 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
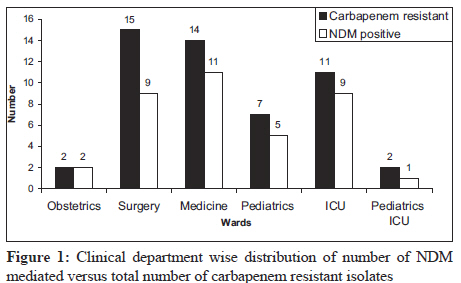
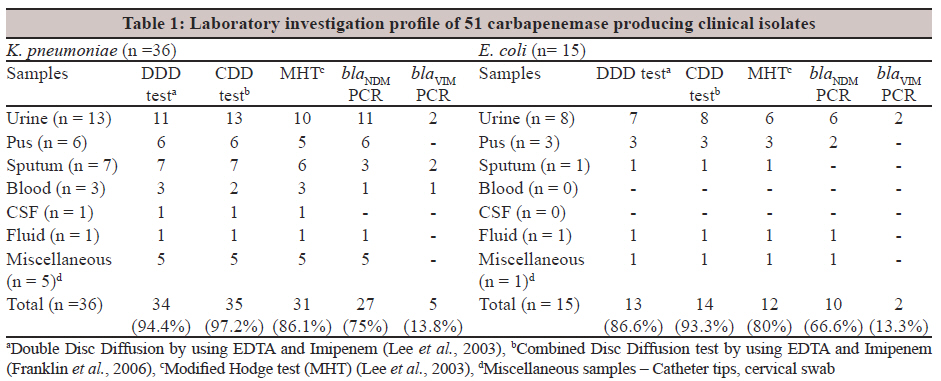
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 93-95 Brief Communication Carbapenem resistance among Escherichia coli and Klebsiella pneumoniae in a tertiary care hospital in south India S Nagaraj1, SP Chandran2, P Shamanna1, R Macaden3 1 Department of Microbiology, St. Johns Medical College, Bangalore, India Correspondence Address: Date of Acceptance: 20-Jan-2012 Code Number: mb12018 PMID: 22361769 DOI: 10.4103/0255-0857.93054 Abstract Carbapenem resistance among clinical isolates of Enterobacteriaceae, especially Escherichia coli and Klebsiella pneumoniae, is largely conferred by metallo-β-lactamase (MBL). Fifty-one non repetitive isolates of carbapenem-resistant (Meropenem and Imipenem) E. coli and K. pneumoniae were studied to determine the molecular mechanism for resistance. Presence of blaNDM and blaVIM was determined by polymerase chain reaction (PCR) and DNA sequencing. blaNDM was detected from majority of carbapenem-resistant K. pneumoniae (75%) and E. coli (66.6%). Timely detection and appropriate and aggressive infection control measures are required to control the spread of these bacteria in healthcare settings. Keywords: Antibiotic resistance, carbapenemases, New Delhi metallo-β-lactamase Introduction Carbapenems belong to the β-lactam group of antibacterial agents. Until recently, carbapenems were the choice for the therapeutic management of multidrug-resistant gram-negative bacterial infections. Currently, the spread of carbapenem-resistant bacteria has caused grave concern due to the limited choice in antibiotics for treating infections caused by them. [1] Resistance in bacteria to carbapenems is due to the production of carbapenem hydrolyzing enzymes called carbapenemases. These bacteria have the potential to spread rapidly within the hospital environment and also across continents. [2] Mechanism of carbapenem resistance is mainly due to production of carbapenemases coded by blaKPC , blaVIM and blaIMP. These belong to Class B of β-lactamases. Klebsiella pneumoniae carbapenemase (KPC) was first identified in 2000 among the isolates of K. pneumoniae in the United States of America; this mechanism has been identified in many countries and has spread across the globe. [3] A report from the United Kingdom demonstrated the presence of a new metallo-β-lactamase (MBL), named as New Delhi metallo-β-lactamase (bla NDM ), first identified in the clinical isolates of E. coli and K. pneumoniae from a Swedish patient who had traveled to India. [4] Consequent to this, there are reports across the globe of isolates carrying this resistance gene. Carbapenem resistance in Enterobacteriaceae in our hospital was not common till 2009. Identification of bacteria with reduced susceptibility to carbapenems by the disc diffusion test prompted us to determine the probable molecular mechanism for resistance among these isolates in this study. Materials and Methods Materials A total of 51 non-repetitive clinical isolates of Escherichia coli and K. pneumoniae, identified as carbapenem-resistant, were included in the study. Antimicrobial susceptibility testing The antimicrobial susceptibility was determined by the Kirby Bauer's disc diffusion method on Mueller-Hinton agar, according to the Clinical Laboratory Standard Institute (CLSI) guidelines. [5] The antibiotics tested were: Ampicillin (10 mcg), Cefuroxime (30 mcg), Cefotaxime (30 mcg), Ceftazidime (30 mcg), Gentamicin (10 mcg), Netilmicin (30 mcg), Amikacin (30 mcg), Ciprofloxacin (5 mcg), Piperacillin (10 units), Piperacillin + Tazobactam (100/10 mcg) and Meropenem (10 mcg) (HiMedia Laboratories Pvt. Ltd., Mumbai, India). Minimum inhibitory concentration (MIC) of Meropenem was determined by VITEK 2 compact (bioMerieux, Marcy l'Etoile,France). Metallo-β-lactamase detection MBL production was detected using Combined Disc Diffusion test by using Imipenem (10 μg) and 0.1 M ethylenediaminetetraacetic acid (EDTA; 292 μg) as described previously by Franklin et al . [6] This was complemented by the Modified Hodge test (MHT) and the Double-Disc synery test with imipenem (10ug) and +EDTA(750ug) for all the isolates, as performed earlier by Lee et al. [7] DNA extraction DNA extraction was performed from the bacterial isolates using alkaline lysis method. [8] Polymerase chain reaction and DNA sequencing The resistance genes blaNDM , blaVIM and blaKPC were amplified by polymerase chain reaction (PCR) by using previously published primers, NDM-Fm 5'-GGTTTGGCGATCTGGTTTTC-3'; NDM-Rm 5'-CGGAATGGCTCATCACGATC-3'; VIMF 5'-GATGGTGTTTGGTCGCATA-3'; VIMR 5'-CGAATGCGCAGCACCAG-3'; KPCF 5'-ATGTCACTGTATCGCCGTCT-3'; and KPCR 5'-TTACTGCCCGTTGACGCCC-3'. [9],[10],[11] The amplified DNA fragments were purified (QIAquick PCR purification kit; Qiagen, GmbH, D-40724 Hilden, Germany) and sequenced with ABI 3730XL (Applied Biosystems, Foster City, CA, USA). The nucleotide sequence was analysed by Basic Local Alignment Search Tool available at the National Center for Biotechnology Information website ( http://www.cbi.nlm.nih.gov/ ). Results [Figure - 1] shows the distribution of the isolates from clinical samples in the various treating units. The General Surgery, General Medicine and Intensive Care Units have relatively large number of carbapenem-resistant isolates. The clinical source of the isolates and tests done for the detection of MBL is given in [Table - 1]. Most of the carbapenem-resistant isolates were from urine samples. Fifty-one isolates resistant to Meropenem by disc diffusion method were selected. This finding correlated with MIC values obtained by the MIC assays for Meropenem. Majority of the K. pneumoniae and E. coli isolates (n = 47/51) showed an MIC >64 μg/ml, while the other four isolates had a range from 4 to 32 μg/ml. The presence of the MBL was best detected by Combined Disc Diffusion and Double Disc Diffusion as compared to MHT. Of the 36 K. pneumoniae isolates, 27 (75%) were blaNDM positive by PCR and 5 of blaNDM negative isolates were identified as blaVIM positive. Out of 15 E. coli isolates, 10 were blaNDM positive and 2 were blaVIM positive by PCR. In this study, blaKPC was not detected from any of carbapenem-resistant isolates. Further characterisation of four K. pneumoniae and three E. coli isolates for the mechanism of resistance (negative for both blaNDM and blaVIM ) was not possible as part of this study. These isolates probably have other carbapenemases like blaIMP and blaOXA or it may be due to efflux changes comediated by chromosomal AmpC β-lactamase overproduction and outer membrane protein loss. [12] Discussion Reports indicate that carbapenemases producing Enterobacteriaceae isolates seem to be increasing in number in the last few years. [1] This study showed a high incidence of blaNDM among E. coli and K. pneumoniae by PCR. Among the carbapenem-resistant Enterobacteriaceae isolates, NDM-1 was detected in 75% (27/36) of K. pneumoniae and 66% (10/15) of E. coli by PCR. Deshpande et al. reported a similar finding from a tertiary care hospital in Mumbai, in which majority of blaNDM producing isolates were K. pneumoniae and E. coli.[12] We observed that the carbapenem-resistant organisms were isolated mainly from urine samples up to 42% (n = 21), followed by wound discharge (18%) and respiratory secretions (16%). 80% (17/21) of urine isolates were positive for blaNDM , which is similar to the finding of Deshpande et al. [13] This study is hospital based and does not reflect the prevalence or incidence of NDM-1 in a community. Enterobacteriaceae contribute to a major part of the gut flora. Just like other bacteria, blaNDM producing Enterobacteriaceae are capable of colonising the gut of patients. They in turn serve as reservoirs for spreading infection or contaminating the environment and fomites, especially in healthcare settings. In order to control the spread, disinfection measures need to be followed as contact isolation of these infected/colonised patients is not routine and may not be feasible in all healthcare institutions, especially in the developing countries. Microbiological surveillance of the rectal flora at the time of admission (especially in patients who have already been exposed to antibiotics and healthcare interventions) and contact isolation of potentially colonised/infected patients will go a long way in preventing contamination of the environment and spread to other patients. In addition, appropriate use of carbapenems will also prevent selecting resistant bacteria in a given geographical area. The present study was designed as a pilot study; so, the sample size was small and the isolates were consecutive and not random. Possibility of nosocomial, and therefore a predominant clonal pattern cannot be ruled out. For confirming the possibility of nosocomial spread, further study is required with higher sample size, more demographical characteristics, hospitalisation data of patients and molecular methods to determine clonality. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12018f1.jpg] [mb12018t1.jpg] |
| |||||||||
{kind=link}
{kind=link}