 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
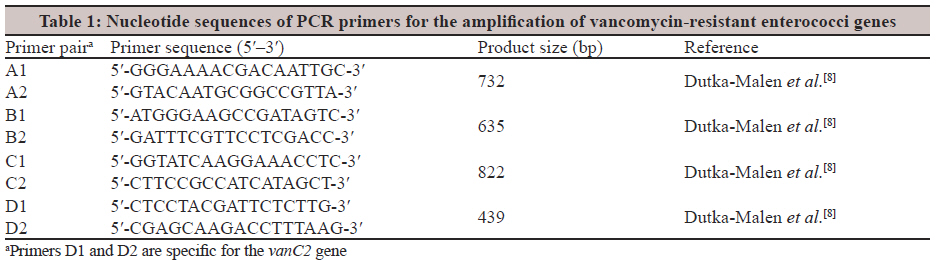
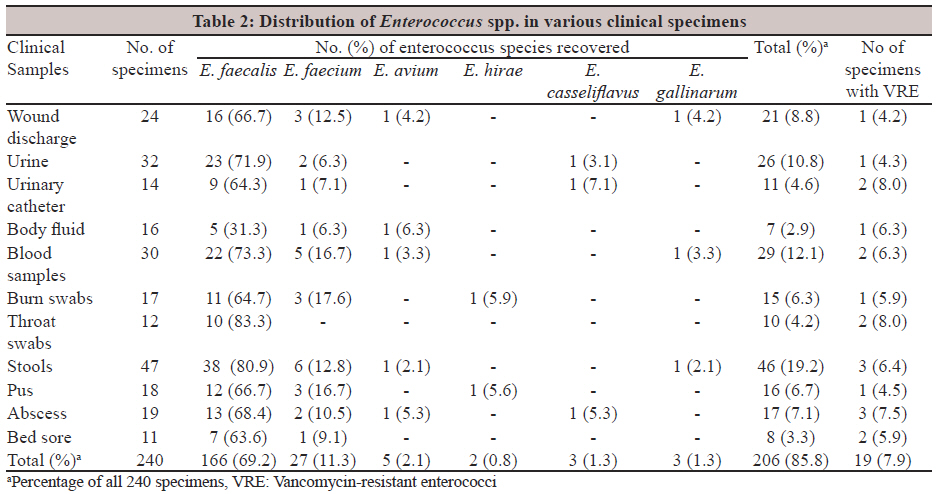
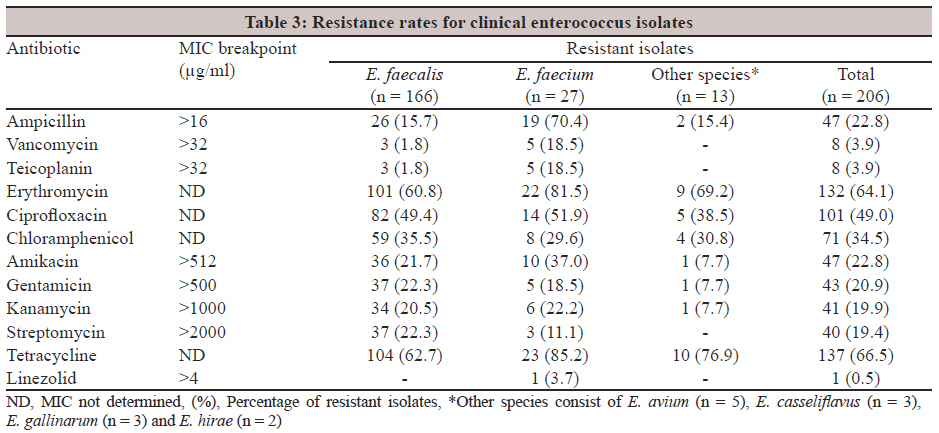
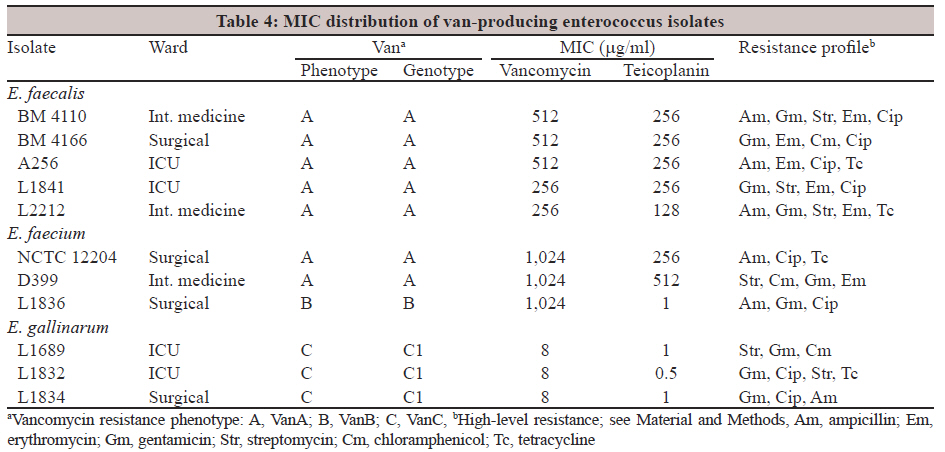
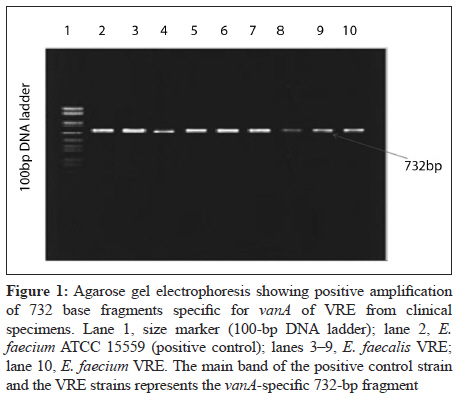
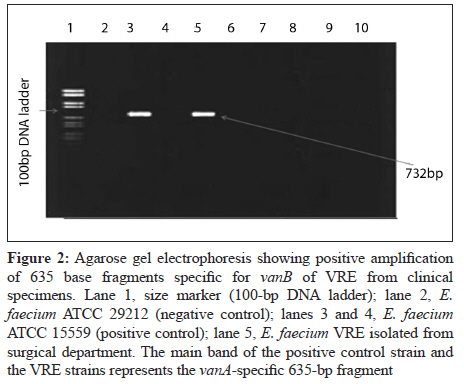
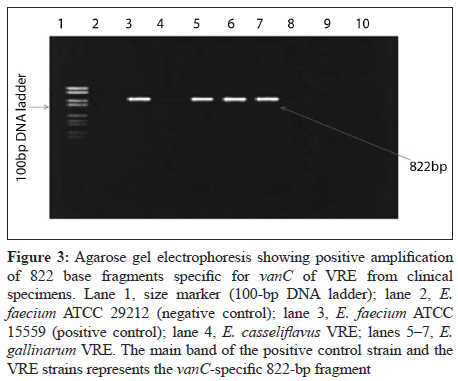
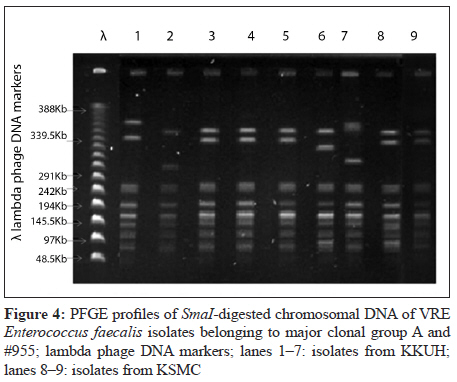
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 44-51 Original Article Prevalence and antimicrobial resistance pattern of multidrug-resistant enterococci isolated from clinical specimens MM Salem-Bekhit1, IMI Moussa2, MM Muharram3, FK Alanazy4, HM Hefni5 1 Department of Pharmaceutics, Kayyali Chair for Pharmaceutical Industries, College of Pharmacy, King Saud University, P. O. Box 2457, Saudi Arabia Correspondence Address: Date of Acceptance: 27-Dec-2011 Code Number: mb12009 PMID: 22361760 DOI: 10.4103/0255-0857.93032 Abstract Purpose: Vancomycin-resistant enterococci (VRE) pose an emerging problem in hospitals worldwide. The present study was undertaken to determine the occurrence, species prevalence, antibacterial resistance, and phenotypic and genetic characteristics of VRE isolated in Riyadh hospitals, KSA. Keywords: Antibiotic resistance, Enterococci, hospitalised patients, VRE, vanA Introduction Enterococci have evolved over the past century from being an intestinal commensal organism of little clinical significance to becoming the second most common nosocomial pathogen associated with significant morbidity and mortality. [1],[2] In recent years, there has been a rapid increase in the incidence of infection and colonisation of patients with vancomycin-resistant enterococci (VRE). The resistance may be intrinsic or acquired via gene transfer. [1] Widespread use of vancomycin and extended-spectrum cephalosporins in hospitals likely contributed to the emergence and dramatic increase of VRE over the past 20 years. [3] The prevalence of VRE has dramatically increased worldwide. [2] The National Nosocomial Infection Surveillance (NNIS) system in the USA has revealed a significant increase in the percentage of invasive nosocomial Enterococcus strains displaying high-level vancomycin resistance. [4] Although more than one dozen species of enterococci have been identified, Enterococcus faecalis was the most common species associated with nosocomial infections, followed by Enterococcus faecium, and both species are responsible for about 95% of infections caused by enterococci. [4] VRE, especially E. faecalis and E. faecium, are prevalent in the hospitalised patients. Other Enterococcus species, E. gallinarum, E. casseliflavus, E durans, E. avium, and E. hirae, are isolated much less frequently and account for less than 5% of clinical isolates. [1] Infections caused by VRE were found to be associated with adverse outcome such as extended length of hospital stay, increased cost and increased mortality. [2],[4] The glycopeptide vancomycin is the first choice alternative to penicillin-aminoglycoside combination for treatment of systemic enterococcal infections. Different types of vancomycin resistance genes have been reported in enterococci. Glycopeptide-resistant genotypes in enterococci include VanA (high-level resistance), which is detected in a wide variety of enterococcal species, VanB, VanB2 and VanD with moderate to high-level resistance and VanC (C1, C2, C3) causing intrinsic low-level resistance. [5] Vancomycin resistance is most commonly found in E. faecium and is encoded by the vanA gene cluster carried on the mobile genetic element Tn1546. [6] Transfer of resistance can occur via conjugative plasmids. Enterococci, as reservoirs of antibiotic resistance genes, tend to transfer their resistance genes to the other bacteria, including methicillin-resistant Staphylococcus aureus.[7] Monitoring the antibiotic resistance of enterococci isolated from clinical specimens is a useful tool to get information about the prevalence of VRE and will be essential for controlling the spread of bacterial resistance. Despite the increasing reports of VRE in different countries, there is a distinct lack of data regarding the molecular characterisation of VRE isolates, originating from the Middle East, including Saudi Arabia. The aim of this study was to investigate the prevalence of antibacterial resistance and genotypic characterisation in enterococci isolated from clinical samples in two hospitals in Riyadh, KSA. Materials and Methods Study design and data collection Specimens were collected for this study over the period from January 2009 to March 2010. They included 32 urine specimens, 30 blood samples, 17 burn swabs, 12 throat swabs, 11 swabs of bed sore, 14 drains and catheter, 47 stools, 18 pus swabs, 16 body fluid, 19 abscess swabs and 24 wound discharge, collected from in-patients and out-patients at King Khaled University (KKU) Hospital (140 specimens) and King Saud Medical City (KSMC) Hospital (100 specimens), Riyadh, Saudi Arabia. A total of 206 enterococci were isolated from these 240 patients with nosocomial infections according to the Centers for Disease Control and Prevention (CDC) definition. [1] We used trypticase soy agar supplemented with 5% sheep blood (BBL, Cockeysville, MD, USA) to isolate enterococci from urine, wounds and sterile body fluids. Stool samples were inoculated into enterococcal broth, incubated overnight at 35°C and subcultured onto brain heart infusion agar (BHIA) (Difco Laboratories, Detroit, MI, USA) containing 6 μg vancomycin/ml and onto BHIA without vancomycin to recover vancomycin-susceptible isolates. Presumptive identification of enterococci was based on their growth characteristics on blood agar, Gram staining, the catalase reaction, ability to grow in 6.5% NaCl broth and bile esculin hydrolysis and biochemical tests using API Strep (bioMe΄rieux, Marcy l′Etoile, France). After the identity of the isolates was confirmed, they were stored in trypticase soy broth containing 16% glycerol at −70°C in freezer vials pending for further analysis. The patients enrolled in the study were monitored daily until discharge for the subsequent development of a nosocomial infection (bacteremia, pneumonia, wound infection, etc.). Ethical approval to perform the study was obtained from the management boards of these hospitals and the Saudi Ministry of Health. Antimicrobial susceptibility testing The susceptibilities of all isolates to different antimicrobial agents were tested by the disc-agar method as standardised by the Clinical Laboratory Standards Institution (CLSI). [8] The following antimicrobial discs and concentrations were used: ampicillin (10 μg), vancomycin (30 μg), teicoplanin (30 μg), erythromycin (15 μg), ciprofloxacin (5 μg), chloramphenicol (30 μg), amikacin (200 μg), gentamicin (10 μg), kanamycin (200 μg), streptomycin (300 μg), tetracycline (30 μg) and linezolid (30 μg) (Becton Dickinson Microbiology Systems, BBL, Cockeysville, MD, USA). The results were recorded after 24 h of incubation at 35°C and after 48 h for streptomycin. Quality control strains of E. faecalis (ATCC 51299) were used to ensure the potency of each antimicrobial agent tested. With the exception of vancomycin, susceptibility interpretations followed the guidelines proposed by the CLSI. Minimum inhibitory concentrations (MICs) for vancomycin and teicoplanin were determined using E-test strips (AB Biodisk, Solna, Sweden). MICs for gentamicin, kanamycin, streptomycin, amikacin and linezolid were determined by the agar dilution method. For this study, vancomycin resistance was defined as any enterococcal isolate with an MIC to vancomycin of at least 16 μg/ml. [8] Vancomycin resistance was confirmed by hybridisation to specific gene probes. The specific vancomycin-resistant genotype (vanA, vanB or vanC) was determined with polymerase chain reaction (PCR) analysis by using specific primers selected from published gene sequences. [9] β-Lactamase production and inhibition tests The ability of the isolates to produce β-lactamase was detected with nitrocefin (Oxoid, USA) according to the manufacturer's instructions. Nitrocefin solution (5 μl) was dropped onto a loopful of pure overnight growth placed on a filter membrane. The development of a red colour within 60 s indicated a positive result. S. aureus strain ATCC 29213 was used as a positive control. [4] Confirmatory tests were performed by the disc-agar diffusion method with amoxicillin-clavulanic acid (AMC 30 μg) and ampicillin-sulbactam (SAM 20 μg) discs (Difco Laboratories), as recommended by the CLSI. [8] DNA isolation Isolates of VRE were grown overnight at 37°C on bile aesculin agar (Difco Laboratories). The colonies were cultured in 30 ml of brain heart infusion broth (Difco Laboratories) and were harvested during logarithmic growth (optical density at 590 nm of 0.8). DNA was prepared by using a modification of the initial steps of the method of Crosa and Falkow [10] to recover both chromosomes and large plasmids. The bacterial pellet was suspended in 1.5 ml of 25% sucrose-0.05 M Tris-0.001 M ethylenediaminetetraacetic acid (EDTA; pH 8); 0.2 ml of a freshly prepared 40 mg/ml solution of egg white lysozyme (Boehringer Mannheim, Mannheim, Germany) in 0.25 M Tris (pH 8) was added. After incubation for 30 min at 37°C, the bacteria were lysed by adding 0.1 ml of 0.25 M EDTA (pH 8) and 0.1 ml of 20% sodium dodecyl sulphate (SDS). NaCl was added to 1 M; this was followed by incubation on ice for 30 min, centrifugation at 30,000× g at 4°C for 30 min, and incubation of the decanted clear lysate with 5 ml of a 5 mg/ml solution of bovine pancreatic RNase (Boehringer Mannheim) for 30 min at 37°C. DNA concentrations were estimated by electrophoresis on 1% agarose gels (Hispanagar; Sphaero Q, Leiden, The Netherlands) containing ethidium bromide in the presence of known quantities of lambda DNA as references. Detection of vancomycin-resistance determinants Genes encoding the vancomycin resistance determinants, vanA vanB, vanC and vanD, were investigated by PCR using specific primers, as described by Dutka-Malen et al. [Table - 1]. [9] For the detection of Van genotypes, the eight VRE and intermediate resistant (IR) strains were investigated for their vancomycin-resistant genotypes by PCR. Amplification was performed using a kit from Gibco-BRL. DNA for PCR was isolated as described previously. [4] The amplification mixture consisted of 45 μl Supermix (22 mM Tris/HCl, pH 8.4; 55 mM KCl; 1.65 mM MgCl 2 ; 220 μM each dNTP; 22 U recombinant Taq DNA polymerase/ml; 3 μl bacterial DNA and 2 μl primer solution in a total reaction volume of 50 μl. A Perkin Elmer 9600 thermocycler was programmed for 32 cycles with the following parameters: denaturation at 94°C for 3 min, annealing at 60°C for 45 s, extension at 72°C for 1 min and final extension at 72°C for 2 min. Amplicons were analysed by electrophoresis on 1% agarose gels (Hispanagar; Sphaero Q) containing ethidium bromide in TAE buffer for 2 h at 70 V in the presence of a 100-bp DNA ladder (Gibco/BRL Life Technologies, Breda, The Netherlands). E. faecalis strain E206 (vanA) and E. faecium E2781 (vanB) were used as controls in the PCR experiments. Restriction fragment analysis by pulsed field gel electrophoresis Chromosomal DNA was obtained as described by Kaufmann. [11] Purified DNA was digested with the restriction enzyme SmaI (GIBCO BRL, New York, USA) and separated by pulsed field gel electrophoresis (PFGE) in 1% agarose gels, using a CHEF-DRII system (Bio-Rad Laboratories, Richmond, CA, USA). The pulse time was increased from 5 to 35s, over 22 h, at 5.9 V/cm at a temperature of 11oC and an angle of 120 o. Lambda ladder of 48.5 kb concatamers (New England BioLabs, Beverly, MA, USA) was used as the molecular weight marker. Gels were stained with ethidium bromide and photographed under UV light. Analysis of DNA restriction profiles was performed by visual inspection according to Tenover et al. [12] Results Enterococci isolates The distribution of species and sources is shown in [Table - 2]. Between January 2009 and March 2010, 240 hospitalised and non-hospitalised patients with active infections were enrolled in this study. A total of 206 enterococcal isolates from various clinical samples were obtained from 24 wound discharge (8.8%), 32 urine cultures (10.8%), 14 urinary catheter (4.6%), 16 body fluid (2.9%), 30 blood cultures (12.1%), 17 burn swabs (6.3%), 12 throat swabs (4.2%), 47 stools (19.2%), 18 pus (6.7%), 19 abscess (7.1%), and 11 bed sore swabs (3.3%). Six different species were identified, of which E. faecalis was the most prevalent. Out of 206 enterococcal isolates, 166 (69.2%) were identified as E. faecalis, 27 (11.3%) as E. faecium, 5 (2.1%) as E. avium, 2 (0.8%) as E. hirae and 3 (1.3%) as E. casseliflavus and E. gallinarum. The mean age of the study participants was 57.7 years; 278 of them (91.1%) were males. Two hundred and six enterococcal isolates (85.0%) were recovered from ICU; 112 (46.7%) from surgical ward, 67 (27.9%) and 27 (11.3%) internal medicine ward. Antibacterial resistance pattern The distribution of antimicrobial susceptibility patterns of isolated enterococci is summarised in [Table - 3]. The results show that the majority of isolates were resistant to tetracycline (66.5%), erythromycin (64.1%), ciprofloxacin (49.9%) and chloramphenicol (34.5%). High-level resistance to gentamicin (MIC > 500 μg/ml), kanamycin (MIC > 1000 μg/ml), amikacin (MIC > 512 μg/ml) and streptomycin (MIC > 2000 μg/ml) was detected in 20.9, 19.9, 22.8 and 19.4% of the isolates, respectively. In addition, 47 (22.8%) of the isolates were resistant to ampicillin (MIC > 16 μg/ml). However, none of them produced β-lactamase. The isolates were tested for their susceptibility to linezolid, a new oxazolidinone antibacterial. They were susceptible to linezolid (MIC range: 0.5-4 μg/ml) except one isolate (0.5) of E. faecium. The antibacterial resistance profiles and van genotypes of VRE isolates are summarised in [Table - 4]. Vancomycin and teicoplanin resistance were detected in 8 (3.9%) isolates consisting of five E. faecium and three E. faecalis (MICs > 32 μg/ml, VanA phenotype). One strain had intermediate resistance to vancomycin (MICs from 6 to 12 μg/ml) and was sensitive to teicoplanin (MICs from 0.25 to 1 μg/ml, VanB phenotype). Three E. gallinarum and one E. casseliflavus strains had intermediate resistance to vancomycin (MICs from 6 to 12 μg/ml) and were sensitive to teicoplanin (MICs from 0.25 to 1 μg/ml, VanC phenotype). All of the vancomycin-resistant isolates expressed low MIC values for linezolid (MIC < 2 μg/ml). The VRE isolates were also resistant to different antibiotics including erythromycin, ciprofloxacin and high-level streptomycin [Table - 2]. Detection of van genotypes All of the seven resistant strains were positive for VanA genotype and a 732-bp PCR product was obtained in all the positive isolates. VanB products (635 bp) were detected in one intermediate resistant isolate as shown in [Table - 3] and [Figure - 1] and [Figure - 2]. PCR of the vanC gene with a product size of 822 bp was obtained from E. gallinarumspecimens [Figure - 3]. No vanD products were detected in any of the isolates. PFGE of vancomycin-resistant isolates The vancomycin-resistant isolates were typed by PFGE after SmaI digestion of their genomic DNA. The genetic profile of eight isolates of VRE was examined and we found the existence of five isolates with identical profile (clone A). Five isolates proved to be highly correlated to the clone A and were considered to belong to this major clonal group [Figure - 4]. These isolates were obtained from different patients who had been admitted to different wards in the same hospital. One isolate was from a blood sample and the other was from a urine sample. The remaining E. faecalis isolated strain had different PFGE patterns [Figure - 4]. Similarly, the three E. faecium isolates had different PFGE patterns. Discussion During the period from January 2009 to March, 2011, we examined different clinical samples from 240 patients for the presence of VRE at Riyadh Hospitals. The vast majority of the isolates in this study were either E. faecalis which caused about 69.2% infection or E. faecium which was responsible for about 11.3% of infection, while E. avium, E. hirae, E. casseliflavus and E. gallinarium accounted for only 6.3% of the isolates, which was comparable to the distribution of enterococcal species in other studies. [13] This species distribution is similar to that reported from different parts of the world including Saudi Arabia, [14] but it is in disagreement with reports from some other countries where E. faecium was predominant over E. faecalis. [15] The prevalence of E. faecium in this study was 11.3% higher than the prevalence reflected in a similar study from Saudi Arabia. [16] E. faecium has also been reported as the most common species in other studies [8],[16] The isolated enterococci were detected mostly in the blood, urine, stool and wound discharge. These results are in conformity with the other previous reports. [8],[16] Enterococci are intrinsically resistant to several antimicrobials and can develop resistance to many others, which complicates treatment of their infections. [4] Of the 206 isolates, 66.5, 49.0 and 34.5% were resistant to tetracycline, ciprofloxacin and chloramphenicol, respectively, which are similar to the levels reported for these antibacterials among the enterococci isolated in Jordan [17] and in a previous study in Saudi Arabia. [18] Frequency of resistance to the commonly used antimicrobials was slightly higher among isolates of this study than that reported from other countries like Kuwait [4] and Lebanon. [19] In this study, 64.1% of isolates were resistant to erythromycin, which is lower than what was reported from other countries such as India (85%) and Lebanon (59%). [13] These results indicate diverse geographical distribution of erythromycin-resistant enterococci. Antimicrobial resistance has been consistently reported to be more common in E. faecium as compared to E. faecalis.[4],[17],[18] Enterococci with VRE are being reported from different parts of the world with increasing frequency, although the epidemiology of these microorganisms varies widely in different geographical areas. [20] The percentage of reported hospital enterococcal infections resistant to vancomycin increased from 0.3% in 1989 to 11% in 1996. [21] In this study, VRE were found in 8 (3.9%) patients and all were identified as E. faecalis and E. faecium. Medical records of these eight patients were reviewed and their clinical features were determined. The patients were immunocompromised and their age varied from 56 to 72 years. All the patients except one were inpatients when VRE was detected in their specimen. This patient was a male with renal complications and a long history of urinary tract infection (UTI), and he visited the health clinic as an outpatient periodically. These results are in agreement with those of Udo et al. [8] who detected VRE in 11 out of 415 isolates (2.6%) at Kuwait hospitals. However, our results are not in agreement with those of Gambarotto et al. [18] who reported that the incidence of VRE in hospitals was 26/70 (37%) and was 20/169 (11.8%) in non-hospitalised individuals. Also, Leven et al. [19] reported the incidence in 586/1260 (46.5%) patients in University hospital in Belgium. All of the isolates were susceptible to linezolid except one. Also, 98.2% of the E. faecalis in this study were vancomycin susceptible. The low prevalence of vancomycin resistance among the isolates in this study indicated that vancomycin retains its therapeutic efficacy against the majority of enterococci isolated from patients in Saudi hospitals. The resistance rate to ampicillin was found to be 22.8% in enterococcal isolates. However, resistance rate to ampicillin reported by Mathur et al. in India (66%) is higher than our result. It has been previously reported that β-lactamase production is a rare event in enterococci and the present study has also corroborated this.[8] Since ampicillin is the drug of choice in the treatment of enterococcal infections, the relatively high resistance of isolates in this study to ampicillin is of great concern, especially in the case of endocarditis treatment. The isolates expressing high-level resistance to amikacin, gentamicin, kanamycin and streptomycin were 22.8, 20.9, 19.9, and 19.4, respectively. The detection of high-level gentamicin resistance in 22.3% of E. faecalis and 18.5% of E. faecium isolates is a cause for concern, as it may signify the beginning of a major resistance problem. This study investigated the prevalence of genes encoding vancomycin resistance in enterococci isolated from clinical samples in Saudi Arabia hospitals. Vancomycin-resistant phenotypes in enterococci have been classified as VanA, VanB, VanC, VanD and VanE, based on levels of resistance, cross-resistance to teicoplanin and inducible or constitutive nature of the resistance. [6] In enterococci, two principal phenotypes of acquired vancomycin resistance have been described, VanA and VanB. The VanA determinant is carried on transposon Tn1546 or close relatives that are transferable in conjugation experiments. [6] In our study, vanA was found in 87.5% of the isolates and strains, with a VanA phenotype possess high-level resistance to both vancomycin and teicoplanin (vancomycin MIC > 256 μg/ml , teicoplanin MIC > 128 μg/ml), whereas strains with a VanB phenotype possess only moderate to high levels of vancomycin resistance (vancomycin MIC ≥ 1024 μg/ml, teicoplanin MIC < 1 μg/ml). In this study, seven E. faecalis and one E. faecium isolates expressed vancomycin-resistance patterns compatible with the VanA and VanB phenotypes, respectively, and all gave positive results in PCR experiments for the vanA and vanB genotypes. However, different studies showed variable results concerning the detection rates of VanA and VanB. In Kuwait hospitals, all VRE strains carried the VanA genotype, non VanB product was detected in any of the isolates [4] in contrast to Nelson et al. [22] who reported that the majority of isolates (97%) were VanB positive and the remaining isolates were VanA genotype. Motile enterococci, including E. gallinarum and E. casseliflavus, are rarely encountered in human clinical specimens and are primarily found in the gastrointestinal tract of poultry, in foods, and in domestic fowls. Although these species are infrequently isolated from clinical specimens, they have been implicated in a wide variety of invasive infections in humans, especially immunocompromised or chronically ill patients, and sometimes are nosocomially acquired. [4],[6] In our study, E. gallinarum, a rare enterococcal species in human infections, was encountered, thereby emphasising the need to speciate the genus Enterococcus encountered in human infections. In this study, vanC1 was detected in three isolates of E. gallinarum. The MICs of vancomycin and teicoplanin were 8 and 0.5 μg/ml, respectively. E. gallinarum and the other motile enterococci are thought to be infrequently causing infection and these strains were isolated from urine specimens in the ICU. Our results are comparable with the results of Descheemaeker et al. [20] They studied the prevalence and molecular epidemiology of glycopeptide-resistant enterococci (GRE) in Belgian renal dialysis units and they detected vanC1 gene in urine samples. As demonstrated by molecular typing, there was a predominant clone among the isolates of VRE (E. faecalis). As this clone was obtained from isolates of patients attending two hospitals (KKUH and KSMC) during a short time-frame period, it is possible to consider that there was an intra- and inter-hospital dissemination of VRE. This is the first report of a major clonal VRE spread in two hospitals of Riyadh. In fact, we found a considerable genetic diversity among VRE in our study. It is noteworthy that clonal dissemination of VRE has already been described in the state of Riyadh in previous years. [18] The identification of a major clonal group in VRE draws attention to the increasing need for control measures to avoid horizontal transmission, since the enterococci currently represent a serious problem in health institutions, especially because of the possibility of spread from healthy carriers and the lack of effective treatment options. Although the prevalence of vancomycin resistance was low among the studied isolates, their presence together with high-level aminoglycoside resistance calls for regular surveillance studies, infection control and monitoring of antibiotic sensitivity among hospital-isolated strains. Presence of vanA, vanB and vanC gene cluster in some of our isolates can provide transfer of vancomycin resistance via conjugative plasmids not only to enterococci species but also to other bacteria such as S. aureus. So, we expect an increase in the number of VRE in the future. The appearance of these highly resistant strains prompted us to do a series of studies to assess the extent of colonisation and infection with VRE in our patient population, to define risk factors for acquisition and to evaluate the effect of interventions on rates of colonisation and infection. Acknowledgment This project was supported by the Research Center, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia for the generous financial support. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12009f3.jpg] [mb12009f1.jpg] [mb12009t4.jpg] [mb12009f2.jpg] [mb12009t1.jpg] [mb12009f4.jpg] [mb12009t2.jpg] [mb12009t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}