 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
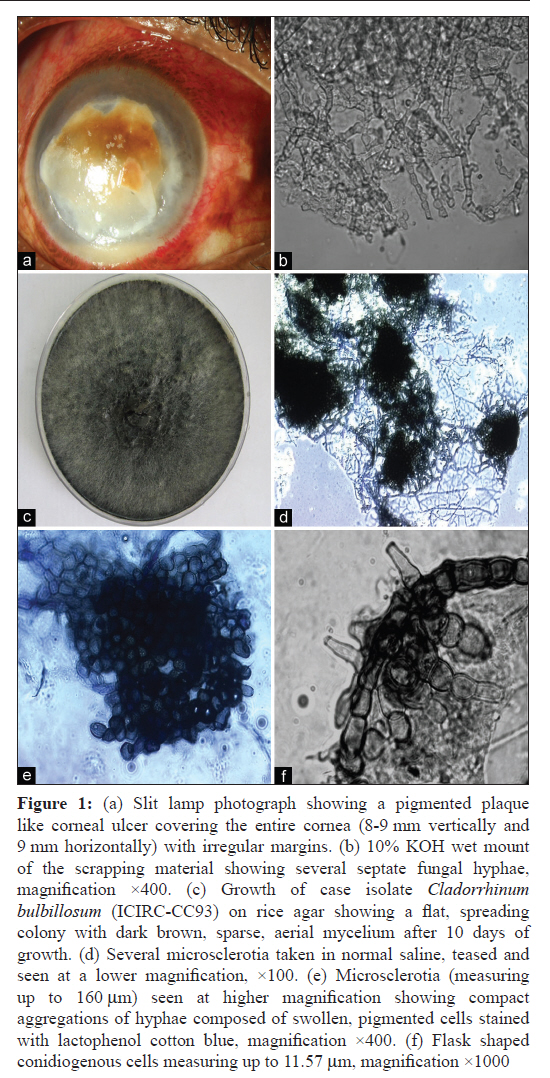
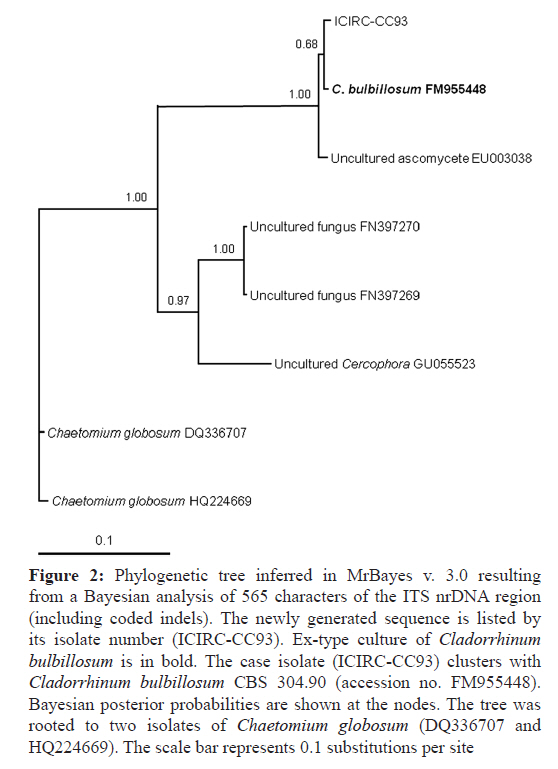
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 434-437 Case Report Severe pigmented keratitis caused by Cladorrhinum bulbillosum DU Gajjar1, AK Pal2, JM Santos3, BK Ghodadra4, AR Vasavada4 1 Scientist, Iladevi Cataract and IOL Research Centre, Ahmedabad, India Date of Submission: 19-Aug-2011 Code Number: mb11106 PMID: 22120812 Abstract We report a case of severe pigmented keratitis with poor prognosis, caused by Cladorrhinum bulbillosum. Antifungal treatment with topical natamycin and fluconazole eye drops and oral tablet fluconazole failed to heal the ulcer and resulted in perforation. The causative fungus, C. bulbillosum, was identified on the basis of its typical microscopic features and 98% sequence homology to ex-type isolate CBS 304.90 (accession no. FM955448). The results of an in vitro antifungal susceptibility test indicated that the isolate was susceptible to natamycin, amphotericin B, fluconazole and itraconazole. The present case is the third case of keratitis and the second case of human keratitis. Compromised immunity due to liver cirrhosis could lead to a failed prognosis even when the fungal isolate is highly susceptible to antifungal treatment. Keywords: Cladorrhinum bulbillosum , pigmented keratitis, liver cirrhosis Introduction Pigmented dematiaceous fungi are the third most common cause of mycotic keratitis. [1],[2] Curvularia spp. are the most common fungal species isolated from pigmented keratitis and other species like Bipolaris, Exserohilum, Cladosporium, Lasiodiplodia, Alternaria, Torula, Aureobasidium, Nigrospora and Epicoccum have also been reported. [2],[3] Here, we report a typical severe case of dematiaceous fungal keratitis caused by Cladorrhinum bulbillosum. Case Report A 42-year-old male farmer presented in the outpatient department of the ophthalmology clinic with a history of severe painful tearing, redness and dimness of vision in the right eye since 10 days. Although the patient was a farmer, he did not recall any incident of intrusion of a foreign body in the eye or any ocular trauma. The patient was on medication for liver cirrhosis since the last 6 months and was alcoholic since the past 20 years. The details of the medication used for liver cirrhosis were not available. On examination, the right eye showed perception of light in the upper and nasal quadrants only. The lids showed high oedema and the conjunctiva showed high circumciliary congestion. A photo slit lamp examination revealed that the ulcer was covering the entire cornea except the limbus [Figure - 1]a. The size of the ulcer was around 8-9 mm vertically and 9 mm horizontally with irregular margins. The upper half of the lesions showed a reddish brown pigment with complete stromal infiltration reaching up to the endothelium. Thick and cheesy hypopyon was also present at a depth of about 2 mm. The details of the anterior chamber were not visible as the corneal abscess was covering the entire cornea. Tension was observed to be digitally high. The left eye was normal. Corneal scrapings were taken from the right eye and the media were inoculated for bacterial culture, fungal culture, KOH mount and Gram staining. The 10% KOH mount showed plenty of pigmented fungal filaments that were highly septate with irregular margins [Figure - 1]b. Gram staining showed prominent septate, branched fungal hyphae and absence of bacteria. A provisional diagnosis of fungal ulcer was made and antifungal treatment was initiated with topical natamycin eye drops (Natamet; 5% suspension, Sun Pharmaceuticals Ind. Ltd, Halol, India), vigamox eye drops (Moxifloxacin; 0.5% suspension, Alcon Laboratories Inc., Texas, USA), fluconazole eye drops (Zocon; 0.3% suspension, FDC Ltd, Aurangabad, India) hourly, and atropine eye drops (Atropine, 0.1% suspension, Taj Pharma Ltd, Mumbai, India) three times a day. The patient was also prescribed tablet Iopar (250 mg to reduce IOP) and an antifungal tablet fluconazole (150 mg) once a day. The nutrient agar plate and blood agar plate inoculated with scraping material showed growth of several colonies of a single fungus within 2 days. The following week, the patient was relatively comfortable but no change was noted in the size of the infiltrate. The therapy was continued. Unfortunately, there was no further improvement and his compliance continued to be poor for another 2 months. At each presentation, he was placed on a topical and systemic antifungal regime. The very poor prognosis and the need for therapeutic keratoplasty were explained to the patient. However, the patient declined keratoplasty. After 2.5 months, the patient complained of severe pain. An examination revealed corneal perforation and a flat anterior chamber. The patient was referred to a government hospital due to financial reasons and since then lost to follow-up. Mycological studies The case isolate (ICIRC-CC93) was subcultured on Sabouraud′s Dextrose Agar (SDA) (Himedia Labs Ltd, Mumbai, India) and rice agar (prepared in the house) and inoculated at 25°C and 37°C. The fluffy, pure fungal growth was brown in the middle and white at the periphery. Colonies were fast growing reaching a diameter of 68-80 mm within 4 days at 25°C and at 7 days they reached the edge of the Petri dish. After 10 days, they turned dark brown [Figure - 1]c. The pure fungus from the SDA plate was mounted with lactophenol cotton blue stain. Septate filaments were observed, and in a few fields, microsclerotia were also observed. The fungus was identified as Cladorrhinum spp. by its morphological and microscopic features. A microscopic picture of several microsclerotia is shown in [Figure - 1]d. The average length of a single microsclerotium is 160 mm. Microsclerotia seen at a higher magnification showed compact aggregations of hyphae composed of swollen, pigmented cells [Figure - 1]e. Rarely, flask-shaped, lateral conidiogenous cells measuring up to 11.57 mm were also seen [Figure - 1]f. For identification of the fungus, sequencing of the ITS (internal transcribed spacer) region was done. The DNA was extracted from the fungus using cetyltrimethylammonium bromide (CTAB) buffer. Sequencing of the ITS region was done at First Base Laboratories Sdn. Bhd, Malaysia, using primers ITS1 (F-5′-TCCGTAGGTGAACC-3′) and ITS4 (R-5′TCCTCCGCTTATTGATATGA-3′), which amplify the following genes of the fungal genome: Partial 18S rRNA gene, complete ITS1, 5.8S rRNA gene and ITS2 regions, and partial 28S rRNA gene. Sequencing of the LSU region, using the MicroSeq D2-LSU rDNA fungal identification kit (Applied Biosystems, CA, USA), was done at the sequencing facility of Gujarat State Biotechnology Mission (GSBTM), Government of Gujarat, India. The ITS and LSU sequences were submitted to the NCBI database. The ITS sequence of the case isolate (ICIRC-CC93) showed 98% sequence similarity to C. bulbillosum CBS 304.90 (accession no. FM955448) with a BLAST search expect value of zero. The 98% match indicated that the isolate was representative of C. bulbillosum. The D2-LSU sequence showed a maximum similarity score of 98% with Cercophora costaricensis (accession no.AY780059) with an expect value of 5E -12 . A Bayesian phylogenetic tree was built using MRBAYES (version 3.0). The adjoining ITS tree clearly clusters the present case isolate with the ex-type isolate of C. bulbillosum (CBS 304.90) [Figure - 2]. In vitro antifungal susceptibility testing In vitro antifungal susceptibility testing was done against natamycin (Natamet; 5% suspension; Sun Pharmaceuticals Ind. Ltd, Halol, India), itraconazole (Itral; 1% suspension; Jawa Pharmaceuticals, Gurgaon, India), fluconazole (Nuflucon; 0.3% suspension; NuLife Pharmaceuticals, Pune, India), and amphotericin B (RM 462, Himedia Labs Ltd, Mumbai, India) using the microdilution method and by following CLSI guidelines. All antifungal agents were dissolved in DMSO and amphotericin B was dissolved in water. The inoculums were prepared by covering the 7-day-old culture plate with 0.85% normal saline. This was followed by gentle probing of the colonies with the help of a pipette and adjusting the densities of the suspension (read at 530 nm) to a final inoculum of 0.5 McFarland standard. The final drug concentration ranges were 0.008 to 32 μg/ml for all the four antifungal agents. All the antifungal agents were tested in RPMI 1640 media with 2% glucose and without sodium carbonate. The results of the in vitro antifungal susceptibility test indicated that the MIC was 0.064 mg/ml for natamycin and amphotericin B, 0.016 mg/ml for fluconazole and <0.016 mg/ml for itraconazole. Discussion Here, we report a severe case of pigmented fungal keratitis caused by an endophytic fungi C. bulbillosum. Cladorrhinum spp. are found mainly on dung and plant material in the soil as saprobes. [4] C. bulbillosum belongs to the Lasiosphaeriaceae family of the order Sordariales. There are almost 29 genera found in this family including Cladorrhinum. Out of those 29 genera, only 2 are found to be pathogenic to human, namely Cladorrhinum and Arnium. [5],[6],[7] In the genus Cladorrhinum, C. bulbillosum is the only reported pathogenic species causing keratitis with only two reported cases so far. The first case of keratomycosis by Cladorrhinum spp. was reported in a 12-year-old Argentinean boy who was working with horses in 1979 (strain CBS 604.75) [7] and the second case was reported in a Percheron cross horse in 1997. [5] The earlier case was later described as the new species C. bulbillosum by Mouchacca and Gams. [8] Cladorrhinum species were mainly distinguished on the basis of their ability to produce microsclerotia, the conidial shape, and more importantly the tufted aggregation of the conidiophores. Our case isolate of C. bulbillosum (ICIRC-CC93) had all the morphological characteristics typical of this species and also clusters along with the ex-type isolate of C. bulbillosum in the adjoining phylogenetic tree. The evolutionary relationship between Cladorrhinum species and other ascomycetes is not very clear. In a recent paper describing two new species of Cladorrhinum, the authors very efficiently discuss the phylogenetic placement of this genus. [4] So far, none of the other species of Cladorrhinum are associated with any human or animal disease. Both the above-mentioned cases were successfully treated using miconazole antifungal agent although a therapeutic keratoplasty was performed on the horse. The present case showed poor prognosis, in spite of good in vitro antifungal activity of all the four tested agents. Our patient was on medication for liver cirrhosis and so the poor prognosis may be attributed to the patient′s immuno-compromised condition. Both liver cirrhosis and alcoholism are well-established reasons for compromised immunity. Patients with liver failure are at risk of incurring bacterial and fungal infection. Endogenous endophthalmitis after liver transplantation and ocular surface damage in patients with chronic hepatitis has been reported. [9] Further, the failure of the treatment can also be attributed to the fact that the patient may not have strictly followed the prescribed drug regime. Previously, in a case series on amniotic membrane transplants, in cases of recurrent and perforated corneal ulcers, three cases of keratitis with liver cirrhosis were shown to be perforated during treatment. [10] However, since this is the second reported case of C. bulbillosum keratitis, all possibilities remain hypothetical. In summary, this case illustrates the vulnerability of the cornea to infrequent organisms and further highlights the importance of the patient′s immune system parallel to the treatment regime in combating infection. Nucleotide Sequence Accession Numbers The GenBank accession numbers for the case isolate Cladorrhinum bulbillosum (ICIRC-CC93) are JF758870 (ITS) and JN107807 (D2-LSU). Acknowledgments DG thanks the financial support from the WOS-A grant (No. SR/WOS-A/LS-120-2008) of Department of Science and Technology, India. The authors thank Dr. Hugo Madrid, Unitat de Microbiologia, Facultat de Medicina i Ciθncies de la Salut, IISPV, Universitat Rovira i Virgili, C/ Sant Llorenc 21, 43201 Reus, Tarragona, Spain for his help in identification of the isolate. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11106f2.jpg] [mb11106f1.jpg] |
| |||||||||

{kind=link}
{kind=link}