 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
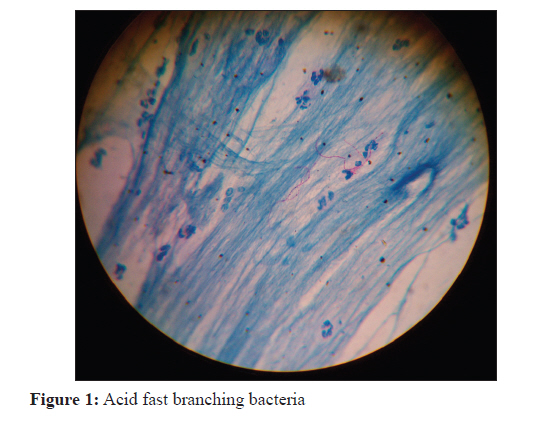
Indian Journal of Medical Microbiology, Vol. 29, No. 4, October-December, 2011, pp. 446-447 Correspondence Primary pulmonary infection caused by 20% acid fast Nocardia brasiliensis V Rawat1, Umesh1, N Thapliyal2, DC Punera3 1 Department of Microbiology, Govt. Medical College, Haldwani (Nainital), Uttarakhand, India Date of Submission: 13-Jun-2011 Code Number: mb11113 PMID: 22120819 Dear Editor, Nocardiosis is a rare localized or systemic infection caused by several species of the genus Nocardia. This genus consists of strictly aerobic, Gram-positive, variably acid-fast, filamentous bacteria with a tendency to fragment into bacillary and coccoid forms. [1] N. asteroides, N. farcinica, N. nova (included in the N. asteroides complex) and N. brasiliensis are the species most often involved in human disease. [1],[2] N. brasiliensis has been recovered from the soil in many tropical and subtropical areas but rarely in temperate areas. The microbiological identification of Nocardia isolate is based on microscopic examination and physiological tests. Partial acid fastness differentiates it from Actinomyces and related species which are usually not acid fast. [1] We report Recovery of a 20% acid fast isolate of N. brasiliensis from patient with primary pulmonary nocardiosis is an unusual finding in this case. A 65-year-old man, farmer by occupation, presented with history of fever for the last 1 month and productive cough for last 2 months. The patient was earlier diagnosed as a case of chronic obstructive pulmonary disease. On examination, his temperature was 39.2°C; pulse, 108/min.; BP, 110/86 mmHg and respiratory rate, 40/min. On auscultation of chest, crepitations and rhonchi were found in right infraclavicular area and lower axillary area. Laboratory studies revealed: Haemoglobin, 11.8 g/dL; total leucocyte count, 13800/mm 3 , P86, L12, E-02 and erythrocyte sedimentation rate 75 in first hour. Roentgenogram of chest showed cavity on right lower lobe and consolidation on right apex. Patient was suspected as a case of tuberculosis and sputum sample was sent for Ziehl Neelsen (ZN) staining and culture. Sputum ZN staining was performed using 20% H 2 SO 4 . Red coloured thin-beaded filamentous bacteria with right-angled branching resembling Nocardia spp. were found on sputum smear microscopy [Figure - 1]. Repeat sample yielded similar findings. The sample was cultured on blood agar and MacConkey agar. After 24 h incubation, moderate growth of Klebsiella spp. and scanty growth E. coli were observed. On further incubation after 48 h, white dry colonies were seen on blood agar and MacConkey agar. Growth was confirmed as Nocardia spp. based on microscopic morphology. Klebsiella could have been secondary invader and E. coli could be transient coloniser of throat. However, antimicrobial sensitivities for amoxicillin, ampicillin plus clavulanic acid, cefotaxime piperacillin-tazobactam, ciprofloxacin and amikacin were performed for both of these organisms and common sensitivity was found for cefotaxime. For confirmation of the species of Nocardia, the isolate was sent to Sanjay Gandhi Post Graduate Institute, Lucknow (India). It was identified as Nocardia spp. on the basis of microscopic morphology and growth in lysozyme broth. N. brasiliensis was confirmed on biochemical characterisation. It was catalase positive, decomposed casein, hypoxanthine, tyrosine but not xanthine. [3] Molecular confirmation could not be done due to lack of facility in our Institute. The isolate was resistant to amoxicillin, ampicillin plus clavulanic acid, erythromycin, piperacillin-tazobactam and ciprofloxacin. It was sensitive to amikacin, gentamicin, tobramycin, chloramphenicol, tetracycline and to co-trimoxazole. The patient was put on amikacin and cefotaxime for 15 day. The patient responded clinically. The clinical end points were freedom from fever, which was achieved after 2 weeks of treatment with reduction in purulence of sputum. Following 2 weeks of treatment, repeat ZN stained sputum smear on microscopy showed 20% acid fast branching bacteria. Oral co-trimoxazole was started, 10 mg/kg/day and continued for a total of 6 months . Patient hailed from interior of Kumaun region and expressed his inability to come every month and reported only after 6 months. After 6 month of treatment, microscopic sputum examination did not show acid fast branching bacteria and radiological improvement with complete resolution was observed. Pulmonary infection due to N. brasiliensis is almost always associated with direct extension from mycetoma through chest wall. [4] Primary pulmonary infection due to N. brasiliensis is rare although cases of primary pulmonary infection by N. brasiliensis have been reported. [4],[5] In our case also there was no chest wall mycetoma found and N. brasiliensis was the cause of primary pulmonary infection, but unique feature of our isolate was 20% acid fastness. To the best of our knowledge, this is the first case of Nocardia spp., which is 20% acid fast. During the course of routine identification, laboratory specialists should be aware of the occasional occurrence of atypical strains of N. brasiliensis. Acknowledgement The authors thank Dr. Rugmei Marik, Associate Professor of Microbiology, Sanjay Gandhi Post Graduate Institute, Lucknow for confirming the identification of isolate as Nocardia brasiliensis. References
Copyright 2011 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb11113f1.jpg] |
| |||||||||

{kind=link}