 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
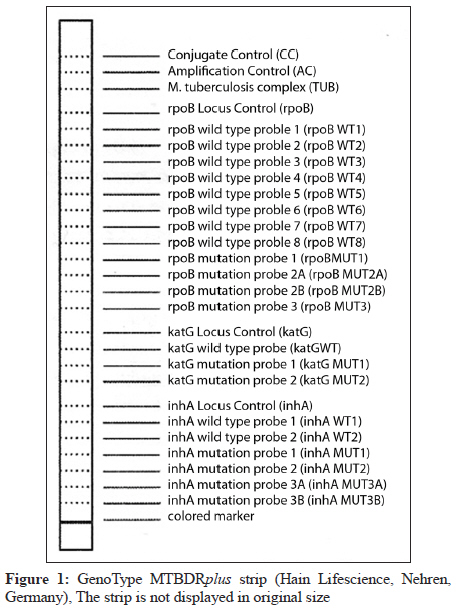
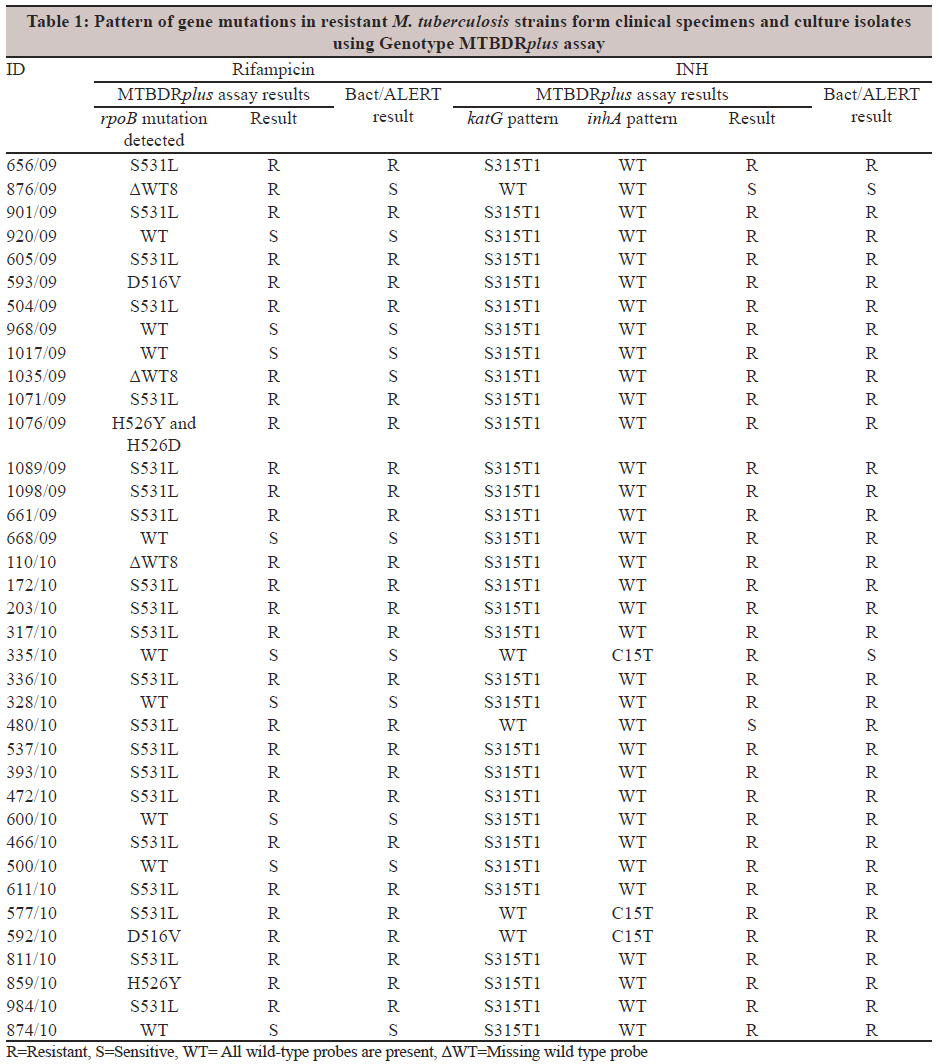
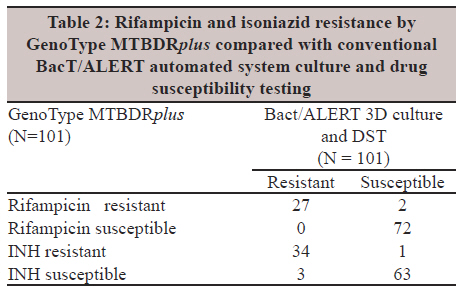
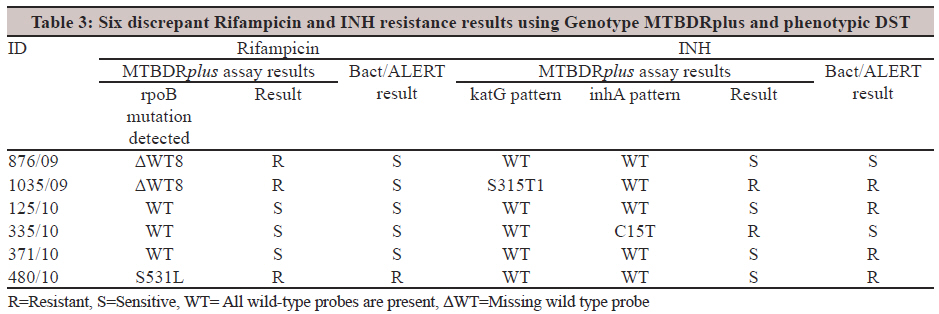
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 58-63 Original Article Utility of GenoType MTBDRplus assay in rapid diagnosis of multidrug resistant tuberculosis at a tertiary care centre in India R Raveendran, C Wattal, JK Oberoi, N Goel, S Datta, KJ Prasad Department of Clinical Microbiology and Immunology, Sir Ganga Ram Hospital, New Delhi - 110 060, India Correspondence Address: Date of Acceptance: 04-Dec-2011 Code Number: mb12011 PMID: 22361762 DOI: 10.4103/0255-0857.93034 Abstract Purpose: Molecular methods which allow rapid detection of tuberculosis as well as drug resistance directly from clinical samples have become the most popular diagnostic methodology with the emergence of multidrug resistant tuberculosis. The aim of the present study was to evaluate the performance of a line probe assay, GenoType MTBDRplus for the rapid detection of Mycobacterium tuberculosis and mutations causing rifampicin and INH resistance directly in smear positive pulmonary specimens and also in M. tuberculosis isolates grown from various clinical specimens. Keywords: GenoType MTBDRplus, rapid diagnosis of multidrug resistant tuberculosis (MDRTB), tuberculosis Introduction India is a high tuberculosis (TB) burdened country with increasing prevalence of multidrug resistant tuberculosis (MDR TB). Timely diagnosis and prompt treatment of infectious cases are the only key elements in reducing the spread of TB. Conventional culture and drug susceptibility testing (DST) on solid media is a time consuming process and these systems have been supplemented with automated liquid culture systems in many diagnostic laboratories with decreased time to detection and greater sensitivity. However, the time for resistance testing is still about 7 to 10 days, beginning from the time that a positive culture is obtained. [1] The most rapid results could be achieved by molecular methods including commercial or in-house DNA hybridization or amplification methods which allow detection of Mycobacterium tuberculosis as well as drug resistance in clinical samples within 1-2 days. [2],[3] Although the line probe assays were developed about 15 years ago, [4],[5] they became a popular diagnostic method recently, after WHO recommended a new policy of using line probe assays for rapid screening of patients at risk of MDR TB in 2008. The two commercially available line probe assays include INNO-LiPA Rif.TB (Innogenetics, Ghent, Belgium) targeting rpoB gene and GenoType MTBDRplus (Hain Lifescience GmbH, Nehren, Germany) targeting rpoB, katG and inhA genes in both culture isolates and clinical samples [6],[7],[8] Among the line probe assays the advantage of the MTBDRplus assay over INNO-LiPA Rif.TB is the detection of resistance to INH as well. These assays are based on multiplex PCR combined with reverse hybridization on nitrocellulose strips, targeting common mutations. GenoType MTBDRplus assay permits the molecular genetic identification of M. tuberculosis complex and its resistance to rifampicin (Rif) and INH from culture isolates and smear-positive pulmonary clinical specimens directly. The aim of the present study was to evaluate the performance of MTBDRplus assay for the rapid detection of M. tuberculosis and mutations causing Rif and high or low level INH resistance directly in smear-positive pulmonary specimens and also in M. tuberculosis isolates grown from various clinical specimens. The MTBDRplus assay is compared to drug susceptibility testing performed by proportion method using automated liquid culture system (BACT/Alert 3D, biomerieux, Durham, North Carolina, USA). Materials and Methods The study was carried out in a tertiary care centre in India during a period of one year from September 2009 to August 2010. Direct fluorescent staining All clinical specimens were subjected to direct fluorescent staining using auramine and rhodamine stains, body fluids and broncho alveolar lavage after concentration and others directly. Pulmonary specimens (smear positive) A total of 37 smear positive clinical specimens (19 sputum and 18 bronchoalveolar lavage) were directly subjected to MTBDRplus assay after digestion and decontamination by N-acetyl-L-cystine NaOH method. The sediment was re-suspended in 1-2 ml of phosphate buffer and besides MTBDRplus assay, were also subjected to culture by Bact/Alert 3D (biomerieux Durham, North Carolina, USA) and LJ media. Positive growths in either media were identified using Accuprobe molecular identification system (GenProbe, San Diego, California) and subjected to susceptibility testing. The results of MTBDRplus assay was compared with that of phenotypic susceptibility testing. Culture positive isolates A total of 69 M. tuberculosis isolates obtained by rapid automated culture using Bact/Alert 3D from various clinical specimens like pus (22), tissue (24), respiratory specimens (18) and body fluids (5) were included in the study. The species identification of M. tuberculosis was done by the Accuprobe molecular identification system and subjected to susceptibility testing. All the M. tuberculosis isolates were subjected to both MTBDRplus assay and phenotypic drug susceptibility testing and the results were compared for INH and Rif susceptibility. Drug susceptibility testing Susceptibility testing to INH and rifampicin was carried out by the Bact/Alert 3 D system (1% proportion method according to manufacturer′s instructions). This automated liquid culture system was used as the gold standard and the critical concentrations used were of 0.1 μg/ml for INH and 1 μg/ml for rifampicin. GenoType MTBDRplus assay The GenoType MTBDRplus line probe assay was carried out according to the manufacturer′s specifications. Briefly, 1 ml of liquid culture broth or a few colonies from solid media were re-suspended in 300 μl molecular biology-grade water. When done directly from smear positive pulmonary samples, 500 μl of the decontaminated sample was used. Heat killing was done at 95°C for 20 min followed by sonication for 15 min. The samples were then centrifuged at 13000g for 5 min and 5 μl of the supernatant was used for the PCR. Amplification mixture consisted of 35 μl primer nucleotide mix, 5 μl of PCR buffer with 20 mM MgCl 2 , 2 μl of 25 mM MgCl 2 , 1 U of HotStar Taq DNA polymerase from Qiagen, 3 μl of molecular biology grade water and 5 μl supernatant in a final volume of 50 μl. Amplification was done in a thermal cycler (MyCycler, Bio-Rad Laboratories) using the amplification profile: denaturation of 15 min at 95°C, followed by 10 cycles of 30 sec at 95°C and 2 min at 58°C, and 20 cycles (for culture isolates) or 30 cycles (for smear positive clinical specimens) of 25 sec at 95°C, 40 sec at 53°C and 40 sec at 70°C and the extension step of 8 min at 70°C. Hybridisation was performed using a pre-programmed TwinCubator (Hain Lifescience GmbH, Nehren, Germany). After denaturation, the biotin-labelled amplicons were hybridised to the single stranded membrane-bound probes. After a stringent washing, as streptavidin-alkaline phosphate conjugate was added to the strips, an alkaline phosphatatase mediated staining reaction was observed as bands where the amplicon and the probe had hybridised. The MTBDRplus strips were interpreted according to manufacturer's guidelines [Figure - 1]. The strip contains 27 reaction zones (6 control probes and 21 probes for mutation). The control probes include a conjugate control, amplification control, M.tuberculosis complex contol, rpoB amplification control, inhA amplification control and katG amplification control. For the detection of rifampicin resistance, the rpoB gene (coding for the β-sub-unit of the RNA polymerase) and for high level INH resistance, the katG gene (coding for the catalase peroxidase) is examined and for detection of low level INH resistance, the promoter region of the inhA gene (coding for the NADH enoyl ACP reductase) is examined [Figure - 1]. For a valid result, all the six control bands should appear correctly. The absence of at least one of the wild-type bands or the presence of bands indicating a mutation implies that the sample tested is resistant to the particular antibiotic tested. Informed consent was not required in this study since it was part of routine investigations done in the department. The study was approved by the hospital ethics committee. Results Pulmonary specimens Out of the 37 clinical specimens analysed, 34 gave a valid result for M. tuberculosis; 3 smear positive pulmonary specimens (1 BAL and 2 sputum samples) were negative for TUB band (M. tuberculosis complex control) in MTBDRplus assay, which subsequently grew non tuberculous mycobacteria (M. intracellulare from BAL and M. fortuitum and M. kansasii from the sputum samples). Out of the 34 clinical specimens with valid results, 21 were susceptible to both INH and Rif, 10 were MDR (resistant to INH and Rif), 3 were resistant to INH and 1 was only resistant to Rif. Culture positive isolates All 69 culture isolates gave a valid result in MTBDRplus assay, 46 were susceptible to both INH and Rif, 16 resistant to both INH and Rif, 6 resistant to only INH and 1 resistant to only Rif. Out of the 69 culture positives, 39 were smear positive and 28 were smear negative by direct fluorescent staining. Two specimens were not subjected to staining because the specimen quantity was insufficient. All genotypically resistant isolates with respective mutations are shown in [Table - 1]. Drug susceptibility testing A total of 101 M. tuberculosis isolates, 69 from culture and 32 from smear-positive respiratory specimens were analysed by genotypic and phenotypic assays for Rif and INH resistance and the results were compared [Table - 2]. Two clinical specimens, one BAL and one sputum, were excluded from the comparative analysis due to failure of growth. The sensitivity and specificity for detection of resistance to rifampicin was 100% and 97.3%, and to INH was 91.9% and 98.4%, respectively. Out of the total 101 strains tested by both the methods, there was 98% concordance for Rif and 96% concordance for INH sensitivity testing between MTBDRplus assay and phenotypic DST. The discrepant results are shown in [Table - 3]. In our experience, the performance of the assay was not satisfactory in smear negative culture positive pulmonary specimens and both smear positive and negative extra-pulmonary specimens (data not given). Discussion The present study has evaluated the performance of MTBDRplus molecular assay for rapid detection of multi-drug resistant M. tuberculosis directly from smear positive pulmonary samples and culture isolates. The assay which is very user friendly and easy to perform is proven to be successful in rapid detection MDR TB. Many recent studies have already demonstrated the feasibility of MTBDRplus assay as an effective tool in early detection of MDR TB and have good concordance with phenotypic drug susceptibility results. [3],[9],[10],[11] The present study has evaluated the assay in a geographic region, which is endemic for M. tuberculosis and studied the frequent mutations leading to drug resistance. To the best of our knowledge this study is the first of its kind from India. In our study, the MTBDRplus assay showed a high sensitivity and specificity (100% and 97.3%, respectively) for detection of Rif resistance compared to the conventional DST. However, for detection of INH resistance, in comparison to the conventional DST, the sensitivity and specificity of the MTBDRplus assay was 91.9% and 98.4%, respectively. The results are in concordance with other recent studies, which have reported the sensitivity of MTBDRplus assay in detecting Rif resistance varying between 92% to 99% and INH resistance between 73% to 92%. [3],[11],[12] Concerning Rif resistance, a mutation in the rpoB gene was detected in 26 out of 27 phenotypically resistant strains. A 100% sensitivity in detecting Rif resistance in our study suggests that all the mutations were in the 81-bp region of the rpoB gene. This is in agreement with many other studies which have also proven the mutations in 81-bp region alone have got 98-100% sensitivity in detecting Rif resistance. [10],[13],[14],[15] Among all the gene mutations leading to Rif resistance, codon 531 of the rpoB gene was the most frequently encountered (84.6%). Other mutations detected were at codons 526 (2 isolates-7.7%) and 516 (2 isolates-7.7%) [Table - 1]. Three isolates had only a deletion of wild type 8 without any detectable mutations. One out of these 3 was also confirmed to be resistant to Rif phenotypically, whereas 2 (ID 876/09 and 1035/09) were sensitive by the conventional DST. However, such discrepancy may be encountered in this assay and in such cases phenotypic results are considered confirmatory. If deletion of wild type 8 is the only indication of Rif resistance and there is no mutation probe, it would be advisable to continue the patient on Rif therapy till phenotypic sensitivity report is available. The molecular basis of resistance to INH is more complex and involves mutations in more than one gene or gene complex such as the katG, inhA and kasA genes and the intergenic region of the oxyR-ahpC complex. [16],[17] In our study, a mutation in the katG codon 315 was detected in 32 isolates (86.5%) and in inhA 15 region in 2 isolates (5.4%) out of the 37 phenotypically INH resistant strains [Table - 1]. No mutations could be detected in 3 out of 37 isolates (8.1%) that were phenotypically resistant to INH. It is suggestive that these strains carry a mutation in some other genomic region not incorporated in this assay such as ahpC, kasA or ndh. [18],[19],[20] There was one false positive result with INH resistance which was in association with inhA C15T mutation but was sensitive to INH by conventional DST [Table - 3]. This could be a mutation which was not phenotypically expressed. The GenoType MTBDRplus assay which is a revised modification of the original GenoType MTBDR version (Hain Lifescience GmbH, Nehren, Germany) with incorporation of probes to detect mutations within the inhA gene as well has a better sensitivity for detecting INH resistance. In some earlier studies the main limitation of the original MTBDR assay appears to be the low sensitivity for the detection of INH resistance. [9],[21] This was because the test was targeting only the katG S315T mutation previously. But the MTBDRplus assay with a second target included namely, the regulatory region of the inhA gene, this issue appears to have been resolved. The higher value of sensitivity for detection of INH resistance in our study may be due to the fact that the majority of the mutations were located on the katG codon 315 in contrast to the study by Lacoma et al[11] and Miotto et al[12] who had reported a low sensitivity of INH resistance 73% and 79%, respectively. However, Hillemann et al.[3] has reported a high sensitivity (92%) of INH resistance similar to our study. There were three clinical specimens (1 BAL and 2 sputum) that were smear positive but negative for MTB by MTBDRplus assay and subsequently grew NTM in culture. In all these cases the significance of this information could be valuable to the treating clinician. The possibility of NTM, because the MTBDRplus assay did not develop a band for MTB could alter the treatment options. In case of the patient with M. fortuitum in sputum, the organism was also isolated from a pus aspirate from a nodule. The other 2 cases were new cases, but their presence was confirmed by doing a repeat NALC-NaOH decontamination and culture of the specimen, which also grew the same organism. A major limitation of the molecular genetic detection of drug resistance remains that not all mutations conferring resistance to anti-TB drugs are known. This is especially true in detecting INH resistance and explains the comparatively low sensitivity. Similarly the sensitivity obtained phenotypically in drug-resistant tubercle bacilli due to its slow growth can be interpreted as sensitive also need to be kept in mind. However, the performance characteristics of the assay suggest that the assay is at par with conventional drug susceptibility testing methods with distinct advantages. Good concordance was observed between BacT/ALERT 3D drug susceptibility testing and MTBDRplus assay. When frequent contamination of the respiratory specimens in culture and the subsequent increase in turn around time is considered, molecular assay is superior to the conventional DST methods. Even though the assay is not recommended for smear negative pulmonary samples or any extra-pulmonary samples, we tried to assess the performance of the assay with a limited number of such samples which were culture positive. But our experience with smear negative culture positive samples was contradictory to some other studies that claim high proportion of interpretable results. [10] In our experience the assay may be beneficial in smear positive pulmonary samples and culture isolates from any specimen to obtain an early detection of MDR tuberculosis, which in turn can help in early modification of anti-tubercular therapy and containment of its spread. In conclusion, the study, the first of its kind from India, a geographic region with high prevalence of tuberculosis, has shown MTBDRplus assay has good sensitivity and specificity in detecting MDR TB cases in our settings. With a turn around time of less than 48 hours, and simultaneous detection of Rif and INH resistance directly from smear positive pulmonary samples, this technique saves several weeks of time required for culture and DST. In the background of rising drug resistance in M. tubercusis, the MTBDRplus assay may be a good tool in the diagnosis and management of MDR TB. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12011f1.jpg] [mb12011t3.jpg] [mb12011t2.jpg] [mb12011t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}