 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
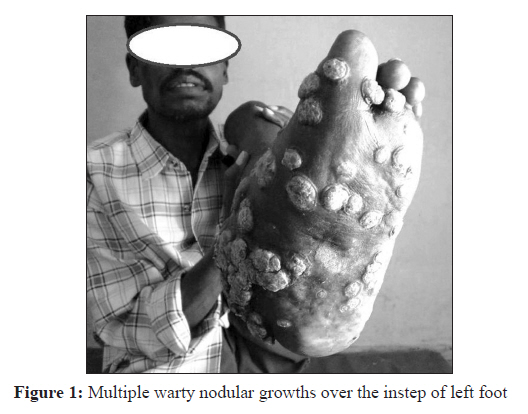
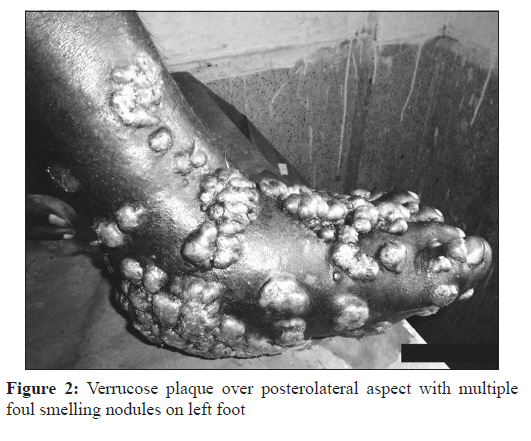
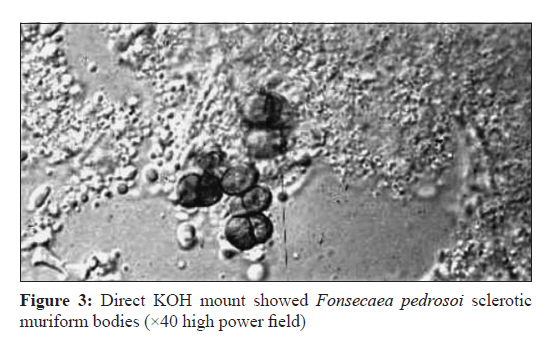
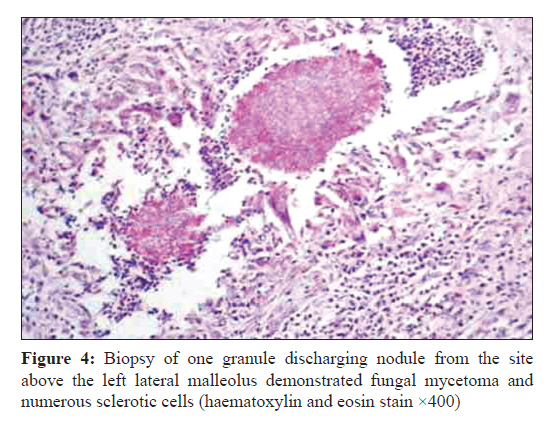
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 437-439 Case Report Concurrent mycetoma and chromomycosis R Murthy1, JP Swain2 1 Department of Microbiology, Chhattisgarh Institute of Medical Sciences, Bilaspur, Chhattisgarh, India Date of Submission: 29-Apr-2011 Code Number: mb11107 PMID: 22120813 Abstract Chromoblastomycosis and Madura foot are chronic localised mycotic infection of the skin and subcutaneous tissue that follows the implantation of the fungi through minor trauma, mainly found in persons working outdoors on bare foot. In cases where both Madura and chromoblastomycosis are present, the treatment becomes difficult with low cure rates and frequent relapses. Here, we present such a very rare case of a 38-year-old cattle farmer who presented with verrucose nodules, tumefaction and multiple discharging nodules on the left lower 1/3 rd leg and foot since last 9 years. Direct KOH mount of the verrucose tissue showed Fonsecaea pedrosoi sclerotic muriform bodies and a biopsy of one granule discharging nodule demonstrated fungal mycetoma. He was put on tab. Itraconazole 200 mg o.d. and cotrimoxazole bid for 6 months with very little improvement. The rarity of this combination is most probably due to different geographical distribution. Keywords: Chromoblastomycosis, Fonsecaea pedrosoi , Madura foot, sclerotic bodies, pseudoepitheliomatous hyperplasia Introduction Chromoblastomycosis (also known as ′Chromomycosis′, ′Fonseca′s disease′) is a chronic fungal infection of the skin and subcutaneous tissue that follows the traumatic implantation of the aetiologic agent. [1],[2] The infection occurs most commonly in tropical or subtropical climates, often in rural areas mainly found in persons working outdoors [2],[3] and also the same for Madura foot. [4] They can be caused by different types of fungi which become implanted under the skin, often by thorns or splinters. Although both the deep mycotic infections are commonly seen among workers in rural areas with bare foot, but usually one infection occurs in one person. Here, we present a case harbouring concurrent mycetoma and chromomycosis. Case Report A 38-year-old cattle farmer from a remote village of Chhattisgarh sought medical attention in our hospital for tumefaction with multiple verrucose and discharging nodules on the left foot and lower 1/3 rd of leg on left side since last 9 years. He first developed small warty growths over the instep of left foot [Figure - 1]; subsequently, multiple satellite dirty warty nodular lesions continued to appear slowly over a long period gradually attaining the present size [Figure - 2]. Physical examination showed very firm tumefaction; large verrucose plaque on postero-medial aspect with numerous foul smelling discharging nodules [Figure - 2] and some nodules had white granular discharge. Systemic examinations showed no abnormality. Routine laboratory blood and urine investigations were within normal limits. Direct KOH mount of tissue scraping from the verrucose growth showed the pathognomonic Fonsecaea pedrosoi sclerotic muriform (Medlar) bodies [Figure - 3] intermediate between the yeast and hyphal forms. [1] Mycological culture studies were not done for this case. Histopathology examination after taking a biopsy of one bigger granule discharging nodule [Figure - 2] from the site above the lateral malleolus had features of fungal mycetoma i.e. pseudoepitheliomatous hyperplasia with abscess cavities in the dermis containing sulfur granules that showed a gram-positive reaction and numerous sclerotic cells with marked epidermal acanthosis [Figure - 4]. [4],[5] From the above clinical features and laboratory findings, he was diagnosed a case of concurrent mycetoma and chromomycosis. Due to extensive involvement and tumefaction, both surgical and antifungal treatments were proposed, but the patient refused to undergo surgery for debridement. He was prescribed with tablet Itraconazole 200 mg o.d. and cotrimoxazole bid for 6 months with little improvement, but unfortunately later we came to know that he was arrested on criminal charges and thus we lost follow up. Discussion Chromoblastomycosis is a slowly developing chronic granulomatous fungal infection, which characteristically produces pigmented hard yeast cells called muriform cells or sclerotic bodies [2] and belong to the group of fungal infections called phaeohyphomycosis caused by dematiaceous (pigmented) fungi. Because of their natural pigmentation, the sclerotic bodies can be easily identified in unstained sections. Fonsecaea pedrosoi is the most common agent of chromoblastomycosis. The diagnosis of chromoblastomycosis mostly relies on the identification of brown coloured ′sclerotic bodies′ or ′muriform cells′ (hence the name). Special stains such as Fontana Masson and Gomori′s methenamine silver nitrate are useful for demonstration. Release of pathogenic sclerotic bodies by transepithelial migration and their autoinoculation and or lymphatic spread could explain the ′satellite′ lesions. For chromoblastomycosis there are several treatment options [6] with variable cure rates, but in cases where both Madura and chromoblastomycosis present it becomes very difficult for treatment with low cure rate and frequent relapses. The prognosis is very good for small lesions. Severe cases are difficult to cure although the prognosis is still quite good. Generally, mycetoma is more commonly seen than chromoblastomycosis. But the rarity of this combination of diseases, despite their common contamination mode is due to different geographical distribution with mycetoma being found in the southern east India region and chromomycosis in the humid central India region. These mycotic infections are highly prevalent in hot and humid climate; found everywhere in soil, decaying vegetation and rotten wood which frequently served as the point source of infection [2] and believed to originate in minor trauma to the skin, usually from vegetative material such as thorns or splinters. This trauma implants fungi in the subcutaneous tissue. The disease frequently involves lower extremities of barefooted adult rural men involved in agriculture or cattle related works. [2],[3] In many cases the patient will not notice or remember the initial trauma, as symptoms often do not appear for years. Although these mycoses slowly spread, they usually remain localized to the skin and subcutaneous tissue. Haematogenous and/or lymphatic spread may occur. Multiple nodules may appear on the same limb, sometimes coalescing into a large plaque. Secondary bacterial infection may occur, sometimes inducing lymphatic obstruction. In this case the patient′s village is on the southern Chhattisgarh zone which comes close to Andhra Pradesh bearing mixed climate. As he belonged to a very remote jungle area village with poor medical facility, he could not seek proper consultation at right time and depended upon the village quacks taking herbal medication and continuing his profession on bare foot for a long period on damp jungle area, thus it resulted in the acquirement of both deep mycotic infections. There is no known preventative measure aside from avoiding the traumatic inoculation of fungi. [2] References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11107f3.jpg] [mb11107f4.jpg] [mb11107f2.jpg] [mb11107f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}