 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
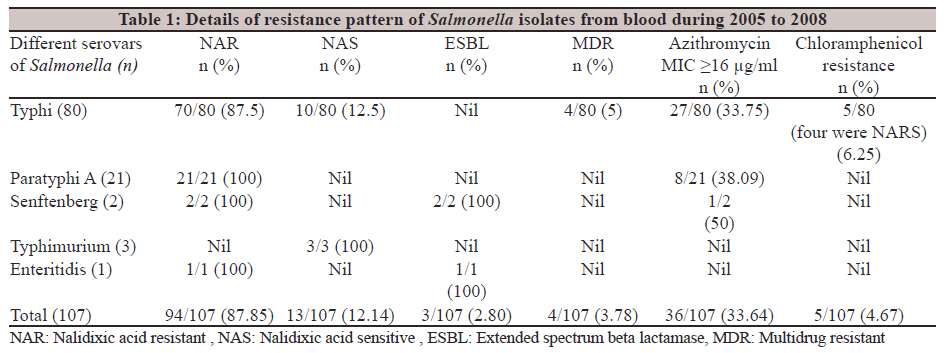
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 30-33 Original Article Rationale of azithromycin prescribing practices for enteric fever in India S Rai1, S Jain2, KN Prasad2, U Ghoshal2, TN Dhole2 1 Department of Microbiology, UCMS and GTB Hospital, Dilshad Garden, Delhi - 110 095, India Correspondence Address: Date of Acceptance: 27-Sep-2011 Code Number: mb12006 PMID: 22361757 DOI: 10.4103/0255-0857.93017 Abstract Purpose: The present study was performed to assess the current susceptibility pattern of blood isolates of Salmonella spp from a super specialty hospital in North India against nalidixic acid, ciprofloxacin and azithromycin and compare the in vitro and in vivo response against azithromycin. Keywords: Azithromycin, multidrug resistant Salmonella Typhi, nalidixic acid, Salmonella Introduction Enteric fever caused by Salmonella spp is one of the most common causes of systemic infections in India and is one of the common causes of travel associated illnesses. [1] Drug resistance in Salmonella has been on the rise in India with emergence of nalidixic acid-resistant (NAR) Salmonella and an increasing clinical non-response to fluoroquinolones. [2],[3],[4],[5],[6] Treatment options are getting limited with emergence of resistance to third- and fourth-generation cephalosporins. [7],[8],[9] A reversal of resistance pattern in favour of chloramphenicol has been observed and with the rising resistance to third-generation cephalosporins, continuous dynamism has been observed in antibiogram patterns worldwide. The Western studies have favoured azithromycin as the potential drug that produces good clinical response. [10] However, due to the lack of breakpoint concentrations in various international guidelines, its in vitro interpretation has often been difficult for Salmonella. In the Western literature, treatment has heavily banked upon the use of azithromycin due to its high intracellular concentration and good clinical response. Clinical trials advent the use of 20 mg/kg per day with a maximum dose of 1000 mg/day for five to seven days for complete cure. [10],[11] Limited role of azithromycin has been suggested by a study where the in vitro0 MIC range was between 4 and 16 μg/mL.[12] . Randomized trials have suggested similar efficacy of azithromycin and ciprofloxacin, both clinically and in vitro studies, against enteric fever caused by sensitive as well as MDR Salmonella Typhi isolates. [13] Non-availability of breakpoint concentrations of azithromycin for Salmonella in most standard antibiotic guidelines makes the laboratory interpretation difficult. The purpose of the present study was to assess the current susceptibility pattern of blood isolates of Salmonella, correlate with other Indian studies and to evaluate and compare the pivotal role of azithromycin prescribing practices for enteric fever in India and Western countries. Materials and Methods The present study was performed on 107 non-repeat isolates of Salmonella spp. isolated from blood samples from 2005 to 2008 in a tertiary care Super Specialty hospital of North India. Identification of fresh growth of the isolates was done by routine biochemical tests followed by serotyping with standard specific antisera (Denka Seiken Co Ltd, Japan). All isolates were subjected to susceptibility against chloramphenicol (30 μg), nalidixic acid (30 μg), ampicillin (10 μg), trimethoprim-sulphamethoxazole (1.25/23.75 μg), ceftriaxone (30 μg), cefepime (30 μg), ciprofloxacin (5 μg), gatifloxacin (5 μg), tetracycline (30 μg), amoxicillin-clavulanic acid (20/10 μg) and ofloxacin (5 μg) (Oxoid, Basingstoke, UK) by disc diffusion as per Clinical and Laboratory Standards Institute (CLSI) guidelines.[14] Escherichia coli ATCC 25922 was used as a quality control strain. The minimum inhibitory concentration (MIC) was determined against nalidixic acid, azithromycin and ciprofloxacin by E - Test; (AB Biomerieux, Solna, Sweden). The MIC breakpoints were interpreted according to CLSI guidelines. International guidelines on antimicrobial susceptibility testing do not mention a value for MIC breakpoint for azithromycin against Salmonella. The British Society of Antimicrobial Chemotherapy (BSAC) guidelines however suggest clinical susceptibility to azithromycin in isolates with MIC values of ≤ 16 μg/mL.[15] Therefore, an MIC breakpoint of ≤ 16 μg/mL was considered as sensitive and > 16 μg/mL as resistant. The MIC90 and MIC 50 values were calculated for nalidixic acid, azithromycin and ciprofloxacin. MIC 90 values of ciprofloxacin were assessed for NAR Salmonella isolates. MIC 90 values were also assessed for patients who did not respond to azithromycin therapy. Available treatment history and hospital discharge summary of patients from whom these isolates were recovered was retrospectively analysed using their central registration numbers on the Hospital Information System (HIS) software and correlated with the susceptibility findings. Strains resistant to third-generation cephalosporins were investigated for production of extended spectrum beta-lactamase (ESBL) using cefotaxime, cefotaxime/clavulanate and ceftazdime, ceftazidime clavulanate discs as per CLSI guidelines. [14] Results Of the 107 blood isolates of Salmonella [Table - 1], 80 were serotype Typhi, 21 Paratyphi A and 6 belonged to other serotypes (3 Typhimurium, 2 Senftenberg and 1 Enteritidis). Among these, 94 (87.8%) were nalidixic acid-resistant (NAR) Salmonella and remaining 13 were nalidixic acid-sensitive (NAS) Salmonella. Among the 80 strains of serotype Typhi, 70 (87.5%) were NAR Salmonella and remaining 10 (12.5%) were NAS Salmonella. As per definition, only four (3.7%) of the Salmonella isolates were multi drug resistant (MDR) i.e., resistant to ampicillin, chloramphenicol and cotrimoxazole. [7] All of the MDR isolates were serotype Typhi and were NAR Salmonella. All of the 21 strains of serotype Paratyphi A were also NAR Salmonella. Isolation of non-typhoidal salmonellae from blood though common in Sub-Saharan Africa is a rare finding in India. [16] Such strains are usually isolated from wound and blood samples of hospitalized patients and are likely to be potential sources of hospital outbreaks. [17] All Senftenberg and Enteritidis isolates were NAR and ESBL producers while all three Typhimurium strains were NAS and sensitive to third-generation cephalosporins. As previously mentioned, the MIC interpretative breakpoint of >16 μg/mL was considered resistant for azithromycin.[15] Taking this into consideration, 36 (33.64%) of all Salmonella isolates were resistant to azithromycin. Even among the 13 NAS Salmonella (10 Typhi and three Typhimurium), 5 had azithromycin MIC′s ≥ 24 μg/mL. Sensitivity to chloramphenicol was observed in 102 (95.32%) of all the isolates thereby showing a reversal of the susceptibility pattern. This was in correlation with another Indian study favouring reuse of chloramphenicol. [18] Among remaining five isolates which were resistant to chloramphenicol, four were MDR. There was also an increase in the prevalence of Paratyphi A isolates from a single isolate in the year 2005 to 4 in 2006, 5 in 2007 and 11 isolates in 2008. The MIC 90 values for nalidixic acid, azithromycin and ciprofloxacin were >256, 24 and 0.75 μg/mL while MIC50 values were >256, 12 and 0.38 μg/mL, respectively. Of the total NAR isolates, the MIC 90 value for ciprofloxacin was 0.75 μg/mL which falls in the decreased susceptibility range (0.125-1 μg/mL) for ciprofloxacin.[19] Of the 107 isolates evaluated, treatment history was retrieved from discharge summaries and clinical notes for 57 patients from the Hospital Information System database. The signatory clinicians of the discharge and treatment summaries were contacted where changes in therapy was made from azithromycin to other drugs. The description of clinical non-response was not uniform and varied from 2 to 5 days after intake of first dose of azithromycin with no significant improvement in patient′s symptoms. Among these, 36 patients were given azithromycin therapy varying from 0.5 to 1 g PO per day for 3 to 5 days. There was a change made in the therapy of 28 patients from azithromycin to oral third-generation cephalosporins or amoxicillin as per standard recommendations. This was done on the basis of non responsiveness to azithromycin therapy as mentioned in 19 of the 28 patients. Reason for changes made in the remaining nine patients was not mentioned, but another probability could have been the non-availability of azithromycin sensitivity from the bacteriology laboratory. Among these 19 isolates, all were NAR Salmonella Typhi (NARST). MIC range for azithromycin in these isolates ranged from 6 to 64 μg/mL with a MIC90 value of 24 μg/mL. Discussion The prevalence of NAR Salmonella (NARS) has been increasing in India with reports rising from 51% in 2006 [8] to as high as 87.8% in the present study and even higher in other recent Indian studies. [20],[21],[22] In contrast, the literature has cited a fall in the prevalence of MDR isolates of Salmonella, being as high as 94% in 1989-91, [23] to 92.3% in 1994, [24] 61.4% in 1996, [25] 39% in 2006 [26] to as low as 3.7 % in the present study. In another Indian study done on 305 Salmonella isolates, only one was MDR [20] while a study from South India reported the MDR prevalence to be 12%. [21] While studies in India have correlated susceptibility of fluoroquinolones in NARS isolates [27] and their molecular epidemiology, [28] the role of azithromycin and its clinical response has not been correlated. Another prospective study from Pondicherry, from 2005 to 2009 demonstrated high sensitivity to ampicillin, chloramphenicol and cotrimoxazole of 66% and just 22% multidrug resistant salmonella typhi (MDRST) indicating a steady fall and rise of MDRST and NARS isolates. [6] With respect to prescribing azithromycin, most of the antimicrobial susceptibility standards do not mention the MIC breakpoints of azithromycin for Salmonella. However, it is still being prescribed worldwide with many clinical trials suggesting its superior clinical efficacy. [29] From a microbiological point of view, this is a questionable practice. Secondly, the MIC 90 values for azithromycin against Salmonella isolates from India do not coincide with the strains isolated from the Western countries. In the present study, MIC 90 for azithromycin was 24 μg/mL, which was the same as mentioned in another study from India.[30] MIC 90 of Salmonella isolates studied in the Western countries have values as low as 4 or 8 μg/mL.[31],[12] A review done on the role of azithromycin in enteric fever indicated that fever clearance time with the use of azithromycin was not different from any other drug and that it was only marginally better than fluoroquinolones in terms of reducing clinical failure. [32] The present study augments this finding as 19 patients had documented clinical non-response to azithromycin. This information may become important especially for patients who acquire enteric fever in India and get azithromycin therapy when they reach back to their native Western countries. In developing countries like India, ciprofloxacin continues to be the mainstay for the treatment of enteric fever as it is orally effective and economical [33] and also probably the clinicians are not aware of the clinical implications of a NARS isolate. With the rise of NARS and fall in MDR isolates, [34] one may look at recycling of chloramphenicol, cotrimoxazole and ampicillin instead of azithromycin. Large-scale randomized control trials with follow up and laboratory correlation need to be done for azithromycin usage in the Indian subcontinent before incorporating its Western prescribing practices. Acknowledgment The Authors would like to thank Mr Malay Ghar, Mr Dinesh Gangwar and Mr Rajesh Sharma for laboratory and logistical support. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12006t1.jpg] |
| |||||||||

{kind=link}