 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
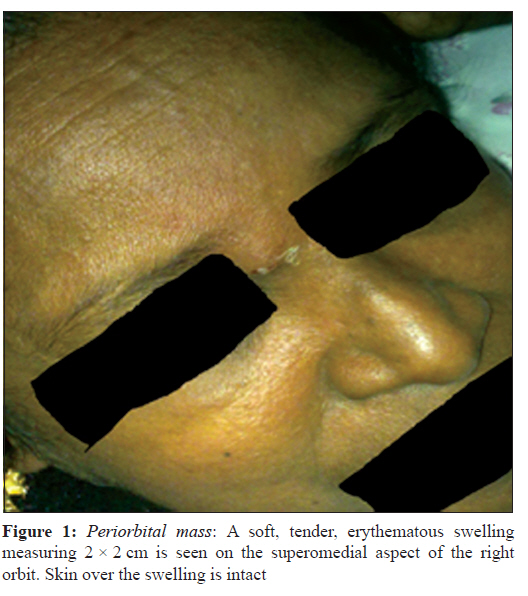
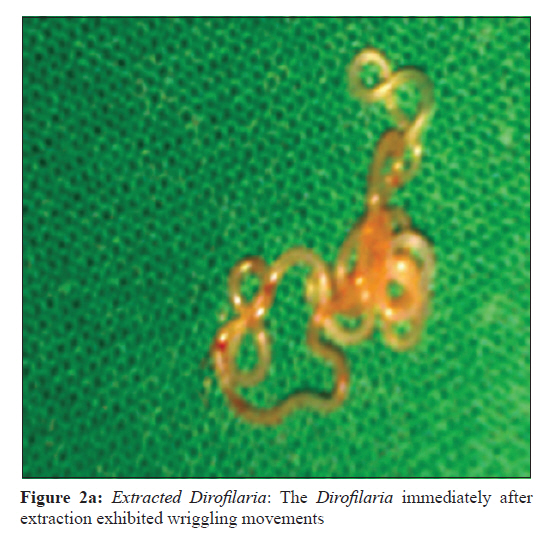
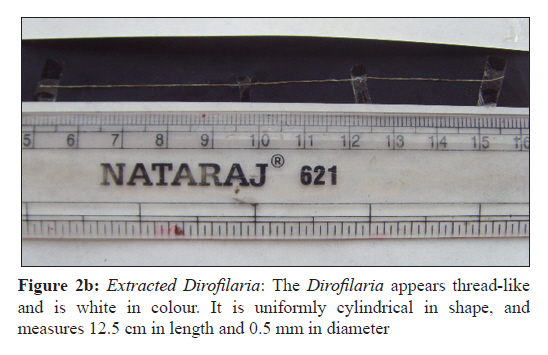
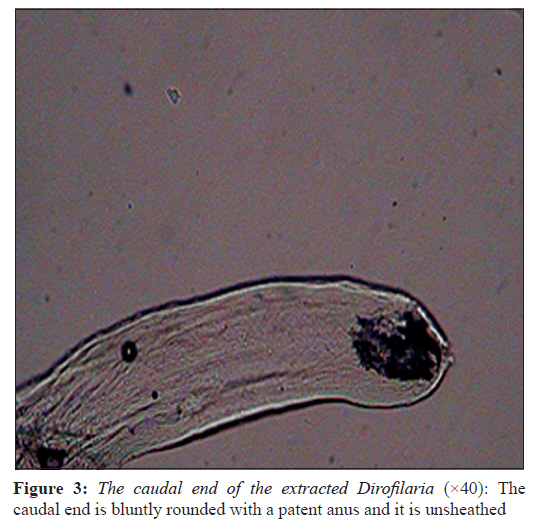
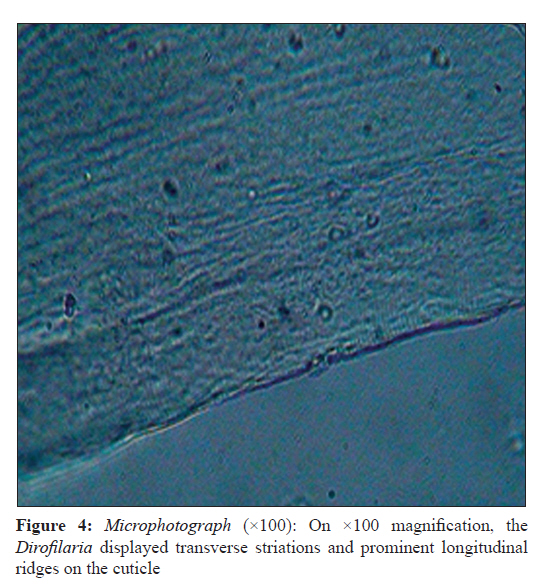
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 431-433 Case Report Periorbital mass with cellulitis caused by dirofilaria K Joseph1, AR Vinayakumar2, S Criton3, MS Vishnu2, SE Pariyaram2 1 Department of Microbiology, Amala Institute of Medical Sciences, Thrissur - 680 555, Kerala, India Date of Submission: 05-May-2011 Code Number: mb11105 PMID: 221208mb11 Abstract Dirofilariasis is a zoonotic disease caused by Dirofilaria, a parasite of domestic and wild animals. The disease is transmitted by inoculation of mosquitoes infected with the microfilariae during their blood meal. Accidental infection of man results in lung nodule, subcutaneous mass anywhere in the body or ocular lesion that may be subconjunctival or periorbital. The incidence of ocular dirofilariasis is on the rise in several parts of India particularly in Kerala. Here we report a case of ocular dirofilariasis with cellulitis presenting as a periorbital mass. Keywords: Dirofilaria, periorbital mass, zoonotic disease Introduction Dirofilaria is a common parasite of dogs, cats and raccoons. Accidental human infection with dirofilaria results in lung nodule, inflammatory subcutaneous mass or subconjunctival nodule. [1],[2] The genus Dirofilaria consists of D. immitis that can cause pulmonary lesions, and D. repens and D. tenuis that can cause ocular lesions. Man gets infected with the infective larvae through the bites of arthropods like mosquitoes, fleas and ticks after biological incubation of larvae in them. Case Report A 50-year-old female patient presented at ENT out patient department with sore throat and cold of four days duration and swelling around the right eye and over the frontal sinus since two days. On examination, there was tenderness over frontal and ethmoidal sinuses. A provisional diagnosis of frontal sinusitis was made and the patient was treated conservatively with antibiotics. Within two days, the oedema subsided and the swelling localised to the superomedial aspect of the right orbit, the size of which was 2 × 1.5 cm and was tender. A CT scan of paranasal sinuses and orbit was done, which showed an obstructed right nasolacrimal duct. Five days later, the patient attended the ENT OPD for review. The swelling persisted and by then had increased to about 2 × 2 cm [Figure - 1]. Aspiration with a wide bore needle was done. To the surgeons′ surprise, a live worm wriggled out of the opening which was later identified as Dirofilaria repens. The patient was given a course of antibiotics and was advised to come for review a week later. Follow up Upon review, the patient underwent a USG orbit which was found to be within normal limits. Following the extraction of the Dirofilaria, the patient recovered fully and no further treatment was required. No other nodules appeared. Microbiological study The nematode was white, thread-like, measuring 12.5 cm in length and 0.5 mm in diameter [Figure - 2a]a and [Figure 2b]. The diameter was almost same throughout the length of the worm. The helminth exhibited wriggling movements even 2 h after extraction. Microscopically, it showed smooth cuticle and transverse striations with longitudinal ridges. The caudal end was bluntly rounded with a patent anus [Figure - 3] and [Figure - 4]. It was unsheathed. The nematode was identified as Dirofilaria repens. The length of the female may vary from 8 to 13 cm and males from 4 to 4.8 cm. [4],[7] The nematode, being 12.5 cm long, was identified as female. Based on its microbiological study, geographical location of the patient and clinical presentation of the lesion, the nematode was identified as female Dirofilaria repens. Discussion Dirofilariasis, a disease commonly found in carnivorous mammals like dogs, cats, wolves, foxes and raccoons, is uncommon in humans. [3] Human dirofilariasis occurs following accidental infection caused by filarial worms of the genus Dirofilaria which includes D. immitis, D. repens, D. tenuis, D. ursi etc. Dirofilaria immitis, a parasite of dogs, is the most common species of Dirofilaria that infects man and is found in the heart and blood vessels. D. repens, D. tenuis, D.ursi and D. subdermata are parasites of cats and dogs, raccoons, bears and porcupines respectively and are found in the subcutaneous tissues of man. [8] D. repens belongs to Phylum Nematoda, Class Secernentea, Order Spirurida and Family Onchocercidae. The suitable vectors for this parasite are mosquitoes belonging to the genera Culex, Aedes and Anopheles, Fleas and Ticks. [5],[10] Adult female worms of D. repens produce thousands of microfilariae into the circulation of the infected animals which are ingested by zooanthrophilic arthropods during a blood meal. After biological incubation in the vectors, the infective larvae are reintroduced back into the vertebrate host. Man is an aberrant host and accidental human infection results in subcutaneous mass anywhere in the body, preferentially in and around the eye or in a subconjunctival nodule. Adult worms do not reach maturity in a normal human host and do not produce microfilaria as humans are a dead end host. [4] The identification of the nematode is made on its morphological characteristics. D. repens is a nematode with a long thin filariform appearance. The length of the female may vary from 8 to 13 cm. and males from 4 to 4.8 cm. [4],[7] The adult Dirofilaria nematodes have short rounded tails with a patent anus and pointed cephalic end. Mouth is simple without lips. It is unsheathed. All Dirofilaria have fine transverse striations on the cuticle and abundant somatic musculature. [3],[5] In addition, D. repens has prominent external longitudinal ridges on cuticle which are absent in D. immitis. The extracted Dirofilaria is presumably identified as immature female worm of D. repens based on its morphology, geographical location of the patient and the clinical presentation. The first case of human ocular dirofilariasis was reported by Addario in 1885 from Milan, Italy and was described as an infection by Filaria conjunctivae. A total of 397 cases of human subcutaneous dirofilariasis have been reported from 30 countries according to a review of world literature. [8] D. repens infection is usually found in the Mediterranean region, Sub-Saharan Africa and Eastern Europe. Italy is with the highest prevalence of human dirofilariasis (66%), followed by France (22%), Greece and Israel. D. repens occurs more commonly in adults (40-49 years), but available literature shows wide variation in age, ranging from 14 to 70 years in India. In Sri Lanka, human infection with D. repens is a common zoonotic infection, where children younger than nine years are most likely to be infected. The youngest individual reported was aged four months. In India, the incidence is on the rise, infections being reported from Kerala, [6] Tamil Nadu, [7] Karnataka, [5],[8] Assam, [9] and Maharashtra. [10] The rise in incidence could be attributed to mosquito density, warm climate and close contact with cats and dogs which have abundant microfilariae. Complete surgical excision of the subcutaneous lesion or simple extraction of the worm is the treatment of choice for patients with human dirofilariasis caused by D. repens. Enhanced awareness of this fast emerging zoonotic infection in India among microbiologists, ophthalmologists and surgeons will increase the prevalence rate and help in early detection that will improve the patient care. Acknowledgement We are grateful to Dr. Agnessamma Jacob, Department of Pathology of Amala Institute of Medical Sciences, Thrissur, Kerala for her help in the histopathological study of the Dirofilaria. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11105f2a.jpg] [mb11105f4.jpg] [mb11105f3.jpg] [mb11105f2b.jpg] [mb11105f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}