 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 64-68 Original Article Evaluation of the microscopic observational drug susceptibility assay for rapid and efficient diagnosis of multi-drug resistant tuberculosis RP Lazarus1, S Kalaiselvan1, KR John2, JS Michael1 1 Department of Microbiology, Christian Medical College, Vellore, 632004, Tamil Nadu, India Correspondence Address: Date of Acceptance: 07-Oct-2011 Code Number: mb12012 PMID: 22361763 DOI: 10.4103/0255-0857.93039 Abstract Purpose: Tuberculosis (TB) is endemic in India and the burden of multi-drug-resistant tuberculosis (MDR-TB) is high. Early detection of MDR-TB is of primary importance in controlling the spread of TB. The microscopic observational drug susceptibility (MODS) assay has been described as a cost-effective and rapid method by which mycobacterial culture and the drug susceptibility test (DST) can be done at the same time. Keywords: M. tuberculosis, MDR-TB, microscopic observational drug susceptibility assay, tuberculosis Introduction There is resurgence in the number of new tuberculosis (TB) cases every year. The arrival of resistant TB, both the multi-drug-resistant (MDR-TB) and the extensively drug-resistant TB (XDR-TB), has further worsened the condition. [1] Therefore, there is a need for early diagnosis and treatment. WHO has endorsed commercial rapid culture methods [2] and molecular line probe assays [3] for simultaneous detection of both Mycobacterium tuberculosis and resistance to rifampicin (RIF) and isoniazid (INH). The former requires expensive equipments, high running cost, whereas the latter is expensive and requires molecular expertise which is often not available in resource poor settings. The microscopic observation drug susceptibility assay (MODS) developed in Peru is a liquid-culture based test that detects M. tuberculosis and assesses INH and RIF susceptibility directly from sputum samples. [4] This assay has been used and found to be cost-effective, technically simple and useful in resource poor settings. [5] The MODS assay has been evaluated in our setting for the diagnosis of pulmonary TB, but its performance in the diagnosis of drug resistance has not been studied. [6] Therefore, the study objectives were to (i) evaluate the performance of the MODS assay against the conventional gold standard of culture on Lowenstein Jensen (LJ) media; (ii) to perform the susceptibility of M. tuberculosis to INH and RIF using MODS directly on positive sputum specimens and compare the results with the standard drug susceptibility test (DST) (1% proportion method) on LJ media; (iii) compare the time taken for positive result by the MODS assay, culture on LJ and DST by the 1% proportion method and to (iv) evaluate the cost-effectiveness of the MODS assay. Materials and Methods Enrolment and sample size This was a prospective, double-blinded study done over a period of 12 months at a routine diagnostic Mycobacteriology Laboratory (accredited by RNTCP and CTB division, Ministry of Health, Government of India, New Delhi) at Christian Medical College, Vellore, Tamil Nadu. The study included consecutive sputum samples, received at the Mycobacteriology Laboratory for routine mycobacterial culture, and DST from patient's aged ≥ 18 yrs and symptomatic for pulmonary TB.
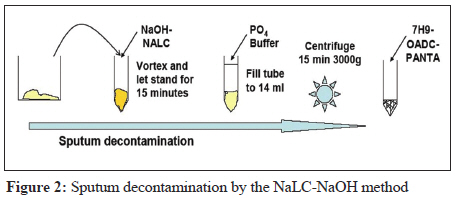
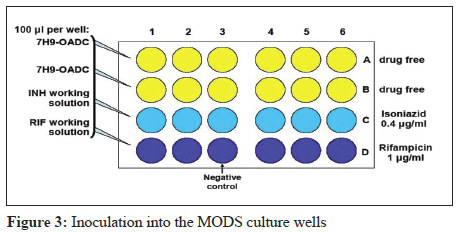
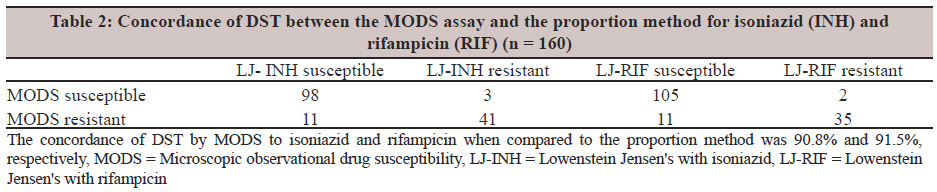
(N = sample size, p = prevalence of the case, q = 100 - p, d = difference in the prevalence). The prevalence of MDRTB is assumed to be 25-35% from the available data in our institution. Based on this formula, the sample size was determined to be 300 (confidence level: 95%). Ethics The Study was approved by Institutional Review Board and Ethics committee. Individual informed consent was not obtained as the study was conducted only on samples that were received in the laboratory for routine diagnosis and it did not involve any additional samples, intervention or any change in management of the patient. Sample processing The sputum samples underwent direct Auramine O fluorescence smear microscopy, following which the sample was divided in to two aliquots, one for culture on LJ medium and the other for the MODS assay as shown in [Figure - 1]. The old Petroffs method of digestion decontamination was used for culture on LJ and the NaLC-NaOH method of digestion decontamination was done for culture on MODS assay. The second sample was coded and the research staff performing the MODS assay was not aware of the results of the conventional methods. MODS assay The MODS assay was performed as described in the standard operating procedure (SOP) given in the MODS website www.modsperu.org (MODS user guide v12.1 14082008). [7] The diagrammatic representation of the procedure is shown in the [Figure - 2] and [Figure - 3]. Specimens were decontaminated and inoculated in 24 well tissue culture plates inside a Biosafety cabinet II B2 in a Biosafety Level 21/2 laboratory with negative pressure. Antibiotics for the MODS assay and for conventional DST were purchased from Sigma Aldrich, USA. Fresh antibiotic stock solutions were made every month as per protocols described in the SOP. 1 ml of the sample suspension was stored in micro-centrifuge tubes at 2-8°C as backup; the remaining 1 ml was used for plating in a sterile 24-well tissue culture plate. The plates were sealed in zip lock polythene bags to prevent accidental spills, minimise cross-contamination, occupational exposure and aerosolisation of the cultures, and were incubated at 37°C. The culture plates were examined 5th to 15th day using an inverted light microscope at a magnification of 40×. Plate reading was then taken on day 18 th and on day 21. If the results were still negative on day 21, the final result was considered as negative. Positive cultures were identified by characteristic cord formation by M. tuberculosis in drug-free control wells, as described previously. Whenever there was growth in the drug free control well, then drug-containing wells -INH and RIF- were visualised on the same day; growth in the presence of drug was regarded as resistance of the organism to the drug, whereas no growth was considered as susceptible. Contaminated samples were re-plated using the back-up samples stored at -20 0 C. Culture and DST on LJ medium Mycobacterial isolates obtained on in-house prepared LJ media were subjected to DST by the 1% proportion method according to Standard Operating Procedures based on Kent and Kubica et al. [8] This was taken as the reference gold standard against which the performance of the MODS assay was evaluated. The drugs used were from Sigma Aldrich, USA(marketed in India by Sigma Aldrich in Bangalore -Plot # 12, Bommasandra Jigani Link Road Bangalore - 560 100) Quality control The reference strain H37Ra ATCC 25177 was used as a positive control in every batch of the MODS assay and the conventional DST. Results Three hundred and two consecutive sputum samples which were received in the mycobacteriology laboratory for mycobacterial culture and first-line DST were included in the study. Of the 302 sputum samples collected, 160 samples were culture positive for M. tuberculosis by both MODS assay and LJ medium and 118 were culture negative by both the methods. In addition 14 samples were culture positive for M. tuberculosis by MODS alone, while 10 were culture positive by LJ and negative by the MODS assay [Table - 1]. On comparison with the reference LJ culture in this study, the MODS assay showed a sensitivity of 94.12% (95% [CI] 91.46%- 96.77%) and a specificity of 89.39% (95% [CI] 85.92%- 92.87%) with a positive predictive value of 91.95% (95% [CI] 88.89%- 95.02%) and a negative predictive value of 92.19% (95% [CI] 89.16%- 95.21%). As shown in [Table - 2], DST was done on 160 M. tuberculosis isolates. Out of these, 98 and 105 isolates were susceptible respectively to INH and RIF and 41 and 35 isolates were resistant by both the 1% proportion method and the MODS assay. The concordance of DST by MODS to INH and RIF when compared to the proportion method was 90.8% and 91.5%, respectively. In addition, 11 isolates each for INH and RIF were resistant by the MODS assay but susceptible by the 1% proportion method and 3 isolates were susceptible for INH and two for RIF, respectively by the MODS assay but resistant by 1% proportion. Due to contamination in either of the 2 culture systems, seven isolates were excluded from the final statistical calculation. The mean time to positivity by MODS for both culture and DST was 9 days as compared to culture positive by LJ being 21 days and DST by the 1% proportion method a median of 42 days. The cost for performing the MODS assay was Rs. 250/- for both culture and DST results for INH and RIF, compared to Rs. 950/- culture of LJ and 1st line DST. The contamination rate of MODS was 7% and that of LJ culture 5%. The sputum samples received were processed by both MODS and Culture by LJ on the same day. The samples that were contaminated during the first run of MODS were inoculated and tested again from samples that were stored at -20 o C as back up. Discussion Patients infected with MDR-TB strains pose a major threat to the community. The unavailability of early DST results for drug-resistant strains, and the arrival of unaffordable new diagnostic tests have lead to the restriction of TB DST to high risk groups in resource poor settings, thereby causing the catastrophic spread of MDR-TB in the community. The early detection of drug-resistant strains would lead to the reduction in the morbidity and mortality of infected patients; this would also play an important role in controlling the spread of MDR-TB. [1] DST methods with solid media are inexpensive but slow and laborious. Liquid-automated commercial systems are rapid but require heavy, expensive equipment, have high running costs and are technically complex. [2] In such a situation, the MODS assay described by Moore et al[4] is a simple and rapid method described to detect both the presence of the M. tuberculosis and susceptibility of the organism to INH and RIF. MODS depends upon three key principles namely that M. tuberculosis grows faster in liquid (broth) than on solid media. Secondly, that characteristic M. tuberculosis growth can be observed under an inverted light microscope long before the colonies are visualised on solid agar. Thirdly, DST from clinical samples is possible by adding anti-TB drugs into broth cultures at the very beginning. When compared to conventional gold standard of mycobacterial culture on LJ medium, the MODS assay had good sensitivity of 94.12% and a modest specificity of 89.39%. It was lower when compared to the 100% sensitivity and specificity described by Limaye K et al. [9] They evaluated MODS on acid fast smear positive sputum samples, whereas we tested them on consecutive sputum samples received in the laboratory from patients suspected to have pulmonary TB. More recently, this assay has been tested on a patient population with higher rates HIV positivity, [10] they had lower sensitivity than ours but higher specificity. Being a liquid culture system MODS assay had better culture positivity than LJ medium. Additional 14 samples were culture positive by the MODS assay, of which 10 were from patients with clinical and or radiological diagnosis of TB and who responded to anti-TB treatment. On the other hand, LJ culture picked up 10 additional culture positives that were negative by the MODS assay. Seven out of 10 samples were lost to contamination during MODS culture. Delays in diagnosis of TB especially MDR-TB is one of the important reasons for poor outcome, increased mortality and continued transmission. [11] As a diagnostic test for both M. tuberculosis and MDR-TB, the MODS assay was remarkably faster than conventional tests for culture and DST. Mean time to positivity for culture and DST by MODS was 9 days as compared to a mean of 21 days for culture on LJ media and an additional 42 days for DST by the proportion method. In the clinical setting, this would allow for early diagnosis and treatment of both HIV positive and negative patients with TB particularly those with multi-drug-resistant TB. [11] In our study, we found that the MODS assay being a 7H9 liquid culture medium had slightly higher contamination rate of 7% as compared to 5% contamination seen on LJ medium. The running cost of MODS was Rs. 250/- which is drastically less than Rs. 950/- the cost of conventional culture and DST on LJ medium. However, though the running cost is relatively low, the initial setting up cost would be high due to the high cost of an inverted microscope and biosafety cabinet needed to perform the test. The MODS assay is a relatively simple culture method that can be adopted by any laboratory. The methodology is available freely on the MODS Peru website-(www.modsperu.org). [7] The materials needed to set up the assay are widely available from local laboratory suppliers. Compared to automated culture methods and molecular techniques, the MODS assay is less complex and does not require trained personnel to perform the test. Training of laboratory personnel can be done within a week and pattern recognition of cording can be supplemented by photo library of images from the above mentioned website. [7] Liquid culture systems in diagnostic mycobacteriology are fraught with risk of aerosolisation when compared to conventional solid culture methods. Therefore, strict infection control measures need to be taken while processing the samples, right from inoculation to the reading of the plates. [12] We processed the samples and inoculated the plates in a Biosafety cabinet II B2 and sealed centrifuge. The plates were also sealed and kept in a zip lock bag. The laboratory personnel wore N95 mask while processing the sample and all this work was conducted in an accredited BSL II Mycobacteriology laboratory with negative pressure. In an era of increasing drug-resistant TB, the MODS assay is a diagnostic tool which is simple, rapid, cost effective and efficient technique for diagnosis of TB and in particular MDR-TB in high burden, underdeveloped and developing countries. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12012t2.jpg] [mb12012f2.jpg] [mb12012f1.jpg] [mb12012t1.jpg] [mb12012f3.jpg] |
| |||||||||
 The sample size was calculated using the formula.
The sample size was calculated using the formula. 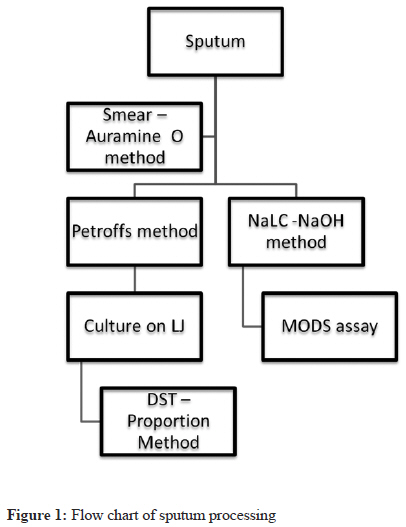{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}