 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
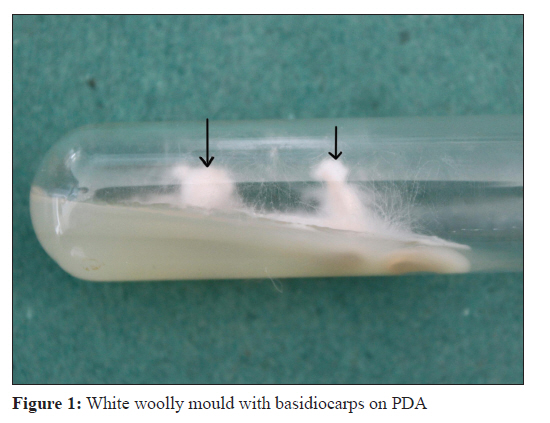
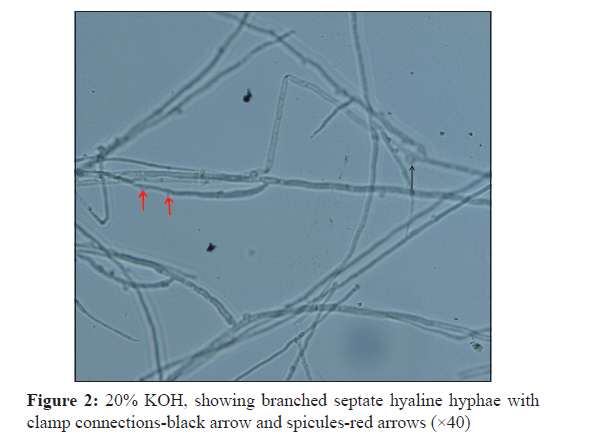
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 439-442 Case Report Schizophyllum commune sinusitis in an immunocompetent host B Swain1, R Panigrahy1, D Panigrahi2 1 Department of Microbiology, Institute of Medical Sciences and SUM Hospital, SOA University, Kalinga Nagar, Bhubaneswar, Odisha, India Date of Submission: 10-Jun-2011 Code Number: mb11108 PMID: 22120814 Abstract Schizophyllum commune is widely distributed in the nature, but it rarely causes human infection. We have isolated this mould in a 46-year-old immunocompetent, non-diabetic patient with chronic sinusitis, previously treated with multiple antibiotics and topical steroid nasal drops with no response. Materials obtained from the nasal sinus during the endoscopic surgery, on KOH mount and histopathological study revealed broad septed hyaline hyphae. Growth on the Sabouraud's dextrose agar and potato dextrose agar produced white moulds with microscopic and macroscopic characters of S. commune. Till date there are few reports of S. commune sinusitis in immunocompetent individuals Worldwide. This is the first reported case in India to the best of our knowledge. Keywords: Fungal Sinusitis, immunocompetent, schizophyllum commune Introduction Fungal infection of the paranasal sinuses is uncommon. However, its incidence in recent years has shown marked increase especially in North Sudan, South Western states of USA and in North India. [1] Most of the fungi causing sinusitis are common saprobes. Although Aspergillus species are the major aetiological agents, the fungi like Alternaria, Curvularia and Bipolaris are also reported to cause sinusitis. [2] There are reports of emerging role of Schizophyllum commune in pulmonary disease, ulcerative lesions of the palate, atypical meningitis, cerebral abscess, chronic or allergic sinusitis and possible onychomycosis from different countries. [2],[3],[4],[5],[6] This fungus is a mould of Phylum Basidiomycota, Schizophyllaceae family, has a worldwide distribution that colonizes diverse trees and rotting woods. These are well-known fungi, having been reported as plant pathogen from 150 countries except Antarctica, some are mycorrhizal fungi, and others are saprobic. Only few of them are harmful to humans upon ingestion because of the toxin (hallucinogenic compounds) they contain. Infections originated from this fungus are rare in humans. [7] Chronic or allergic sinusitis caused by this fungus is reported in immunocompromised patients either due to prolonged antibiotic intake, steroid therapy or with under-laying diseases like diabetes, AIDS and malignancy. [3],[7] Only few cases are reported in immunocompetent individuals. [7],[8] We report a case of S. commune sinusitis involving paranasal sinuses in an immunocompetent adult female; a rare case from India. Case Report A 46-year-old housewife from urban background, presented with 1 year history of discomfort over her left frontal and maxillary sinuses. This was associated with anosmia and a left-sided purulent anterior nasal and postnasal discharge. She had taken many antibiotics at different occasions by many physicians with minimal symptomatic improvement. There was no history of previous surgery, facial trauma, distant travel or drug abuse. Physical examination noted purulent discharge in the left middle meatus. The right middle meatus was clear. Examination of her head and neck did not reveal any abnormality. Her haematological parameters were within normal limits. Her tests for diabetes and HIV were negative. The chest X-ray finding was unremarkable. A plain X-ray of paranasal sinuses showed a nodular mucosal thickening and the absence of air/fluid levels with homogenously cloudy maxillary and ethmoidal sinuses, without bony destruction. A bone density computerized tomography (CT) scan of her sinuses showed polypoidal soft tissue attenuation lesion completely filling bilateral ethmoidal sinuses, and mucosal thickening of left maxillary antrum. There was intact bony wall of paranasal sinuses. This gave the impression of left maxillary sinusitis with bilateral ethmoidal polyposis. She was given a week course of amoxycillin and was subjected to endoscopic surgery. The frontal sinus was found to be normal. The nasal polyps from both ethmoidal sinuses and blackish material (necrotic debris) from the left maxillary sinus were removed. This material was subjected to histopathological test and microbiological examinations. Routine tests for bacterial aetiology was done with Gram′s stain and cultured on the MacConkey agar, sheep blood agar and chocolate agar. To exclude tuberculosis, ZN stain was done from the material and cultured in LJ media in two sets. Simultaneously, the specimen was examined for fungus using 20% KOH and cultured in two sets at 22°C and 37°C respectively for fungal isolation on Sabouraud′s dextrose agar (SDA) tubes containing gentamicin and SDA medium containing cycloheximide in the Mycology Lab. The surgical specimen yielded negative results for pathogenic bacteria and mycobacteria both by microscopy and culture. Histopathology and KOH preparation from the surgical specimen showed hyaline septate hyphae with few dichotomous branching. The fungal culture at 22°C and 37°C on Sabouraud′s dextrose agar containing gentamicin yielded white to pale buff, densely woolly fungus with a pale-brown reverse in 2 weeks producing a strong disagreeable odour. There was no growth on medium containing cycloheximide. A white buff, densely woolly fungal growth was seen on potato dextrose agar medium (PDA). Sub-cultured both on tubed SDA containing gentamicin and PDA kept with a light source, the mould formed macroscopic white, tube-shaped, leathery basidiocarps at the colony periphery in 4 days [Figure - 1]. Microscopic examination of the mould by teased mount both in KOH and lacto-phenol cotton blue preparation showed hyphae of various widths and some of these had small peg like projections (spicules) with clamp connections [Figure - 2]. The isolate was kept for several months and sub-cultured on different media but it failed to sporulate under all conditions. From the above microscopic and macroscopic features, the isolate was identified as S. commune. To identify the fungus from another source, it was sent to Mycology Division, Dept. of Microbiology, the Centre for National Culture Collection of Pathogenic Fungi (NCCPF-A National facility supported by ICMR, New Delhi), PGIMER, Chandigarh. It also gave the same result for this fungus as S. commune with Reference no-1, Isolate no. II-254/Date-12.1.2011. Considering from different mycological studies of the isolate, clinical history and radiological finding of the patient, it was diagnosed as a case of chronic non-invasive fungal sinusitis of S. commune aetiology. No antifungal treatment was given during post-operative period. There was dramatic resolution of her symptoms by 1 week with surgery and cavity took 4 weeks to heal with no evidence of residual infection. Follow up at 3 months showed complete clearance of the disease. Discussion S. commune occurs worldwide on a wide range of dead deciduous trees and uncommonly on vegetation such as hay, where its fan-shaped basidiocarps are easily identified. [9] Although S. commune is ubiquitous in nature, there are only rare reports of its association with human infections, including those of the brain, lungs and mouth. [4],[5],[6] Animal studies have shown that S. commune is a fungal agent of relatively low virulence causing a progressive low-grade infection, with death occurring in some very young animals, and in which the progress of infection is influenced by the age of the host, the size of the inoculum, and prior treatment with an immunosuppressive agent. [4] Fungal sinusitis is a rare entity that has increased in recent years in immunocompetent individuals. It reveals three clinical manifestations: Allergic, chronic non-invasive and invasive. The allergic manifestation involves immunocompetent patients and it is characterized by allergic mucin with eosinophils and Charcot-Leyden crystals, as well as increased serum IgE. The chronic non-invasive manifestation affects immunocompetent individuals, and does not cause mucosal or blood vessel invasion. The invasive manifestation occurs in immunocompromised individuals with tissue and vascular invasion. [10] In our case, the fungus isolated was S. commune. Both the X-ray and CT scan of paranasal sinuses showed no bony destruction with intact intersinus septa in ethmoid labyrinth which is an important finding in favour of non-invasive form of fungal sinusitis. [11] She was an immunocompetent individual. The common pathway in the conversion of these ubiquitous organisms from saprobic to pathogen state may be due to sinus obstruction by the bilateral nasal polyps with impaired ventilation. The patient was also from a warm and dry climate which may also favours the fungal sinusitis. Fungal sinusitis has been described as a disease process that primarily affects young male farmers, [1] in contrast in our case she was an adult housewife of urban background. Further study may be required for different contributing factors to the human pathology by the S. commune. Schizophyllum commune is infrequent as cause of pathologies. Clinically and in the laboratory, confusion with Aspergillus infection can occur in the initial presentation and the microscopy of the specimen. Because the hyphae of this basidiomycete may appear similar to those of Aspergillus species in the surgical material, accurate diagnosis of S. commune infection relies on recognition of the fungus in culture. S. commune can be identified with reasonable certainty in culture by observing narrow and wider type of hyphae with small lateral projections, spicules or tubercle [Figure - 2]. Nobles [12] considered that these structures are always present and are diagnostic for the species, but they are easily overlooked. A typical hypha has a clamp connection [Figure - 2] at every septum. Based on her observations, she defined the cultural characteristics of many basidiomycetes. Clinical laboratories should not overlook basidiomycetes as potential opportunistic pathogens. It is likely that infections caused by S. commune are misdiagnosed or are not recognized because of the lack of familiarity of clinicians with this fungus and the difficulty many laboratories may have in identifying this basidiomycete. Any white, rapidly growing, sterile isolate with septate hyaline hyphae should be suspected as S. commune if (i) it grows well at 37°C; (ii) it forms a dense, tough (i.e., difficult to cut), woolly colony; (iii) it is susceptible to cycloheximide (400 mg/ml); (iv) it tolerates benomyl (2 mg/ml); and (v) it has a pronounced and disagreeable odour. Confirmatory findings include (i) the presence of spicules on some hyphae, (ii) the presence of clamps at some septa and (iii) formation of fan-shaped basidiocarps when grown in the light. [3] In this case, the patient was cured with intervention of the paranasal sinuses and drainage which is considered the therapy of choice for maxillary fungal sinusitis. However, the optimal treatment for infections caused by S. commune is not well established, because of the few cases and it is difficult to determine the adequate therapy. This patient was not treated with any antifungal drugs. However, some reports in the literature have shown that the effectiveness for the surgical procedure; and administration of amphotericin B or fluconazole [10],[13] in the treatment of S. commune. It is worth noting that the lack of familiarity with S. commune, may lead Microbiologists and clinicians to consider it as a contaminant without importance although the basidiomycetes must be kept present as potential pathogens. Given that this fungus may be isolated from the environment, culture by itself is not diagnostic. To attribute pathogenicity of S. commune, it must be isolated and accompanied by identification of the fungal structures. Certainty the diagnosis is more when direct examination of the organism is confirmed. Correct diagnosis will avoid unspecific treatments, chronicity of the illness or complications to the patients. Acknowledgements The authors express their gratitude to Professor Dr. Arunaloke Chakrabarti, Dept. of Microbiology, PGIMER, Chandigarh, India, for identification of the fungus. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11108f1.jpg] [mb11108f2.jpg] |
| |||||||||
{kind=link}
{kind=link}