 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
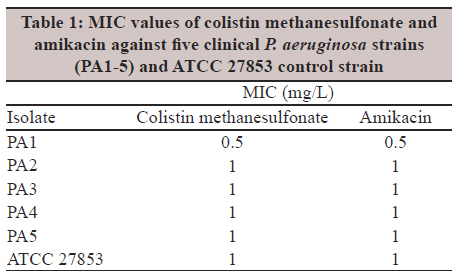
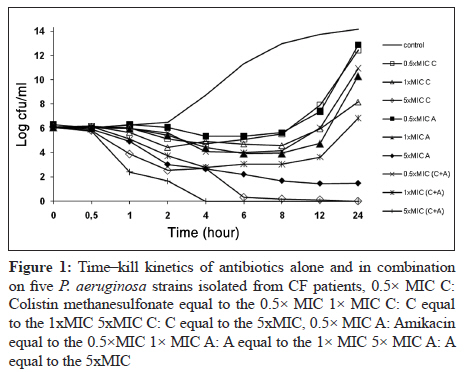
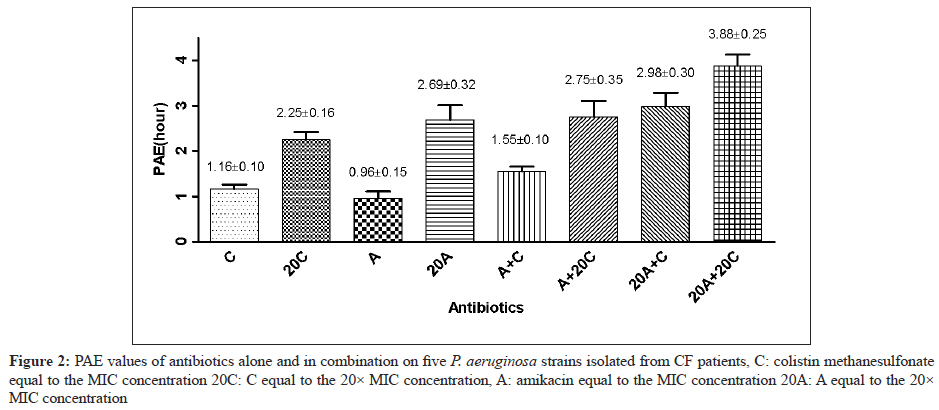
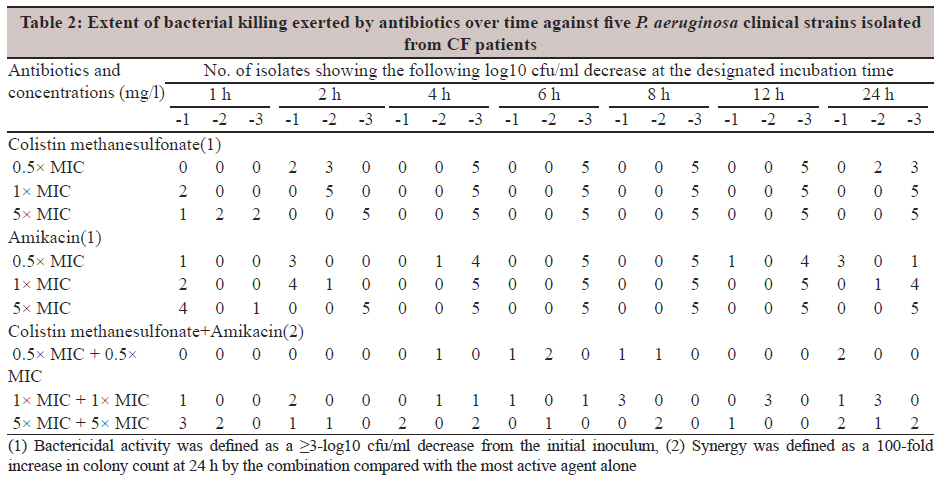
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 34-38 Original Article In vitro pharmacodynamic properties of colistin methanesulfonate and amikacin against Pseudomonas aeruginosa C Bozkurt-Guzel, AA Gerceker Department of Pharmaceutical Microbiology, Faculty of Pharmacy, Istanbul University, 34116 Beyazit, Istanbul, Turkey Correspondence Address: Date of Submission: 15-Jun-2011 Code Number: mb12007 PMID: 22361758 Abstract Purpose: In vitro pharmacodynamic properties of colistin methanesulfonate and amikacin were investigated by studying time-kill kinetics and post-antibiotic effect (PAE) against strains of Pseudomonas aeruginosa isolated from patients with cystic fibrosis. Keywords: Antibiotic combinations, colistin methanesulfonate, cystic fibrosis, Pseudomonas aeruginosa, postantibiotic effect Introduction Pseudomonas aeruginosa is a gram-negative bacterium considered as one of the major human opportunistic microorganisms and the main cause of a wide range of nosocomial infections in immunocompromised and cystic fibrosis (CF) patients. [1] CF is the most common life-limiting genetic disease in the Caucasian population. Over time, people with CF become chronically infected with P. aeruginosa with associated declining pulmonary function and increasing symptoms. [2] Although antimicrobial therapy has undoubtedly prolonged the lives of patients with CF, [3] treatment and prevention of P. aeruginosa infections in CF patients is a major problem. As no novel agents have been introduced to combat these microorganisms, and as it seems unlikely that any new agents will be introduced soon, researchers may become forced to rediscover older agents such as colistin, a polypeptide antibiotic. It was first isolated in Japan from Bacillus polymyxa var colistinus in 1947 and became available for clinical use in 1959. However, it was replaced in the 1970s by antibiotics considered less toxic. [4] Notably, the recent reuse of polymyxins has not been associated with such high rates of toxicity as reported when these agents were first introduced into clinical practice. It should be highlighted that the dosages of polymyxins used in most of the studies published in the old literature were considerably higher compared to the current recommended dosages. In fact, several reported cases of polymyxin-induced toxicity were associated with overdose. Thus, this may account for the observed difference in the incidence of polymyxin-induced toxicity noted between the old and recently published studies. [5] It is also used therapeutically as colistin methanesulfonate, which has sulfomethylated amino groups, in order to minimise pain at injection sites and toxicity. [6] Recent investigations have revealed colistin methanesulfonate to be less nephrotoxic than amikacin or tobramycin. [7] Just as, there is a rise in the number of in vitro studies using this novel agent. [8],[9] Additionally, colistin has been successfully administered alone and in combination for the treatment of P. aeruginosa infections in CF patients. [10] The most appropriate dosing schedule of an antibiotic depends on its pharmacodynamic parameters such as the MICs for the target bacteria, time-kill kinetics and post-antibiotic effect (PAE). As a pharmacodynamic parameter the importance of PAE is that antibiotics or antibiotic combinations, those inducing a long PAE, may be administered with longer dosing intervals without loss of efficacy, thus letting the patients suffer less possible side effects. We also employed time-kill kinetic studies which provided a dynamic picture of antimicrobial action and interaction over time. [11] For these reasons, the aim of the present study was to investigate the pharmacodynamic properties of colistin methanesulfonate alone and in combination with amikacin against five P. aeruginosa strains isolated from CF patients for evaluating the preclinical information. Materials and Methods Bacterial isolates Five strains of P. aeruginosa isolated from CF patients (PA1-PA5) were obtained from sputum and throat secretion specimens submitted to the Clinical Microbiology Laboratories of Istanbul University, Istanbul Faculty of Medicine. All strains were identified by the API 20 NE System (bioMerieux Vitek, Marcy l′Etoile, France). P. aeruginosa ATCC 27853 was used as a quality control strain. Antibiotics Colistin methanesulfonate was obtained from Sigma Aldrich and amikacin was kindly provided from Eczacibasi Pharmaceuticals. Stock solutions from dry powders were prepared at a concentration of 5120 mg/l and stored frozen at -80 o C. Frozen solutions of antibiotics were used within 6 months. Media Mueller-Hinton broth (MHB, Difco Laboratories, Detroit, MI) was used for MIC determinations, time-kill kinetic studies and for PAE experiments. Pour plates of Tryptic Soy agar (TSA, Difco Laboratories, Detroit, MI) were used for colony counts. MIC determination Amikacin MICs were determined by the microbroth dilution technique as described by CLSI. [12] Serial twofold dilutions ranging from 256 to 0.25 mg/l were prepared in MHB. The MICs of colistin methanesulfonate were determined by using a microbroth dilution assay modified from the method of CLSI. [13] This method was proposed by Steinberg since cationic peptides bind polystyrene causing an increase in MIC values up to twofolds. Briefly, serial twofold dilutions ranging from 640 to 0.3 mg/l were prepared in 0.2% BSA and 0.01% acetic acid buffer in Eppendorf tubes (polypropylene). 0.01 ml of each concentration was added to each corresponding well in 96-well polypropylene (Greiner 650261) microtitre plate. Each well was inoculated with 0.1 ml of a 4-6 h broth culture which gives a final concentration of 5 × 10 5 cfu/ml in the test tray. The trays were covered and placed in plastic bags to prevent evaporation and incubated at 37oC 18-20 h. The MIC was defined as the lowest concentration of antibiotic giving complete inhibition of visible growth. Experiments were performed in triplicate. Determination of time-kill curves The time-kill curve method was used to evaluate concentration-dependent bactericidal activity and synergy testing and was performed using the broth macrodilution technique described by the NCCLS. [14] For each strain, antibiotics were studied alone and in combination at the 0.5×, 1× and 5× MIC concentrations. Antibiotic-free control was included for each strain. Inoculum was prepared spectrophometrically and added to the flasks to yield a final concentration of 1×10 6 cfu/mL. The final inoculum was determined at time zero; viable counts were performed after 0, 0.5, 1, 2, 4, 6, 8, 12 and 24 h in a 37oC calibrated shaking water bath. All tests were performed in duplicate. The rate and extent of killing were determined by plotting viable colony counts (log 10 cfu/mL) against time. The lower limit of detection for time-kill assays was 1 log 10 cfu/mL. The results were interpreted by the effect of the combination in comparison with the effect of the most active agent alone. Synergism and antagonism were defined as a 100-fold increase or decrease, respectively, in colony count at 24 h by the combination compared with the most active agent alone. Additivity (or indifference) was defined as a <10-fold change increase (or decrease) in killing at 8, 12 and 24 h with the combination in comparison with the most active single antimicrobial alone. Bactericidal activity was defined as a ≥3-log 10 cfu/ml decrease from the initial inoculum. Determination of the post-antibiotic effect PAEs were determined by a standard viable counting method. [15] Organisms in the logarithmic phase of growth, producing a final concentration of inoculum in the test tubes of approximately 1×10 6 cfu/ml, were exposed to concentrations of colistin methanesulfonate and amikacin equal to 1× or 20× MIC, alone and in combinations. After incubation for 1 h in a 37oC calibrated shaking water bath, antibiotics were removed by washing the contents of the tubes twice with MHB. After centrifugation for 10 min at 5000 rpm, pellets were resuspended in prewarmed broth; controls were handled similarly. Bacterial counts of the tube contents were determined at time zero, immediately before and after centrifugation and each hour after centrifugation for 8 h by a pour plate technique. Bacterial growth was assessed after counting colonies and multiplying with the appropriate dilution factor. The PAE was defined as PAE = T - C, where T is the time (in hours) required for the count in the test culture to increase 1 log 10 above the count observed immediately after centrifugation and C is the corresponding time for the controls. Experiments were performed in triplicate. Statistical analysis Statistical analysis for the comparison of PAEs were performed using the non-parametric ANOVA and Bonferroni correction for post-hoc comparisons. A correction according to Bonferroni was applied to avoid random correlations. All data were reported as mean ± standard error (mean±SE). Any value of P below 0.05 was considered as statistically significant. Results The MICs of colistin methanesulfonate and amikacin ranged from 0.5 to 1 mg/l are shown in [Table - 1]. In time-kill kinetic studies, colistin methanesulfonate and amikacin were bactericidal in a concentration-dependent manner [Figure - 1]. PAEs for clinical strains of P. aeruginosa for antibiotics, alone and in combination, are displayed in [Figure - 2]. According to the results, the mean values of PAEs for the five clinical strains, colistin methanesulfonate at a concentration equal to and 20 times of MIC values were found to be 1.16±0.10 h and 2.25± 0.16 h, respectively and for amikacin 0.96±0.15 h and 2.69±0.32 h, respectively. Both of the antibiotics showed increased PAE values in a concentration-dependent manner. When the antibiotics were used in combination at a concentration of 20 times of the MIC values, the PAEs were prolonged to 3.88±0.25 h [Figure - 2]. The extent of bacterial killing exerted by antibiotics over time against five P. aeruginosa strains are displayed in the [Table - 2]. For the control strain P. aeruginosa ATCC 27853, colistin methanesulfonate at a concentration equal to and 20 times of MIC values, exhibited 1.5 h and 2.2 h, and amikacin 1.5 h and 2.5 h of PAEs, respectively; and when antibiotics were used in combination at 20× MIC, the PAE was prolonged to 3.9 h. Discussion Apart from the considerable data on the MICs of colistin methanesulfonate, very little study has been conducted on the pharmacodynamics of colistin methanesulfonate, particularly against P. aeruginosa.[8] The most appropriate dosing schedule of an antibiotic depends on its pharmacodynamic parameters such as the MICs for the target bacteria, time-kill kinetics and PAE. Because there are limited pharmacodynamic studies of colistin methanesulfonate, in the current study the time-kill kinetics and PAE of colistin methanesulfonate were examined against strains of P. aeruginosa isolated from patients with CF. As seen from both [Table - 2] and [Figure - 1], both colistin methanesulfonate and amikacin antibiotics showed their bactericidal activities in a concentration-dependent manner where at 5× MIC the bactericidal activities were seen in 2 h. And when the concentrations were decreased, it was seen in 4 h and 6 h. One of the most important finding in this study was that colistin methanesulfonate at 1× and 5× MIC and amikacin at 5× MIC concentrations, alone, displayed bactericidal activity at 24 h against all of the strains. Other researchers have examined the bactericidal activities of colistin methanesulfonate at two concentrations (0.5 and 5 mg/l) and have demonstrated more rapid killing with the higher concentration. [16] According to another study, colistin methanesulfonate was rapidly bactericidal at the highest concentrations, with counts falling to undetectable numbers in 1 to 4 h at 16 to 64 times the MIC. [8] However, additional studies are needed to establish which is clinically required. Combination therapy plays an important role in the management of P. aeruginosa infections in CF patients. [17] When the antibiotics were used in combinations at a concentration of 1× MIC or 5× MIC in the killing-curve technique, synergistic effects have been seen against three P. aeruginosa strains. Some of the strains produced earlier synergistic effects at 1, 2, 4, 6, 8 and 12 h [Table - 2]. In contrast to the checkerboard technique, which typically provides only inhibitory data, the killing-curve technique measures the microbicidal activity of the combination being tested. For this reason, it is often more relevant for clinical situations in which bactericidal therapy is desirable. The other major advantage of killing curves is that they provide a dynamic picture of antimicrobial action and interaction over time based on serial colony counts. [11] It has been shown by our group with this current study and others [18],[19] that time-kill synergy testing is a discriminatory method, but more time consuming. Our results confirm and extend the use of time-kill kinetics to detect synergy between colistin methanesulfonate and amikacin. The results of this research also indicate that colistin methanesulfonate and amikacin, both alone, showed significant PAEs on P. aeruginosa strains in a concentration-dependent manner [2]. According to our results, colistin methanesulfonate produced a significant PAE of 1.16±0.10 h against the strains at 1× MIC which is in agreement with results obtained by other investigators. [8] We have seen almost the same pattern as we did with amikacin. When the concentration of antibiotics was increased, the duration of PAE was prolonged to almost two times (P<0.001). The benefit of this prolonged PAE value of antibiotics may allow for prolonged dose interval without reduced efficacy, and possibly a lower frequency of adverse effects. The interaction of two antimicrobials produced a prolonged PAE compared with that of single agents. [15],[20],[21] At 20× MIC, antibiotics exhibited longer PAE values than when they were used in combination at a concentration equal to MIC. When antibiotics were used in combination at 20× MIC, the duration of PAE was increased significantly when compared with other parameters (P<0.001). According to these results, PAE values of colistin methanesulfonate or amikacin alone or in combination might have a clinically significant effect on designing optimal dosage regimens in CF patients. Studies have demonstrated positive outcomes utilizing once daily (or an extended-interval) administration of aminoglycosides in infections with gram-negative organisms. [22],[23] According to our results, when amikacin is used in combination with colistin methanesulfonate, that shows the same pharmacodynamic properties, once daily administration of amikacin might be prolonged in accordance with the clinical studies. Knowledge of the PAE permits optimal use of antibiotics and such data could have important implications for timing of the doses during therapy with antimicrobial combinations, which could also decrease the expected toxicity of each single agent by permitting the administration of wider dosing intervals. If the pharmacodynamics of these agents are throughly understood, dosing regimens may be designed rationally to optimise patient outcomes and to minimise the emergence of resistance to these agents. However, more data are needed to answer important clinical questions, including the appropriate dosage and comparison of monotherapy with combination therapy. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12007t2.jpg] [mb12007f1.jpg] [mb12007f2.jpg] [mb12007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}