 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
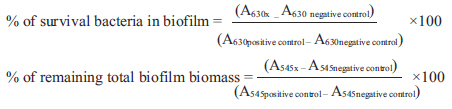
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 76-80 Original Article Antimicrobial activities against biofilm formed by Proteus mirabilis isolates from wound and urinary tract infections R Wasfi1, OA Abd El-Rahman2, LE Mansour3, AS Hanora4, AM Hashem3, MS Ashour2 1 Department of Microbiology, Faculty of Pharmacy, University for Modern Sciences and Arts, Giza, Egypt Correspondence Address: Date of Acceptance: 31-Oct-2011 Code Number: mb12014 PMID: 22361765 DOI: 10.4103/0255-0857.93044 Abstract Background: Bacterial species are capable of living as biofilm and/or planktonic forms. There is increasing evidence for the role of bacterial biofilm in various wound and urinary tract infections (UTIs). The aim of the present study was to evaluate the ability of the bacteria, isolated from urinary tract infections (UTIs) and wound infections, to form biofilm and correlate the role of biofilm with their antimicrobial resistance. Keywords: Antimicrobial agents, biofilm, Proteus mirabilis, wound and urinary tract infections Introduction Bacteria generally exist in one of the two types of population: Planktonic, living freely as single cells in bulk solution, and sessile, as a unit attached to a surface or within the confines of a biofilm. The differences in the physiological state of biofilm and planktonic cells are reflected by significant changes in their gene expression pattern, as highlighted by studies on functional genomics . [1] The pathogenic bacteria which are able to form biofilm are the cause of many chronic and recurrent infections such as periodontitis, endocarditis, chronic otitis media, cystic fibrosis, urinary tract and wound infections. [1] Moreover, the medical devices such as intravenous catheters, artificial joints and cardiac pacemakers, which become rapidly coated with human extracellular matrix and serum proteins, are prime targets for bacterial biofilm formation. [1] Biofilm-forming bacterium constitutes a major medical problem because of the sharply decreased susceptibility of bacteria, within the biofilm, to host defences and antibiotic treatments. [2] Standard antibiotic therapy is only able to eliminate the planktonic and the superficial cells in biofilm leaving the deeply embedded sessile cells propagating within the biofilm and continue to disseminate when the therapy is terminated. [2] The aim of this study was to quantitatively evaluate biofilm formation among bacterial species isolated from urinary tract and wound infections from two Egyptian hospitals. In addition, the susceptibilities of four Proteus mirabilis isolates to antimicrobials were assessed by examining the effect of different antimicrobials on planktonic bacteria, biofilm synthesis and preformed biofilm. P. mirabilis isolates were selected because of their strong biofilm forming ability, the implication of Proteus sp. biofilm on both urinary tract and wound infections and there are few studies on the effect of antimicrobial agents on biofilm formed by P. mirabilis. Materials and Methods Bacterial strains A total of 207 isolates were obtained from 204 specimens (urinary tract and wound infections sources) from patients admitted to General Surgery Department and Urology department in El-Hussein and El-Demrdash hospitals, Cairo, Egypt. The isolates were then identified microscopically and biochemically according to Mahon et al. [3] The present study was approved by the Research Ethics Committee of the University and written consent was also taken from the patients. Quantitative biofilm assay All the isolated bacteria were screened for their ability to form biofilm using the microtitre plate method described by O'Toole et al. [4] The extent of biofilm formation was determined by the following formula; BF = AB - CW (1) Where BF is the biofilm formation, AB is the OD 545nm of stained attached bacteria and CW is the OD 545nm of stained control wells containing bacteria-free medium only. [4] Results were interpreted as follows: BF >0.3 strong biofilm formation, BF <0.3 and >0.2 moderate biofilm formation, BF <0.2 and >0.1 weak biofilm formation and BF <0.1 negative biofilm formation. Antimicrobial susceptibility The antimicrobial agents amoxicillin, ciprofloxacin, trimethoprime-sulfamethoxazole, erythromycin, gentamicin nitrofurantoin, ceftriaxone, chloramphenicol were evaluated against four Proteus sp. isolates (two isolates from urinary tract and other two isolates from wound infections). Determination of MIC of antimicrobials on planktonic cultures The susceptibility testing was performed on planktonic cultures using the two-fold micro-broth dilution method using flat bottomed 96-well microplates.[5] Effect of sub-MICs of antimicrobials on bacterial adherence The effect of sub-MICs (1/2, 1/4 and 1/8 MIC value for each tested isolate) of antimicrobials was evaluated on biofilm synthesis (bacterial adherence). This test was done by adding various concentrations of antimicrobials after distribution of bacterial inocula in micro-plate wells so that final concentration of bacteria was 5 Χ 10 5 cell/ml. The plates were incubated for 24 h at 37 o C. Biofilm formation was determined by the crystal violet assay. [6]
Where A c is OD 545 nm for control wells and A t is OD 545nm for biofilm in presence of antibiotics The effect of antimicrobials on pre-formed biofilms The antimicrobial effect on pre-formed biofilm was determined by examining its effect on viable bacteria within the biofilm matrix and on total biofilm biomass. Bacterial biofilms were allowed to be formed in micro-titre plates, then two-fold dilutions of antimicrobials (from 8 to 1024 μg/ml) were then added to the wells.[3] Plates, which are used for testing the effect of antimicrobial on total surviving viable bacteria, were rinsed and 100 μl sterile medium was added in each well, then the plate was sonicated at room temperature for 10 min in a water-bath sonicator (Soniclean; , Australia) for transferring biofilm from wall of wells to the medium. The surviving bacteria was detected by measuring change in turbidity by measuring OD 630 using an ELISA plate reader before and after incubation at 37°C overnight. [3],[7] Plates, used for measuring remaining biomass, were assayed by the crystal violet assay as mentioned before under the quantitative biofilm assay. The percentage of biofilm remaining in the presence of antimicrobial agents was calculated using the following two formulas:
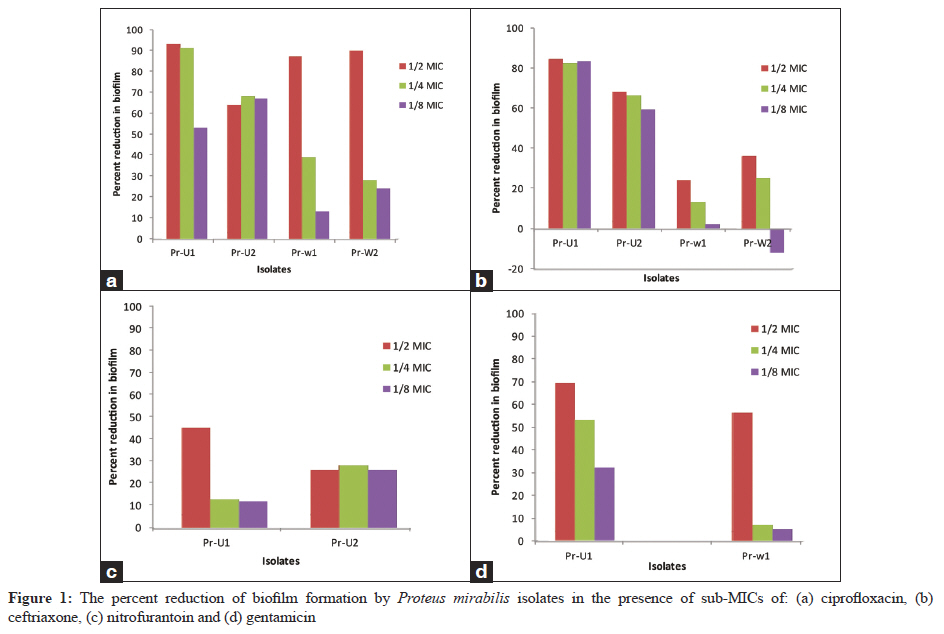
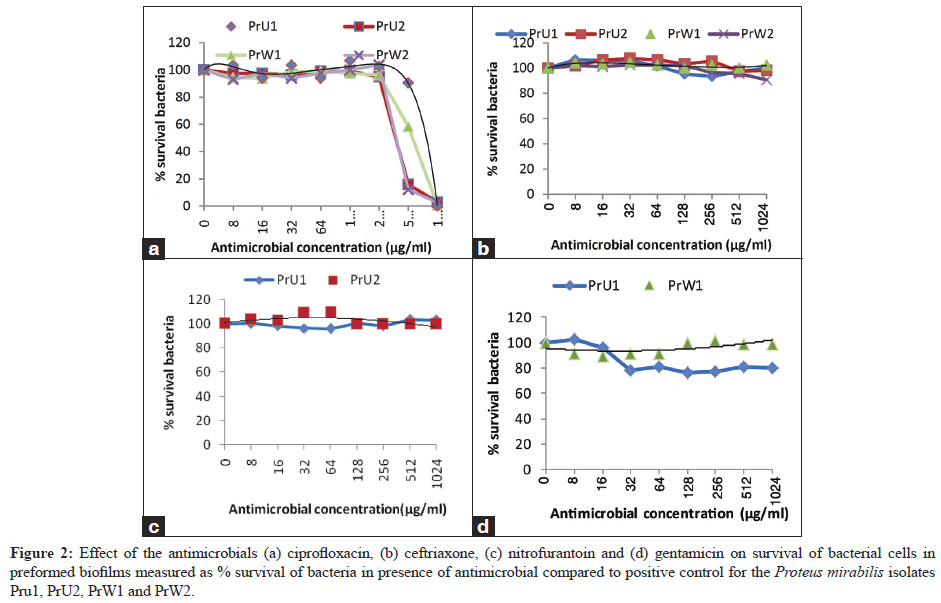
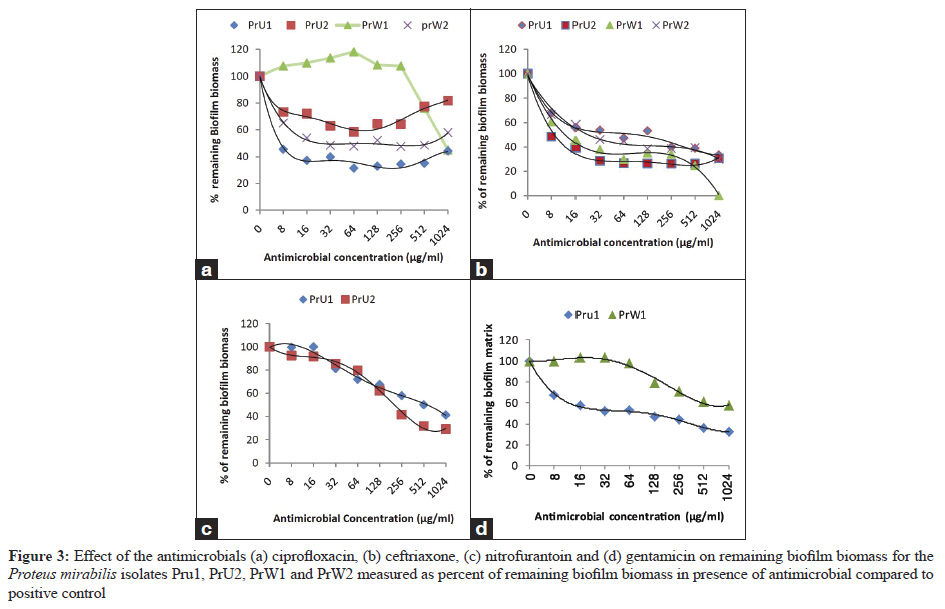
The letter x corresponds to the tested antimicrobial agent. The OD (nm) value obtained for each strain without drug was used as positive control; wells containing Mueller Hinton broth only were used as a negative control. Results Isolation and identification of causative agents from urinary tract and wound infections A total of 102 and 105 bacterial isolates were obtained from urine samples and specimens of wound infections, respectively. The most predominant bacteria isolated from urine samples was Escherichia coli (50%), while the highest percentage in wound infection was obtained by Pseudomonas aeruginosa (22%). Proteus sp. represented 8% of the total collected Gram negative isolates. Determination of biofilm forming potentials of different bacterial isolates Our results showed variation among the capacities of diverse isolates from different sources to form biofilms in-vitro. The strongest biofilm forming isolates belonged to the Klebsiella sp., Proteus sp. and Pseudomonas aeruginosa. Some bacteria such as Staphylococcus aureus, coagulase negative Staphylococcus sp. and Enterobacter sp. isolated from wound infections showed stronger biofilm forming ability than urinary tract isolates. It was apparent in reviewing literatures that urinary tract and wound infections, caused by biofilm forming P. mirabilis, were resistant to antimicrobial treatment. Hence, four isolates from the strongest biofilm forming P. mirabilis were selected for further experimentation as: two isolates [PrU1 and PrU2] from UTIs and another two isolates [PrW1and PrW2] from wound infections. Antimicrobial susceptibility The antimicrobial activities of eight different antimicrobial agents (expressed as MIC values) against four strong biofilm forming isolates of P.mirabilis were determined via the micro-broth dilution method. It was clearly observed that four isolates showed a high resistance pattern against most of the antimicrobials tested. However, all were sensitive to ceftriaxone and nitrofurantoin, while only two isolates were sensitive to gentamicin and ciprofloxacin. Effect of sub-MICs of antimicrobials on biofilm adherence Results were variable between strains against the same antimicrobials. It was noticed that the use of antimicrobials in ½ MIC showed significant reduction in biofilm formation by 85% to 90 % in most of the tested isolates (P<0.01). Ciprofloxacin was the antimicrobial that provided highest percent reduction ranging from 64% to 93%, at one-half MIC and 28% to 91% reduction at ¼ MIC [Figure - 1]. The effect of antimicrobials on preformed biofilm The effect of high antimicrobial concentrations (8-1024 μg/ml) on the pre-formed biofilm was tested. As shown in [Figure - 2], the best results were obtained by ciprofloxacin which have the ability to kill almost all viable bacteria in all isolates at high concentrations. On the other hand, the biofilm biomass of the isolates PrU1-PrU2 and PrW2 begin to decrease from concentration 8 μg/ml [Figure - 3]. The other two antimicrobials had no significant effect on viable cells [Figure - 2], while they reduced the bioflm biomass of all isolates at high concentrations [Figure - 3]. Discussion The main problem associated with infections caused by biofilm forming bacteria is the low sensitivity of the bacteria to the antimicrobials used. Ruzicka et al. [8] showed that there exists a possible level of correlation between the ability of the microorganism to form biofilm and the isolation site of the strain. In the same way, our results showed that the capacity for biofilm formation by some of bacteria isolated from wound infection was more than that obtained from UTIs which may be related to variation of virulence factors according to site of isolation. In the study carried out by Smith et al. [9] on S. aureus it was revealed that the isolates originating on the skin had a significantly greater ability to form fully established biofilms than isolates taken from the blood or other body sites. Duran et al., [10] observed that the frequency of adhesin genes was detected at a high rate in S. aureus strains, isolated from skin Successful strategies that can overcome a medical biofilm formation may require the use of multiple concurrent management techniques that do not only attempt to kill the bacteria in the biofilm but also attempt to interfere with the formation of the biofilm. [3] One of these techniques was the use of antimicrobials in sub-MIC to reduce the bacterial adherence to non-living surface, as catheters. Successfully, it was found in our study that all tested antimicrobials, at sub-MIC, markedly reduced the adherence of all P. mirabilis isolates to polystyrene in a dose-dependent manner. Recent studies demonstrated that sub-MIC of some antimicrobials were effective for reducing the amount of biofilm formed by Pseudomonas aeruginosa. [11] On the other hand, it has been documented that formation of static biofilm increased when P. aeruginosa grew in the presence of sub-MIC concentrations of ciprofloxacin. [11] On studying the effect of ciprofloxacin, ceftriaxone, gentamicin and nitrofurantoin on biofilm biomass of pre-formed biofilm, the results showed that both ceftriaxone and ciprofloxacin gave the best results for biofilm biomass removal. Ceftriaxone on 8 μg/ml concentration, which is multiple of MIC, caused removal of 33-69% depending on the tested isolates. About 34-55% of the formed biofilm was removed by 8 μg/ml ciprofloxacin in only three tested isolates. Generally, there is no fixed pattern for the effect of antimicrobials on pre-formed biofilm. El-Feky et al. [12] found that MIC and 2x MIC of ciprofloxacin reduced total biofilm biomass and viable cells in biofilm by > 60% and 78%, respectively. Spoering and Lewis [13] who worked on the effect of three antimicrobials belonging to different classes explained that the ineffectiveness of carbenicillin in killing viable cells in biofilm may be attributed to slow growth of the cells inside the matrix and β-lactams antimicrobial can kill rapidly growing cells only. On the other hand, they found that ofloxacin was capable of killing biofilm cells because of its effectiveness on non-growing cells. In contrast, tobramycin was unable to kill biofilm cells in spite of its effect against non-growing cells, but this result may be attributed to the binding of the positively charged aminoglycoside to the negatively charged exopolysaccharide in biofilm so restricted permeation. [14] References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12014f2.jpg] [mb12014f1.jpg] [mb12014f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}