 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
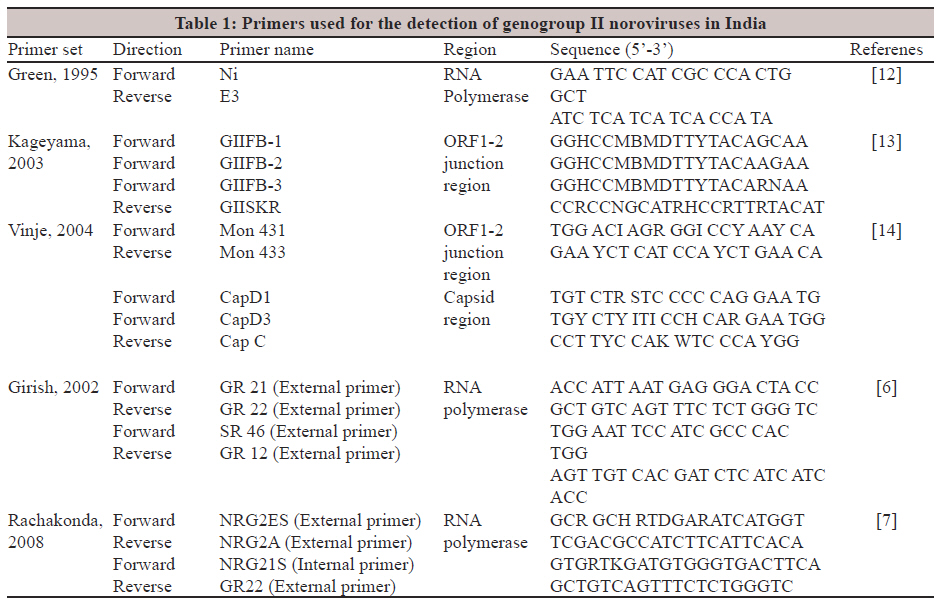
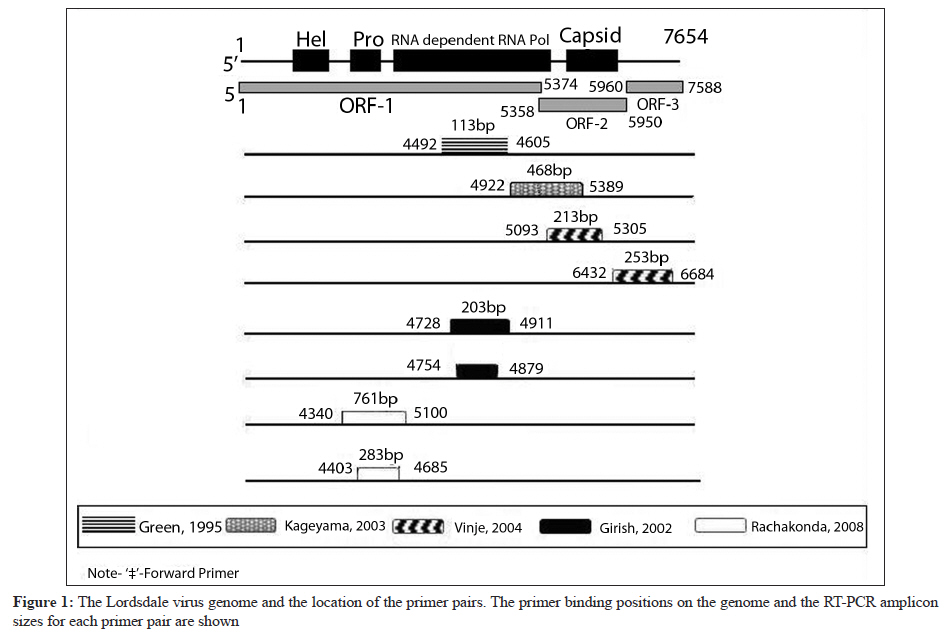
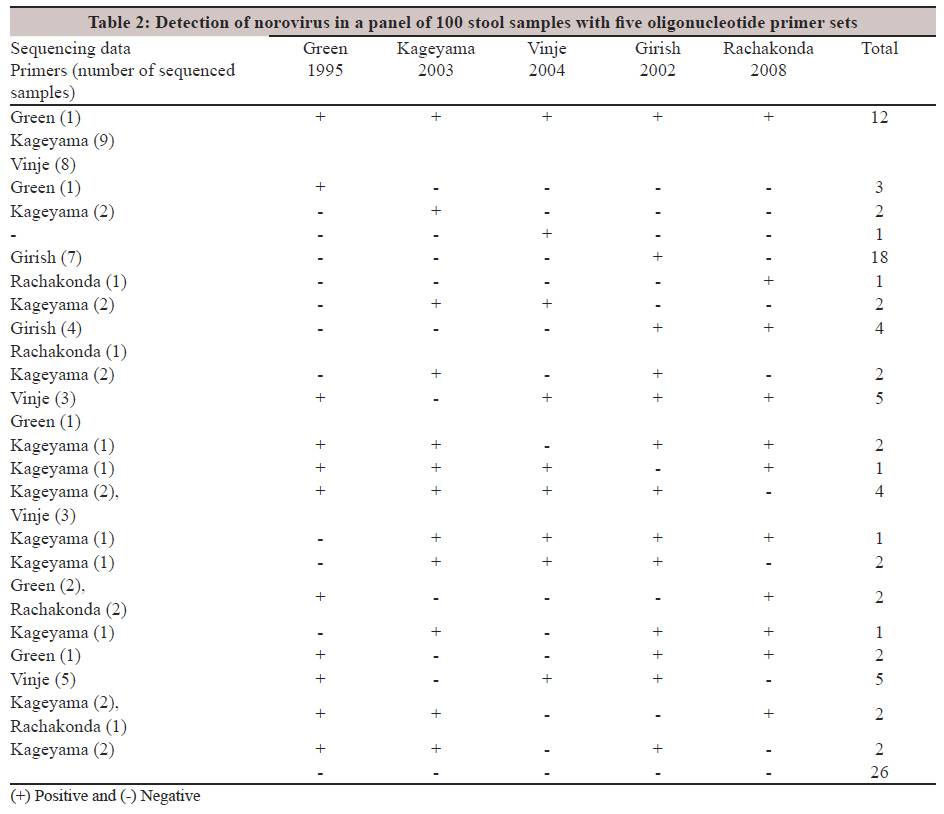
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 24-29 Original Article Comparison of primers for the detection of genogroup II noroviruses in India S George, VK Menon, S Ramani, G Kang Department of Gastrointestinal Sciences, Christian Medical College, Vellore - 632 004, India Correspondence Address: Date of Acceptance: 21-Nov-2011 Code Number: mb12005 PMID: 22361756 DOI: 10.4103/0255-0857.93016 Abstract Purpose: Noroviruses (NoV) are increasingly recognized as an important cause for acute gastroenteritis, worldwide. Reverse transcription polymerase chain reaction (RT-PCR) and sequencing are the methods of choice for the detection of NoVs, but there is currently no consensus about the primers to be used in these assays. Keywords: Genogroup II, India, norovirus, primer comparison Introduction Noroviruses (NoV) are small, single-stranded, non-enveloped, positive sense Ribonucleic acid (RNA) viruses, belonging to the family Caliciviridae with a genomic size of approximately 7.5 kb. [1] The viral genome consists of three open-reading frames (ORFs), with ORF1 encoding six non-structural proteins, including the RNA-dependent RNA polymerase (RdRp) required for the replication of the virus. ORF2 codes for the major structural capsid protein, while ORF3 codes for a minor structural protein required for stabilising the capsid. [2] There are currently five different NoV genogroups (G) GI - GV, of which GI, II, and IV infect humans. [1] GII NoV has been found to be the most prevalent among the human infectious NoVs around the world, with NoV GII.4 being the dominant strain. [2] Epidemiological studies of sporadic cases and outbreaks of gastroenteritis show that NoV GII is a common cause of gastroenteritis in all age groups. [3] The viruses are transmitted through faecally contaminated food or water and by direct person-to-person contact. The major tools for detection and characterisation of NoVs are reverse transcription polymerase chain reaction (RT-PCR) and sequencing. [4] The RdRp and capsid regions of the NoV genome contain highly conserved motifs, which are targeted for the detection and genotyping of the virus. [4] However, there is great variability in the rates of detection across different populations with circulating genotypes, varying by year and locale, partly due to the evolution of new virus genotypes by recombination, resulting in an enormous genomic diversity. [5] Although a large number of primers have been designed to detect NoVs, there is currently no consensus about the most suitable primer pair for the detection of the viruses. [5] There are few reports of NoVs in the Indian population. [6],[7],[8],[9],[10],[11] Even as these studies highlight the differences in rates of detection and genotype circulation in different parts of the country, it must be noted that there is variability in the populations examined, methods, and primers used for the detection and characterisation of noroviruses. The primary objective of this study was to identify the most suitable primers for the detection of GII NoVs in children with diarrhoea in this region. Five sets of published oligonucleotide primers including three primer sets used widely across the world and two primer sets used elsewhere in India were evaluated, using a panel of 100 stool samples. Materials and Methods Polymerase chain reaction primers for detection of noroviruses The primer sets were classified into five groups for the purpose of comparison - Green 1995,[12] Kageyama 2003, [13] Vinje 2004, [14] Girish 2002, [6] and Rachakonda 2008 [7] - based on the name of the first author and year of publication of the corresponding manuscript. Primers from Green 1995 amplified a 113 bp region of the RdRp region, while Kageyama 2003 amplified a 468 bp region of the ORF 1-2 junction. The Vinje 2004 primers targeted two regions of the NoV genome-ORF 1-2 junction region (213 bp) and part of the norovirus capsid region (253 bp). Two primer sets used in previous studies from India (Girish 2002 and Rachakonda 2008) amplified a part of the RdRp region by nested RT-PCR. Both primer sets were modified from previously published primers. [15] The oligonucleotide sequences and the target regions for each of the primers are given in [Table - 1]. The relative locations of the primers on the genome of GII.4 reference strain Lordsdale are shown in [Figure - 1]. Study samples A total of 100 stool samples, including 49 samples identified as positive for norovirus and 51 negative samples from previous hospital- and community-based studies on norovirus diarrhoea in children < 5 years of age at a tertiary care hospital in Vellore, India, were tested in this study. All the hospital and community samples were screened by the Vinje 2004 and Kageyama 2003 primer sets. The settings in which the samples were collected have been previously described. [8],[16] Written informed consent was obtained from parents of all children prior to the use of the samples, and the study was approved by the Institutional Review Board. Ribonucleic acid extraction and complementary deoxyribonucleic acid synthesis Viral RNA was extracted from 200 μl of 20% (w / v) stool suspension in Minimal Essential Medium using guanidium isothiocyanate and silica, as described by Boom et al.[17] A known positive control was included in all extractions, to detect PCR inhibition. Complementary deoxyribonucleic acid (cDNA) synthesis was carried out by reverse transcription at 37°C, for one hour, with random hexamers (hexamers; Pd(N)6, Pharmacia Biotech, Little Chalfont, Buckinghamshire, UK), and 400 U of Moloney murine leukemia virus reverse transcriptase (Invitrogen, Life Technologies, Paisley, UK). The cDNA were stored at -20°C until further use. Reverse transcription polymerase chain reaction for detection of Noroviruses Complementary deoxyribonucleic acid from all samples was tested for NoV, by RT-PCR, using all primer sets. Single round PCR using 5 ul of cDNA was carried out for the detection of the NoV using the Green 1995, Kageyama 2003, and Vinje 2004 primers. As the Vinje 2004 primer targeted two regions of the norovirus genome, the sample was called positive if amplification was seen in either region targeted by the primer set. Nested RT-PCR was set up with primer sets from Girish 2002 and Rachakonda 2008, wherein 5 μl of cDNA was used to set up the first round PCR with external primer pairs followed by nested PCR with 5 μl of the first round product and internal primers. A sample was positive if amplification was seen in the second round PCR. Positive, negative, and no template controls were included in every PCR run, to ascertain any carryover contamination. The PCR cycling conditions used for each of the primer sets were as described in the respective publications. [6],[7],[12],[13],[14] Sequence analysis Sequencing of a subset of positive amplicons was carried out by using the ABI PRISM Big Dye Terminator cycle sequencing ready reaction kit (Applied Biosystems, CA). The sequences were resolved in an automated DNA sequencer ABI PRISM 310 Genetic Analyzer. The sequences were imported into the BioEdit software (version 7) and compared with the published sequences available from GenBank. Results A total of 74 samples were identified as positive for NoV by at least one primer set, for one of the regions being amplified. All calculations for sensitivity were performed by using the 74 positive samples as a 100% score. The most sensitive primer set was Girish 2002, which could detect 60 / 74 (81%) positives. Forty samples (40 / 74, 54%) were identified as positive by the Green 1995 primers, while the remaining three primer sets picked 33 / 74 (45%) positives each. Interestingly, agreement between all the assays was found in only 12 (16%) samples, positive by all primer sets, and 26 negative samples. Of the 74 samples positive for NoV, 25 (33%) samples were identified as positive by only one primer set. These included 18 samples detected by Girish 2002 primers, three samples by Green 1995 primers, two samples by Kageyama 2003 primers, and one sample each by the Vinje 2004 and Rachakonda 2008 primers. To confirm the specificity of detection, subsets of these samples were chosen at random for sequencing, to confirm the specificity of the amplicons detected. Of the 25 samples identified as positive by a single PCR, 11 amplicons (Girish 2002 - 7, Kageyama 2003 - 2, Green 1995 - 1, and Rachakonda 2008 - 1) were sequenced and confirmed as genogroup II NoV [Table - 2]. Thirty-five samples (35 / 74, 47%) were identified as positive by at least three primer sets, and 49 / 74 (66%) samples were identified as positive by at least two primer sets. The subsets of these were also sequenced and none of the selected samples failed sequencing. The 25 samples identified by the new primer sets alone had been previously identified as being negative by both Kageyama 2003 and Vinje 2004 primers. The results were analysed based on the region of amplification. Of the 68 positives identified in the RdRp region, 60 samples (88.2%) were detected by Girish, 2002 and 40 samples (58.8%) were detected by Green, 1995. Forty-two samples were identified as positive in the ORF1-2 region including 33 (78.5%) samples by the Kageyama 2003 primers and 29 (69%) by the Vinje 2004 primers. Discussion Since molecular diagnostic techniques became widely available, RT-PCR has become the method of choice for the detection of NoVs in faecal, environmental, and food samples. [18] However, the choice of primers used in RT-PCR assays varies from laboratory to laboratory. The differences in sensitivity and specificity of various primers often lead to difficulties in comparing results from various studies. Indeed, in an international collaborative study to compare RT-PCR assays for the detection and genotyping of NoVs from several countries, no single assay stood out, as the method of choice and a range of sensitivities in results were seen. [19] In this study, five sets of published oligonucleotide primers were evaluated for the detection of NoVs in samples from a clinical and community setting. The choice of primer sets was based on their use in previous studies published from India. The study focused on GII NoVs because of previous reports demonstrating the predominance of GII strains and the lack of circulation of GI viruses in this region. [16] Higher detection rates were achieved either by using multiple primers or by using a sensitive nested RT-PCR assay in the current sample set. The findings of this study were similar to a study evaluating nine sets of PCR primers and seven internal oligonucleotide primers in the RdRp region for the detection of noroviruses in Japan, where it was found that there was no single primer pair that could detect all NoVs, and at least three primer pairs were required to detect the virus. [5] This suggested that the use of combinations of primer sets could increase the sensitivity of detecting NoVs, as compared to the use of a single set of primers, in any geographic region. The most sensitive primer set was Girish 2002, which used previously designed primers, [15] with some modifications in a nested RT-PCR format, for the detection of NoVs. The increased sensitivity of these primers over other primers may be due to the use of a nested RT-PCR. Although these primers appear to be the best among those tested for the detection of GII NoVs in India, it must be noted that the nested PCR assays have sometimes been considered less favourable, due to the increased risk of a carryover. [19] In this study, water blanks and negative controls were included in every experiment, to rule out the possibility of carry-over contamination. However, the use of a highly sensitive technique, such as the nested RT-PCR, could result in an overestimate of the actual number of cases of diarrhoea attributed to NoV. [20] An estimation of the viral load by real time RT-PCR might be useful to distinguish between cases of diarrhoeal disease caused due to NoV and those where the presence of low levels of NoV may not actually be the cause of illness. One of the limitations of this study is that although all the primers were evaluated for detection of noroviruses, the primer sets were originally designed for different purposes. The Green 1995 [12] and Kageyama 2003 [13] primers were designed for detection, while the remaining primers sets were designed for genotyping (Vinje, 2004, [14] Girish, 2002, [6] Rachakonda, 2008 [7] ). It was therefore important to note the specificity of all primers evaluated for the detection of NoVs. Subsets of positive amplicons were sequenced and no non-specific PCR products were identified, indicating that all primer sets were specific for the detection of NoVs. Refinement and evaluation of diagnostic techniques is needed to assess the true burden and aetiology of diarrhoeal disease. This is particularly true for NoVs where virus evolution and introduction of new strains require frequent updating of methods, and where one method cannot be uniformly applied in all parts of the world. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12005t1.jpg] [mb12005f1.jpg] [mb12005t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}