 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
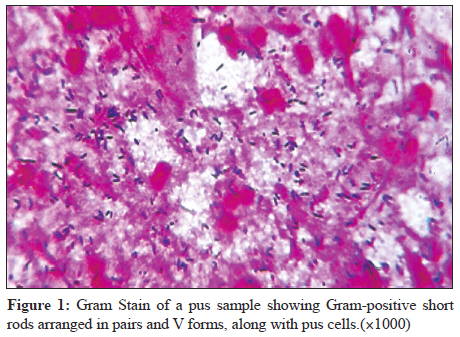
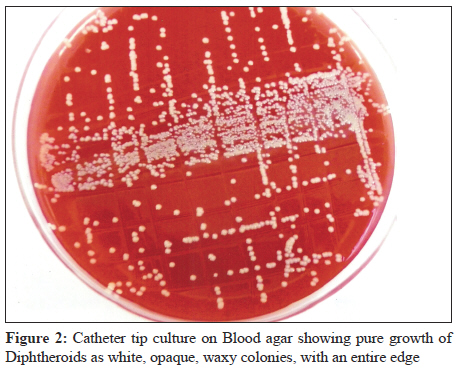
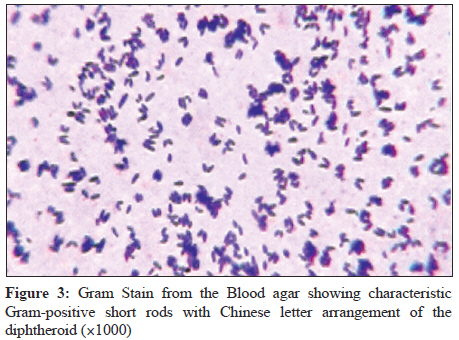
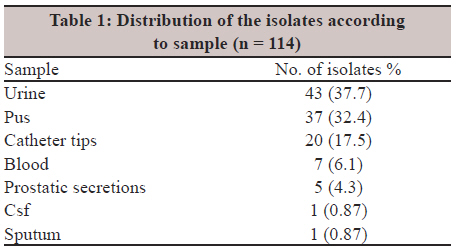
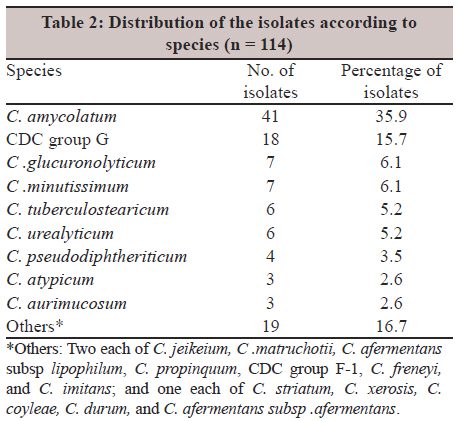
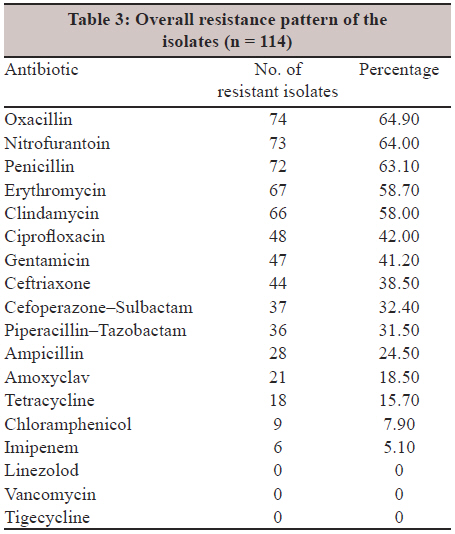
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 52-57 Original Article Isolation, speciation, and antibiogram of clinically relevant non-diphtherial Corynebacteria (Diphtheroids) BS Reddy, A Chaudhury, U Kalawat, R Jayaprada, GSK Reddy, BV Ramana Department of Microbiology, Sri Venkateswara Institute of Medical Sciences, Tirupati - 517 507, Andhra Pradesh, India Correspondence Address: Date of Acceptance: 08-Nov-2011 Code Number: mb12010 PMID: 22361761 DOI: 10.4103/0255-0857.93033 Abstract Purpose: Coryneform or the non-diphtherial Corynebacterium species largely remains a neglected group with the traditional consideration of these organisms as contaminants. This concept, however, is slowly changing in the light of recent observations. This study has been done to find out the species distribution and antibiogram of various members of the clinically relevant Coryneform group, isolated from various clinical materials. Keywords: Antibiogram, Corynebacterium, diphtheroids, speciation Introduction Non-diphtherial Corynebacteria, which are also referred to as Diphtheroids, are a widely diverse collection of bacteria. Up to now, the pathogenic potential of coryneform bacteria has been underestimated. Although frequently considered as contaminants, these organisms have been associated with invasive disease, particularly in immunocompromised patients. Species like C. amycolatum, C. jeikeium, C. minutissimum, and C. urealyticum are being reported with increasing frequency in recent years. These organisms have been implicated in multiple infections like catheter-associated blood stream infections, endocarditis, prosthetic valve infections, meningitis, neurosurgical shunt infection, brain abscess, peritonitis, osteomyelitis, septic arthritis, urinary tract infections, empyema, and pneumonia. [1] The importance of these isolates in clinical settings is still undermined, as evidenced by the lack of comprehensive data with a large number of isolates. It is clearly stated that the recognition of infections caused by coryneform bacteria is highly dependent on the laboratory personnel′s ability to identify these species. [2] Most often these isolates are dismissed as mere contaminants in the laboratory setting, without going into the details of the patient profile or repeat microbiological analysis. This problem is aggravated by the fact that until recently, the Clinical and Laboratory Standards Institute (CLSI) had not published any specific guidelines for the susceptibility testing of coryneform bacteria, in particular for fastidious organisms like lipophilic corynebacteria. Only recently the CLSI has proposed a reference microdilution method for testing these organisms. [3] However, at present, there are no specific guidelines with regard to the disc susceptibility testing method. Partly for this reason, antimicrobial susceptibility patterns of coryneform bacteria have not been studied systematically. Very few comprehensive studies on this subject are extant. [4],[5] A few other studies have focused on particular organisms such as Corynebacterium jeikeium,[6] and C. urealyticum.[7] Reports on this group of organisms from India are sparse, except for a rare case report concerning a particular species. [8] No large scale study is available from this country regarding the distribution of these species in various clinical samples, and their true clinical significance. As a consequence, there is a total absence of the antimicrobial susceptibility pattern of the coryneform organisms in Indian settings, and we have to depend only on western data. For these reasons, this prospective study has been performed, to find out the spectrum of the species of organisms belonging to the genus Corynebacterium that actually cause clinical infections, and to determine their antimicrobial susceptibility. Materials and Methods It was a prospective study and the clinical samples submitted to the Microbiology Department were processed during the period of April 2009 to October 2010. Culture was performed on sheep blood agar and MacConkey's agar as part of the routine procedure, with additional chocolate agar for the cerebrospinal fluid (CSF) and sputum samples. The following scheme was adopted to find out the true clinical significance of the isolates: (a) Urine: A repeat sample was collected if the overnight culture of the first sample grew the organisms as a pure growth, at a count of 104CFU / ml, or as a predominant organism with a total count of 105CFU / ml. [2],[9] (b) Pus, Sputum, Prostatic secretions, CSF: Presence of Gram-positive rods in the stained sample and growth of similar coryneforms after overnight incubation were considered significant [Figure - 1]. [9] A repeat sample of pus was collected on the same day after observing the Gram smear and after making sure that no antibiotic treatment had been instituted. For CSF and prostatic secretions, a second sample could not be collected. (c) Blood: Two blood samples collected from two different sites growing the same organism was considered significant. (d) Catheter Tips: A roll plate culture growing > 15 colonies and / or a phosphate buffered saline (PBS) vortexed sample growing > 103CFU / ml were taken as significant [Figure - 2]. Vortexing of the catheter tip in PBS was done, followed by plating, to isolate the intraluminal bacteria that could not be obtained by the roll plate technique. For all samples, except blood, direct smear for a Gram stain was done. For urine, the repeat sample was Gram stained after centrifugation. Wet mount preparation of the urine was also done, to find out if pyuria was present. The plates were incubated for 48 hours (except urine and sputum) at 37°C. For all specimens, isolation as pure growth or repeated isolation or a significant growth were considered significant. [9] In all cases, tiny pinpoint colonies were seen on MacConkey's agar in addition to growth on blood agar, and the smear from these pinpoint colonies had revealed similar Gram positive rods [Figure - 3]. Diphtheroids grown from the samples were first Gram stained to see the characteristic morphology. Speciation was done based on the panel of reactions described by von Graevenitz and Funke, [10] which included a catalase test, test for fermentation or oxidation, motility, nitrate reduction, urea hydrolysis, esculin hydrolysis, alkaline phosphatase test, acid production from glucose , maltose, sucrose, mannitol, and xylose, Christie, Atkins, Munch-Peterson (CAMP) reaction with a beta hemolysin producing strain of Staphylococcus aureus, and a test for lipophilism. The antibiogram was determined by the disc diffusion method on 5% sheep blood agar. One percent Tween 80 was added to this medium when testing the susceptibility for lipophilic corynebacterial species. The following antibiotic discs were used for testing: Ampicillin (10 μg), amoxicillin-clavulanic acid (20 / 10 μg). cefaperazone-sulbactum (75 / 10 μg), ceftriaxone (30 μg), chloramphenicol (30 μg), clindamycin (2 μg), erythromycin (15 μg), Ciprofloxacin (5 μg). Nitrofurantoin (300 μg), gentamicin (10 μg), imipenem (10 μg), linezolid (30 μg), oxacillin (1 μg), penicillin (10 units), piperacillin-tazobactum (100 / 10 μg), tetracycline (30 μg), vancomycin (30 μg), and tigecycline(15 μg). Due to the lack of established CLSI guidelines for the disc diffusion method, for this group of organisms, the following approach was adopted: (a) The British Society for Antimicrobial Chemotherapy (BSAC) guidelines were followed when testing for ciprofloxacin, penicillin, and vancomycin. [11] (b) For other antibiotics, the CLSI guidelines applicable for Staphylococcus aureus, with an S.aureus ATCC 25923 control strain, were used. [12],[13] (c) For reporting cefoperazone-sulbactam sensitivity, the recommendations of the manufacturer were adopted. The disc content was 30 mcg Cefoperazone / 75 mcg sulbactam. The interpretation was as follows: susceptible: ≥ 21 mm, Intermediate: 16 - 20 mm, resistant:≤ 15 mm. For quality control: S.aureus ATCC 25923 zone size was 23 - 30 mm. Results A total of 114 isolates belonging to the genus Corynebacterium were studied and were subjected to speciation. A majority of these isolates were obtained from urine, pus, and catheter tips, together constituting 87.7% of the total isolates, with urinary isolates comprising of a maximum of 37.7% [Table - 1]. Among 43 urinary isolates, only 11 were obtained in pure culture and the remaining were obtained in mixed cultures, with diphtheroid being the predominant isolate, with a significant colony count, as mentioned earlier. All the urine samples had shown > 1 pus cell / 7 HPF in a wet mount of the uncentrifuged sample, which corresponded to a significant pyuria of 104 WBC / ml. All the isolates obtained from the clinical samples, other than urine, were in pure form. For the single CSF sample obtained from a suspected acute meningitis case, a moderate number of pus cells were seen on a Gram stain cytospin deposit, along with a few short Gram-positive rods. More than 20 different species were isolated and identified in our series. C. amycolatum was the predominant species (35.9%) followed by CDC group G (15.7%) and together they represented more than half of the total isolates (51.6%) [Table - 2]. C. amycolatum was the most commonly isolated species among the catheter tips, urine, and pus samples. Although the number of C. amycolatum species isolated was more in the pus samples, the relative occurrence of this species was more among the catheter tip isolates, constituting around 55% of the total catheter tip isolates. The majority of the CDC group G species were recovered from the pus samples and catheter tips, together constituting 77.7%, with very little isolation or none from other clinical samples. Most of the C. minutissimum and almost all the C. urealyticum strains were recovered from the urinary isolates. The overall resistance pattern of the isolates [Table - 3] showed high frequency of resistance (> 50%) to penicillin, oxacillin, erythromycin, and clindamycin, and more than 40% of the strains were resistant to ciprofloxacin and gentamicin. Excellent activities were shown by vancomycin, linezolid, and tigecycline, to which all the isolates were sensitive. During the study period, a close liaison was maintained with the clinicians concerned, keeping in mind the problems in interpretation of the laboratory results. Only when a repeat sample grew the same organism, the clinician initiated the treatment. In other cases, the clinician would start the empirical therapy and modify the antibiotic based on the culture results, if necessary. The treatment outcome was uniformly good with the addition of vancomycin, as and when necessary. Discussion Corynebacterium species other than C. diphtheriae, are being reported with increasing frequency as potential pathogens, especially nosocomial pathogens. With the duration and intensity of immunosuppression that patients are now subjected to and the increased use of indwelling intravenous devices, the role of coryneform bacteria has became more significant than in the past. As far as the various species are concerned, differences have been observed among Corynebacterium species, most commonly recovered from human clinical materials, by several authors, and no uniformity has been observed regarding this on the whole. Although earlier studies had found C. jeikeium, C. striatum, and C. xerosis the most common organisms, recently there has been an increased rate of isolation of C. amycolatum strains, probably because these organisms have been misidentified in the past. [14] In our study C. amycolatum was the most commonly isolated species accounting for 35.9% of the total isolates. It was the most frequently isolated species from all the specimens, including urine, pus, and catheter tips. Lagrou et al[15] have reported a similar finding, with a 53% isolation rate of this organism, which was the predominant organism in their series. This species is at present emerging as an important causative agent in infectious conditions, partly on account of our greater acquaintance and improved identification techniques for these organisms and partly on account of the growing number of immunocompromised patients in whom their pathogenic role is increasingly being established. The second most common species, accounting for 15.7% of the total isolates, was CDC group G. It was isolated in greater frequency from catheter tips and pus. It was less frequently isolated from urine Although CDC group G has not been found to be a significant pathogen in most studies, two studies by Williams et al.[16] and Olender and Ketowska [17] have found them to accountfor 12 and 16.7% of the infections, , respectively in various sites. Our observations correlate with their findings. There was one single isolate from CSF and the organism was CDC group G. The patient had classical signs of acute meningitis. The patient was started empirically on Inj. Ceftriaxone IV as per the antibiotic policy of our institute. As the isolate was found to be sensitive to ceftriaxone, the same treatment was continued and the patient made an uneventful recovery. C. minutissimum and C. glucuronolyticum were isolated in a frequency of 6.1% each. Both these species were predominantly isolated from urine samples. Isolation of C. minutissimum at a frequency of 6.1% in our series roughly corresponded to an earlier study, where the rate was 6%. [17] C. tuberculostearicum and C. urealyticum constituted 5.2% each among the isolates. All the C. urealyticum species were exclusively isolated from urine with no isolation from the other samples, whereas, C .tuberculostearicum was mostly isolated from the pus samples, . C. pseudodiphtheriticum was the only species isolated from sputum. The other species like C. atypicum, C. aurimucosum, C. jeikeium, C. matruchotiiwere isolated less frequently, (accounting for less than 3% each among the total isolates). Most recent studies show an alarming rate of antibiotic resistance among the Corynebacterium species. Resistance to β-lactams, clindamycin, erythromycin, ciprofloxacin, and gentamicin is quite frequent, sometimes leaving vancomycin the only drug of choice. To date, vancomycin and teicoplanin are the agents that are most active against corynebacteria in vitro. In recent times, tigecycline has also shown good activity against these organisms. In our study all the isolates were uniformly susceptible to vancomycin, linezolid, and tigecycline and a majority of the isolates were susceptible to imipenem, chloramphenicol, and tetracycline. On the other hand, a majority of the isolates were resistant to penicillin, oxacillin, and nitrofurantoin, followed by resistance to erythromycin and clindamycin . C. amycolatum, the predominant organisms in our study showed high frequency of resistance to nitrofurantoin, penicillin, oxacillin, erythromycin, clindamycin, ciprofloxacin, and gentamicin. The isolates were relatively less resistant to chloramphenicol, amoxyclav, and tetracycline. These results were in accordance with the previous studies. [18],[19] Most of the CDC group G strains in the present study were resistant to penicillin which was similar to the findings of Weiss et al.[20] with 80% resistance along with high resistance to nitrofurantoin clindamycin, erythromycin and ciprofloxacin, Relatively less resistance was observed to tetracycline. C. glucuronolyticum strains in the present study were highly resistant to clindamycin erythromycin, and nitrofurantoin These observations were comparable to the findings of Turk et al.,[19] where a majority of C. glucuronolyticum strains were resistant to clindamycin erythromycin and nitrofurantoin Among all the species, isolated C. amycolatum, CDC group G, C. jeikeium, C. matruchotii, and C. glucuronolyticum were the species showing a high level of resistance to multiple antibiotics(three or more) followed by C. tuberculostearicum and C. urealyticum. The other species isolated were relatively more sensitive to antibiotics. Isolates from catheter tips, pus, and blood samples, showed higher resistance frequency compared to isolates from urine, prostatic secretions, sputum, and CSF. It was noted that isolates from catheter tips were extremely resistant to antibiotics like clindamycin and erythromycin. Resistance to gentamicin was also much higher (90%) among the catheter isolates, when compared to isolates from other samples. Multidrug resistant organisms were also much more frequently recovered from catheter tips than from other clinical samples. The resistance patterns of these organisms also vary according to the sample from which they have been isolated. Organisms isolated from catheter tips show a very high level of resistance followed by pus and blood. Isolates from catheter tips are highly resistant to clindamycin, erythromycin, gentamicin, and nitrofurantoin. The relatively high rate of resistance shown by catheter isolates goes to prove that these are hospital strains that are frequently multidrug resistant. The catheter tips are from the internal jugular vein or femoral vein, mostly from haemodialysis patients. However, we have not found similar isolates from blood culture and central venous catheter tips, thus ruling out catheter-associated blood stream infection. The isolates from the catheter are presumably from immature / mature biofilms, which have got a potential to lead to blood stream infection. Urinary isolates and isolates from prostatic secretions have shown relatively less resistance. The identification of Coryneform bacteria remains a challenge for routine diagnostic laboratories, because of the large array of species belonging to this group, compounded with the problem of infrequent isolation of many of these organisms. Due to the fact that almost all of them form part of a commensal flora at one or the other site in the body absolute judgment is needed to find out its clinical significance. Multiple tests are needed to accurately identify these isolates to the correct species level most of which are almost never used in routine laboratories. Molecular methods and sequencing of the isolates could have given us a more reliable identification of the organisms, but due to several constraints, of sequencing of more than 100 isolates it was not feasible. The focus of our study was on the frequency of isolation of various species of non-diphtherial coryneforms and their antimicrobial resistance pattern, as almost no data regarding the same was available from India. Direct and indirect evidences mentioned in the methodology suggest that the samples have reflected definite infection in the particular organ / system. Coryneform bacteria are to be considered as clinically significant organisms whenever they are isolated in pure culture, or isolated from a sterile site, or isolated repeatedly. [9] Speciation and determination of the antibiotic sensitivity need to be performed for such isolates. Determining the antibiogram of these Corynebacterial species is necessary as species like C. jeikeium, C. urealyticum, and C. amycolatum are highly resistant to many of the commonly used antibiotics including β-lactams, macrolides, and fluoroquinolones. Nowadays, species like C. amycolatum and CDC group G are increasingly recovered from clinical specimens and recognized as potential pathogens, especially in debilitated patients and as hospital-acquired pathogens. These organisms also show a variable resistance pattern to different antibiotics. Fortunately, most of these multidrug resistant Corynebacterial species are susceptible to glycopeptide antibiotics, which justify their use as first-line empirical drugs against serious infections caused by these organisms. Tigecycline, the newer glyacylglycine antibiotic, can also be considered for treatment, as a substitute to glycopeptide antibiotics. In the current study all the isolates have been uniformly sensitive to tigecycline. Emerging antimicrobial resistance in various species has created an additional need for accurate identification of coryneform organisms to the species level and continuous surveillance of their resistance patterns. In this study, the importance of the need to take coryneform bacteria into consideration, especially as pathogens of opportunistic and nosocomial infections, and the importance of assessing their antibiotic sensitivity is emphasized. Our data can provide guidance for the clinician to start an appropriate empirical or specific antibiotic therapy. Acknowledgment Miss Vasavi , Technical Staff, Department of Microbiology. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12010t2.jpg] [mb12010f1.jpg] [mb12010t1.jpg] [mb12010f2.jpg] [mb12010f3.jpg] [mb12010t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}