisms consistent with Microsporidial spores. Within a week of treatment with topical fumagillin and oral albendazole, improvement of symptoms was noted with decreased density of corneal lesions. The patient had complete resolution of infection with no recurrence after 6 months of follow up. Microsporidia are obligate intracellular parasite/fungi belonging to the phylum Microspora and are recognized as opportunistic infectious agents worldwide. [4],[5] They produce environment resistant spores which infect both vertebrates and invertebrates. Ocular infection with microsporidia has been documented in both immunocompetent and immunocompromised patients. [5] Sources and mode of human infection with microsporidia have been difficult to ascertain although exposure to water may be an important risk factor. [5],[6] Seasonal outbreaks (rainy season) of epidemic keratoconjunctivitis associated with microsporidia have been reported from Eastern India. [7] Significantly higher prevalence of microsporidial keratoconjunctivitis in rainy season has also been reported from central India. Personal communication with ophthalmologists from other parts of India also point towards prevalence of this condition in most part of India. Therefore, it is possible that our patient may have acquired the infection through contact with contaminated water or another infected individual. Although late onset LASIK infections have been reported in the literature, [8],[9] the importance of LASIK surgery in causation of microsporidial keratitis is uncertain in our patient as it was performed two and half years prior to presentation. On one hand, wide range of drugs have been suggested for the treatment of microsporidial keratoconjunctivitis and on the other the condition is purported to be self-limiting. [10] Anecdotal reports of specific drug treatment of microsporidiosis include albendazole, itraconozole, propamidine isethionate and fumagillin, but there effectiveness remains debatable. Albendazole is a broad spectrum antihelminthic that has been shown to be effective in treatment of microsporidiosis. [10] Our patient may have responded to albendazole; however, spontaneous resolution cannot be ruled out. Thus this report demonstrates the probable risk of microsporidial keratitis in an immunocompetant patient years after LASIK with no antecedent contact lens wear and emphasizes the importance of life long post operative vigilance by patient and physician. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11104f2c.jpg] [mb11104f2d.jpg] [mb11104f1.jpg] [mb11104f2a.jpg] [mb11104f2b.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}