 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
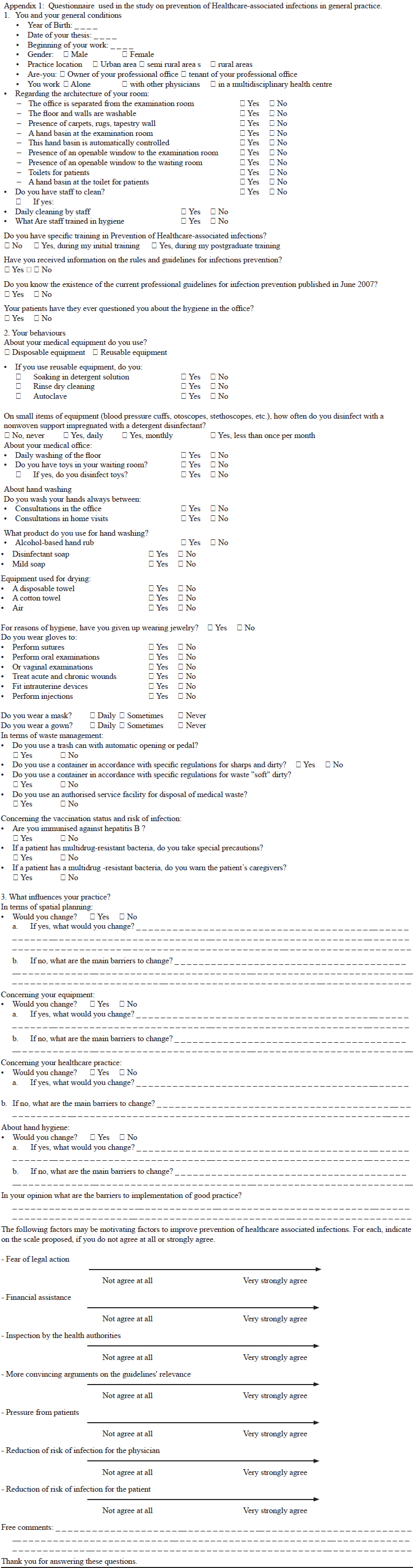
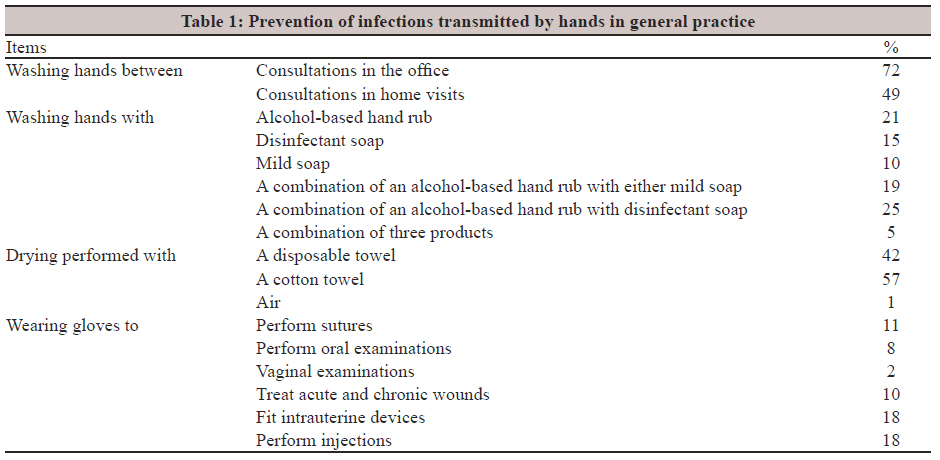
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 69-75 Original Article Prevention of healthcare-associated infections in general practice: Current practice and drivers for change in a French study M Gignon1, S Farcy2, JL Schmit3, O Ganry1 1 Medical School, University of Picardy, 3 rue des Louvels, F-80000; Public Health Department, Amiens University Hospital, Amiens, France Correspondence Address: Date of Acceptance: 07-Oct-2011 Code Number: mb12013 PMID: 22361764 DOI: 10.4103/0255-0857.93040 Abstract Purpose: The fight against Healthcare-associated infections is a public health priority and a major challenge for the safety and quality of care. The objective was to assess hygiene in general practitioners' (GPs') office and identify barriers to and drivers for better practice. Keywords: Compliance with guidelines, general practice, healthcare-associated infections, public health, quality improvements Introduction Healthcare-associated infections (HAIs) affect hundreds of millions of people each year and have an impact on both health of patients and on cost of healthcare systems. Indeed, HAI constitutes the most common adverse event threatening patient-safety worldwide. [1],[2] In Europe, the prevalence of HAIs is between 4.4% and 14.8%. [3],[4] In the USA, the incidence is estimated at around 5-6%, with an attributable mortality of 3.6% and excess costs of at least 4.5 billion US dollars every year. In the United Kingdom, a study has estimated excess costs of 930 million pounds sterling with 3.64 million additional hospital days. [5] For example, if we apply an average additional cost of 3,500 to 8,000 Euros (€, EUR) for each of the 750,000 nosocomial infection per year in France, we arrive at a figure of between 2.4 and 6 billion EUR. Hence, a 10% decrease in infections will lead to a saving of 240 to 600 million € - at least six times more than the amount that France currently spend on prevention. This calculation emphasises the fact that poor-quality care costs more than prevention. [6] The fight against HAIs is a public health priority that was promoted through the World Health Organization's 'Clean Care is Safer Care' campaign. [7] Improved surveillance and control of HAIs are major challenges for the safety and quality of care. [8] HAIs have many causes, which are related to healthcare systems and procedures on one hand and behavioural practices on the other. Even though the medical literature has often reported on infection-control practices in hospital care, a focus on outpatient care is less common. [9],[10],[11],[12],[13] Hygiene rules concern the GP's office just as much as they do in hospital care. In 2007, the French Agency for the Quality of Care issued professional guidelines on hygiene and infectious risk prevention in surgeries and paramedical settings, on the basis of a review of the international scientific literature. [14] The primary objective of the present work was to assess hygiene practices in general practice. The secondary objective was to identify obstacles limiting the dissemination of good practice and factors that may motivate GPs to improve their hygiene during health-care delivery. Materials and Methods We performed a cross-sectional study of 800 randomly selected GPs in the Picardy region of northern France. On the basis of the current professional guidelines, we developed a self-administered questionnaire consisting of two parts (Appendix 1). The first part assessed the GPs' compliance with laid-down guidelines on hygiene, including the office's lay-out and cleaning, training in hygiene, sterilisation equipments, use of gloves and vaccination against hepatitis B. It was composed of closed questions with yes/no or multiple choice answers. The second part of the questionnaire focused on (i) obstacles to implementation of good practice and (ii) factors that may encourage physicians to improve practice. It was composed of open questions with answers that are free and Lickert items. [15] The physicians' motivations were expressed on a numerical scale ranging from 1 (not at all motivated) to 7 (extremely motivated). The questionnaire was posted to a representative sample of 800 randomly selected GPs in the Picardy region of northern France. A reminder was sent to physicians who did not return the questionnaire within a few weeks. We performed a descriptive statistical analysis of the responses to closed questions and a qualitative analysis of the responses to open-ended questions. In this analysis, quantitative variables are expressed as the mean and 95% confidence interval, whereas qualitative variables are expressed as a percentage. Comparisons were made using a chi-squared or Student's t test. The threshold for statistical significance was set to P<0.05. Results Description of the study population The response rate was 22% (n = 173). All returned questionnaires were analysed. The population studied was predominantly male (75% male, n = 129). The mean age was 51 years. Fifteen percent of the GPs had set up their general practice in the previous 10 years, 25% had set up their practice between 10 and 20 years previously and 60% had been practising for over 20 years. Thirty-nine percent worked in urban areas, with 29% in semi-rural areas and 32% in rural areas. Forty-six percent worked alone, 46% worked with other physicians in a GP-only practice and 8% worked in large, multidisciplinary health centres. Assessment of practice The office was compliant with architectural guidelines (alcohol-based hand rub, washable flooring, no carpet, a hand basin in the care room, at least one window each in the waiting room and care room and a toilet with a hand basin for patients) in 42% of cases. A person was responsible for cleaning in 95% of the surgeries. Daily cleaning took place in two thirds of the surgeries and the floor was washed daily in 68% of cases. The personnel responsible for cleaning the premises had received specific training in 57% of cases. In our sample, 41% of physicians had received training in hygiene (during their initial training among 15% of GPs and as postgraduate training among 24% of GPs). The extent of training varied significantly with the GPs′ time in general practice. Fifty-six percent of the GPs having been in practice for less than 10 years had received training, versus 38% (P <0.05) of the GPs having been in practice for 10 or more years. Only a third of doctors said they were aware of the current professional guidelines. Forty-two percent of the physicians had already been questioned by their patients about hygiene in the office. Thirty-one percent of the surveyed GPs used disposable equipment. Only 38% of the remainder complied with guidelines on the sterilisation or disinfection of reusable equipment. Small items of equipment (blood pressure cuffs, otoscopes, stethoscopes, etc.) were variously maintained daily (by 21% of the GPs), monthly (38%), less frequently than monthly (25%) or not at all (16%). Of the 148 surgeries that made children's toys available in the waiting room, 42% never disinfected these items. The results for measures to prevent hand-transmitted infections are summarised in [Table - 1]. For hygiene reasons, 21% of physicians had stopped wearing jewellery or watches. Most physicians (60%) never wear a mask, whatever the circumstances. Daily use of gowns was found in 7% of the physicians, who wore it promptly as and when required and 8% of the physicians never wore gowns. In terms of waste management, 36% of physicians complied with the guidelines; 97% of these GPs used an accredited service. Twelve percent of physicians (all of whom were over the age of 45) were not vaccinated against hepatitis B. When dealing with patients with multidrug-resistant bacteria, 79% of the GPs took stricter hygiene measures and 71% warned the patients' caregivers. Barriers to and drivers for better practice In terms of spatial planning, 60% of the physicians did not want to induct any change in practice for improvement. Others planned to change their premises (4%) or flooring (3%) or install automatic taps (3%). The main barriers to change were the high cost of modifications, lack of time and/or lack of appropriate space. Sixty-nine percent of the GPs did not to wish to change their equipment, 9% planned to opt for single-use, disposable material and 5% planned to clean their equipment more often. Twelve percent of the physicians considered that disposable materials were too expensive (12%), while others believed that they would not have a sufficiently frequent need for materials with a defined shelf life (7%). Sixty-one percent of the physicians did not intend to change their health-care practice, while others planned to improve their use of gloves/masks (12%) or gowns (3%). Nearly two thirds of the GPs did not want to change their practice regarding hand hygiene. However, 8% of the physician proposed to conduct a more regular hand hygiene practice and 6% planned to opt for a disposable towel. Most doctors highlighted a lack of information and felt they do not have enough knowledge to choose relevant products (36%). Others stated that the frequent changes in the guidelines prevent them from staying up to date (21%). Some physicians expressed doubts on the efficacy of the measures stated in the guidelines (16%) and the risk of infection itself (11%). Others suggested that the measures were inadequate and/or not valid for non-hospitalised patients. The cost of the fight against infection is a barrier for the GP. Results are expressed as mean (+ / - standard deviation). An average that tends to 7 is a very motivating factor and a average tending to 1 is a low motivation factor. The stated drivers for change were as follows (in decreasing order on the scale, from 1 to 7): Pressure from patients (4.8; (4.4, 5.1)), inspection by the health authorities (4.8; (4.4, 5.1)); fear of legal action (4.4; (4, 4.7); financial assistance (4.2; (3.8, 4.6)); more convincing arguments on the guidelines′ relevance (3.5; (3.2, 3.9)). The least motivating factors were a reduction of risk of infection for the physician (3.4; (3, 3.7)) and the patient (3.1; (2.7, 3.5)). Discussion Our results show that there are significant differences between actual practice and professional guidelines concerning treatment hygiene in the GP′s office. Poor adherence to medical guidelines has often been described, regardless of the medical specialty or country. [16],[17] Even though architectural features are not easily changeable, some basic practices can always be improved. Waiting room toys increase the risk of transmission of infectious diseases. [18],[19],[20] and therefore should be suitable for easy disinfection. We believe that physicians should receive more information on the preferred characteristics of waiting room toys. Although wiping hands with cloth towels is common, several studies have evidenced a significant risk of contamination. [21] Use of an alcohol-based hand rub (an easy-to-use product with demonstrated efficacy) is still too infrequent - especially when performing home visits. [22],[23] The frequency of use of appropriate medical gloves could also be emphasised upon and its use increased in general practice. Knowledge about patients who have hospital acquired infections with multidrug-resistant bacteria after discharge is particularly important. Specific measures of prevention should be taken such as wearing gloves (non-sterile single-use) when there is direct contact with the site carrying the multidrug-resistant bacteria and wearing disposable and single-use gowns when there is a risk of projections. Despite the significant potential for improvement in several areas, our study shows that about two thirds of GPs do not plan to change their current practice. This illustrates the gap between evidence-based guidelines and actual clinical practice. In the literature, various factors have been identified as hampering adherence to guidelines. [17],[24] The first is lack of awareness by the practitioner. Even though guidelines are disseminated widely, limited uptake may be due to the high volume of information available to GPs and, perhaps, the limited reading time available. The physician′s acceptance of guidelines depends on the credibility and applicability of the proposed measures and the corresponding costs involved. [25] These barriers appear to be particularly frequent among GPs. [26] Strategies to improve practices must take into account barriers in initiating changes. The assessment of professional practice and targeted, tailored measures for reducing barriers to guideline implementation can be effective but are cumbersome to implement. [27] References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12013t1.jpg] [mb12013a1.jpg] |
| |||||||||
{kind=link}
{kind=link}