 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
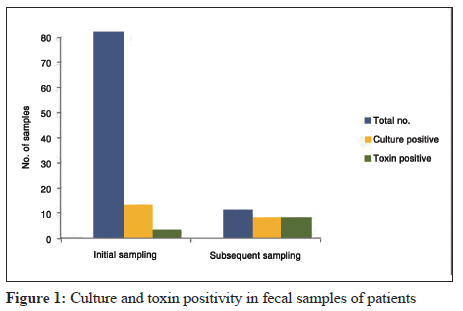
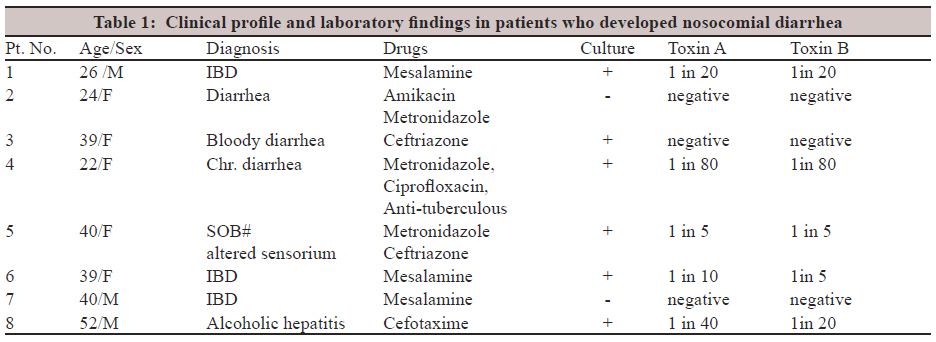
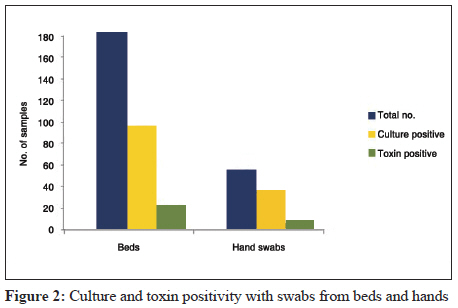
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 89-92 Brief Communication Preliminary investigation of environmental prevalence of Clostridium difficile affecting inpatients in a north Indian hospital C Vaishnavi, M Singh Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India Correspondence Address: Date of Acceptance: 30-Nov-2011 Code Number: mb12017 PMID: 22361768 DOI: 10.4103/0255-0857.93052 Abstract A preliminary study was conducted to see the prevalence of Clostridium difficile in patients and their environment in a tertiary care hospital. Seventy-nine fecal specimens from hospitalized patients, 176 swab samples from beds and 48 from hands of hospital personnel were investigated. Sixty-three patients received antibiotics and 14 proton pump inhibitors. Abdominal pain was observed in 16 patients with fever in 15 of them. C. difficile culture was positive in 12.6% patients at initial sampling but none were toxin-positive. Eight patients developed diarrhea and five were both culture and toxin-positive. Fifty-one percent of bed swab samples and 62.5% of hand swab samples were culture positive. Similarly 8.5% of bed swab samples and 4.2% of hand swab samples were positive for toxins A and B. The environmental cross-infection between patients and carriage by hospital personnel are plausible sources of C. difficile infection and spread in our hospital. Keywords: C. difficile, environment, hospitalized patients, prevalence Introduction Clostridium difficile is a well-established nosocomial enteric pathogen, particularly in the elderly. The first step in development of C. difficile colonization is the disruption of normal flora of the colon, usually caused by administration of broad spectrum antibiotics. C. difficile leads to increased patient morbidity and is often associated with increased hospital stay. The emergence of the global epidemic hypervirulent strain of C. difficile viz. NAP1/BI/O27 has led to an increased mortality. C. difficile infection has also been reported to be involved in the exacerbation of ulcerative colitis [1] and increase in cases of small bowel involvement. [2] The pathogenicity of C. difficile is attributed to elaboration of two highly potent exotoxins - toxin A and B - that bind to specific receptors on the colonic lumen leading to subsequent cell death. C. difficile is highly prevalent in hospitals [3] and spreads through resilient spores which survive for months in the environment as they are relatively resistant to most common disinfectants. Colonization occurs by oral route; the ingested spores of C. difficile survive the gastric acid barrier and germinate in the colon. Symptoms of C. difficile-associated diarrhea (CDAD) may start on the first day of antibiotic therapy or up to 6 weeks or longer after antibiotic therapy is stopped. [4] C. difficile is believed to be the leading cause of infectious nosocomial diarrhea, accounting for 20-40% of all cases [5] and is the most common cause of antibiotic associated diarrhea (AAD) in hospitals in developing countries. [5] Outbreaks of CDAD are commonly reported from hospital wards and may also result in ward closure. [6] Therefore, a preliminary investigation was conducted in a tertiary care hospital to study the prevalence of C. difficile infections in patients at initial admission and after developing nosocomial diarrhea. Swab sampling from the beddings of hospitalized patients and those from the hands of nursing personnel were also investigated to look into the environmental prevalence of C. difficile and the possibility of transmission to the hospitalized patients. Materials and Methods The study was approved by the Institute Ethical committee and conducted between April 2008 and May 2009 on clinical and environmental samples. Patients admitted to medical and surgical wards of the hospital were enrolled for the study. The clinical details of the patients were recorded on a preprinted proforma along with informed consent. The inclusion and selection criteria of the enrollment were (i) admission of patients to various wards of the hospital (for initial sampling) (ii) hospitalized patients on drugs (for subsequent sampling) and (iii) hospitalized patients developing symptoms of diarrhea, fever and/or abdominal pain (for subsequent sampling) and (iv) patients hospitalized for more than 48 hrs. Patients with insufficient clinical data and patients below 2 years of age were excluded from the study. Fecal samples obtained from 79 patients at admission were taken as the initial sampling for investigation and from those who developed diarrhea later than 48 h of hospital admission as subsequent sampling. Diarrhea was defined as the passage of three or more unformed stools in 24 h. Fecal samples were collected in Stericol vials with collection spoons attached to them (HiMedia, Mumbai, India). Apart from this hand swab samples were collected from 48 hospital personnel and swab samples from 176 hospital beds using cotton swabs pre-moistened with sterile saline and inoculated directly into brain heart infusion (BHI) broth (HiMedia, Mumbai, India). They were vortexed for 1 min and incubated anerobically at 37°C for at least 48 h for enrichment and growth of C. difficile. Subcultures were put up on cefoxitin cycloserine fructose agar (CCFA) and Columbia blood agar (HiMedia, Mumbai, India) for isolation of C. difficile. Fecal samples were similarly cultured onto selective media both directly and after alcohol shock treatment and incubated anaerobically at 37°C for 72 h. Identification of C. difficile was done by colony morphology, Gram staining and biochemical methods. Supernatants from BHI broth cultures were prepared by centrifugation at 3000 rpm for 5 min at room temperature and used for toxins A and B assay as described earlier [7],[8] using purified antitoxin A and antitoxin B (kindly provided by Dr. M. Warny, USA). Supernatants from fecal samples were similarly prepared after dilution 1 in 5 in phosphate buffer saline. In brief, 50 µl of each supernatant was taken on a clean glass slide to which ready-to-use C. difficile antitoxin A or B-coated latex beads were added. The latex beads for preparation of the reagent were purchased from M/s Sigma Aldrich Co. St. Louis, USA. The slide was gently rocked manually and checked for immediate macroscopic agglutination. The supernatant that agglutinated with latex beads coated with antitoxin A was taken to be positive for toxin A and that which agglutinated with antitoxin B as positive for toxin B. A known positive fecal sample obtained from a patient with AAD was the positive control. Two negative controls consisted of (i) an unreactive fecal sample from a healthy volunteer who had no antibiotic exposure for 6 weeks prior to testing and (ii) uncoated latex beads plus diluted test sample. All positive fecal samples from patients were further subjected to titrations by doubling dilutions and repeating the procedure. The toxin titer was determined by a positive agglutination reaction with the highest dilution of the fecal supernatant. No titration for toxins of swab samples could be carried out because of the nature of the samples. Results There were 44 males and 35 females in the study. The age range of the patients was 15-75 years. Of the 79 patients, 63 were on antibiotics and 14 on proton pump inhibitors (PPI). Sixteen of the patients complained of abdominal pain and 15 of fever. 10/79 (12.6%) of the fecal samples investigated at admission were culture positive but negative for the toxins. Of the eight (10%) patients who developed diarrhea during hospital stay, five (62.5%) were positive for culture as well as both toxin A and B [Figure - 1] up to a titer of 1 in 80. [Table - 1] shows the clinical diagnosis and other findings of the eight patients. Of the 176 bedding samples, 90 (51%) were positive for culture and 15 (8.5%) for both toxins A and B [Figure - 2]. A single sample was positive for toxin B only. Of the 48 hand swab samples, 30 (62.5%) were positive for culture and two (4.2%) for both the toxins. A lone sample was positive for toxin A only. Discussion Nosocomial acquisition and transmission of C. difficile have been well documented with outbreaks of CDAD in geriatric, [9] orthopedic, [10] medical [11] and surgical wards [12] as well as in long-term care facilities. [13] Weese et al[14] isolated C. difficile from 4.5% and 8.1% in large and small animal clinics, respectively, and from 20% of environmental sites sampled elsewhere with 66.6% strains tested producing toxins in vitro. Similarly Titov et al[15] have isolated toxigenic C. difficile from the hospital environment and the two strains identified were common to patients and the environment. Sundaram et al[16] investigated the environmental spore contamination in a General Hospital in South East England and reported the highest incidence of CDAD on the care of elderly in medical wards. These studies demonstrate the prevalence of C. difficile in the environment and its potential role in nosocomial disease. In our preliminary investigation, 12.6% of the fecal samples at initial sampling were positive for C. difficile culture, but negative for toxin production. Of the patients who developed diarrhea during hospital stay 75% were positive by culture and 62.5% of them for both the toxins. Among the patients who developed diarrhea after receiving antibiotics, 60% had fecal C. difficile toxin positivity. Additionally, 37.5% patients with nosocomial diarrhea were on mesalamine treatment for inflammatory bowel disease with 66.6% of them testing positive for C. difficile toxin. Kumar et al[17] reported a high carriage rate of C. difficile after mesalamine exposure. Surprisingly, none of the patients on PPI developed nosocomial diarrhea, but this could be because of the lower patient volume and lesser hospital stay. The incidence rate of nosocomial CDAD may vary with hospital populations and is influenced by the presence of predisposing factors, such as increased patient age, type and duration of antimicrobial therapy, severity of underlying illness and length of hospital stay. A limitation of our study is that initially though a larger number of patients were enrolled for the study, fecal samples could not be obtained at admission from all of them particularly from those in surgery ward. Thus almost all of the patients with nosocomial diarrhea did not come from surgical wards where elderly patients predominate. Secondly, many of the patients from the medical wards were discharged much before the onset of nosocomial diarrhea could be detected. This resulted in a loss of follow-up. The hospital environment is a major source of infection where C. difficile spores lurk for months, as they are resistant to heat and standard disinfectants. The organism may remain in a dormant spore phase for weeks or months, providing a reservoir for new infections. [18] Infected patients and asymptomatic carriers may serve as reservoir for the organism and help perpetuate the disease in susceptible individuals. High rates of infection have been reported among patients in double rooms and after exposure to an infected roommate. [3] The organism is present in hospitals not only from patients but also because it is present as normal flora of the infant in hospital nurseries. In the present study, even though as high as 62.5% of the hand swab samples of hospital personnel were positive by culture, only 4.2% were positive for both the toxins with a lone sample positive for toxin A only. Apart from this, 51% of the patients′ beds were culture positive with 8.5% of them also being positive for both toxins A and B and a single sample for toxin B only. The environment cross-infection between patients, and carriage by hospital employees have all been cited as plausible sources of infection. C. difficile can be recovered from the open-air wards in which no barriers are present between patients. [19] This again is a hazard and can foster the spread of C. difficile. Oldfield [20] suggested that to prevent CDAD, education and better compliance with isolation, use of gloves and hand washing were necessary. Control appears to be based on initiation or reinforcement of infection control practices rather than drug restrictions. In conclusion, environmental prevalence of C. difficile in hospitals can result in nosocomial acquisition of C. difficile as seen in the present study also. Good patient and hospital hygiene will play a role in the prevention of infection. This can be achieved by educating both the patient population and the hospital personnel from time to time. Acknowledgment The authors are grateful to Dr. M. Warny, USA, for providing the C. difficile antitoxin sera. The technical assistance provided by Mr. Babbar Raja and Ms. Monica Sharma is also thankfully acknowledged. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12017f2.jpg] [mb12017f1.jpg] [mb12017t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}