 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
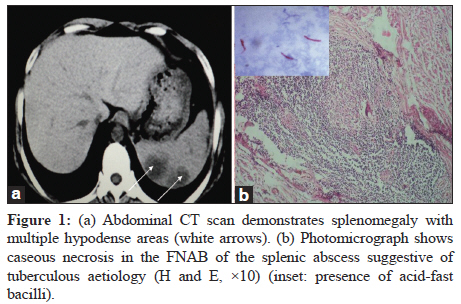
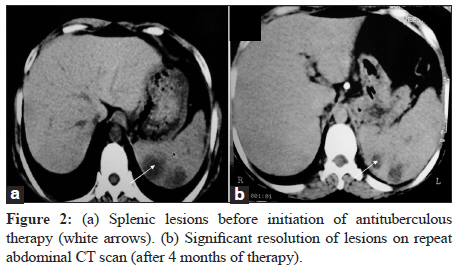
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 101-103 Case Report Isolated tubercular splenic abscess: Can we defer splenectomy? Our single experience with anti-tuberculous therapy alone S Ray, S Kundu, M Goswami, D Sarkar, M Saha Department of Medicine, Medical College and Hospital, Kolkata - 700073, India Correspondence Address: Date of Acceptance: 06-Sep-2011 Code Number: mb12021 PMID: 22361772 DOI: 10.4103/0255-0857.93060 Abstract Isolated splenic tuberculosis is an exceedingly rare clinical condition. Microbiological confirmation of diagnosis in such cases is quite difficult. We encountered the case of a 35-year-old female, who presented with persistent low-grade fever and weight loss. The CT scan of the abdomen revealed multiple hypodense splenic lesions. No primary focus of infection was detected in any other organs. Fine needle aspiration of splenic lesion revealed acid-fast bacilli on Ziehl-Neelsen stain. With anti-tuberculous therapy, the lesions regressed significantly in size. We stress that splenic tuberculosis should be considered as a diagnostic possibility even in immunocompetent individuals and choose combination antituberculous therapy as the first line treatment with consideration of splenectomy depending on response. Keywords: Splenic tuberculosis, acid-fast bacilli, antituberculous treatment Introduction Tuberculosis (TB) still remains a major health problem worldwide, despite notable advances in diagnosis and treatment of the disease. [1] The disease may present as pulmonary and extrapulmonary forms with varying clinical presentations. Extrapulmonary form comprises almost 15% of all cases [2] and splenic TB is a rare clinical condition. This form of TB is normally seen as part of military TB and is rarely present as an isolated entity. Isolated splenic involvement is very unusual with only a few case reports and studies mentioning this presentation to date. [3],[4],[5],[6],[7],[8],[9] Literature search revealed some three to four reported cases from different countries including India during the last few years. [6],[7],[8],[9] The incidence of splenic TB is variable depending on the prevalence of the disease in a particular geographical area. Isolated splenic TB often poses diagnostic complexity and therefore, likely to be misdiagnosed as splenic abscess, carcinoma of spleen, lymphoma, or metastasis. The diagnosis is often delayed due to its non-specific clinical presentation and difficulties in confirming diagnosis. Here, we report a case of primary TB of spleen in an immunocompetent female presenting as splenic abscess. Case Report A 35-year-old non-diabetic woman from a middle-class family presented with a 3-month history of low-grade fever off and on, malaise, and weight loss. Fever was associated with night sweats. However, there was no history of cough, haemoptysis, breathlessness, anorexia, or other gastrointestinal symptoms. Before admission, she had been treated without having any definitive diagnosis. She neither had any significant illness nor had any contact with a patient of TB or human immunodeficiency virus (HIV) infection. On examination, she was thin built and moderately nourished, having fever with high temperature (up to 103°F) especially during evenings and mild pallor. Abdominal examination revealed an enlarged spleen without any hepatomegaly. Respiratory and cardiovascular system examinations were non-contributory. Complete haemogram showed normocytic anaemia and high erythrocyte sedimentation rate (ESR) of 90 mm in the first hour. The tuberculin test was positive (18 mm). The HIV serologic test was negative. The bone marrow aspiration study was normal. Blood biochemical profiles were also within normal limits. The chest x-ray revealed no abnormalities. Abdominal ultrasound revealed moderately enlarged spleen with multiple ill-defined geographic areas of hypoechogenecity. In view of these findings, we decided to have a contrast-enhanced computed tomography (CT) scan of the abdomen and to obtain a biopsy from the lesion. The CT of the abdomen showed multiple well-defined hypodense lesions suggesting abscess or metastases [Figure - 1]a. There was no bowel thickening, lymph node enlargement, or free fluid in the abdomen. A CT-guided fine-needle aspiration biopsy (FNAB) was performed. The cytomorphology showed granulomas with areas of caseation in the centre surrounded by a variable number of Langhans giant cells and epithelioid cells accompanying inflammatory cells infiltration, favouring the diagnosis of TB [Figure - 1]b. A few acid-fast bacilli were noted on Ziehl-Neelsen (ZN) staining [[Figure - 1]b; inset]. Culture and PCR-based confirmation could not be contemplated due to inadequacy of sample. Splenectomy was not performed because of unwillingness from the part of patient despite proper counselling. Therefore, a provisional diagnosis of isolated TB of spleen was made and the patient was put on combination antituberculous regimen (isoniazid 300 mg/daily, rifampicin 600 mg/daily, ethambutol 800 mg/daily, and pyrazinamide 1.5 gm/daily). After 4 months of drug therapy (Initially four drugs for 2 months, then two drugs), she became afebrile and gained weight, with an improvement of general condition. A repeat CT scan of the abdomen (done after 4 months) showed significant resolution of splenic lesions [Figure - 2]. Treatment continued with two drugs (isoniazid 300 mg/daily; rifampicin 600 mg/daily) for next 2 months. She completed the 6 months′ treatment and now is on our follow up. No signs of recurrence have been found till date. Discussion TB presents as a systemic disease involving pulmonary and extra-pulmonary organs. Abdominal organ involvement was observed in 11% cases of extrapulmonary TB. [2],[10] Splenic TB occurs in two forms. The first form is encountered during military TB, especially in immunocompromised patients. Spleen is the third most commonly involved organ (75%) in the setting of miliary TB (first and second being lung 100% and liver 82%, respectively). [11] The second form is primary involvement of spleen which is extremely rare, even rarer if it occurs in immunocompetent person, as in our patient. A majority of the information regarding splenic TB is in the form of case reports. There are only sporadic cases of splenic TB in immunocompetent patients. [5],[7] TB should be considered as a diagnostic possibility in patients presenting with FUO and splenomegaly especially in areas where the disease is prevalent. [2],[12] No specific symptoms will be of help for establishing the diagnosis of splenic TB. Ultrasonography (USG) of the spleen can be useful in diagnosis of splenic TB and therapeutic response assessment. It is a cost-effective and non-invasive modality, and is especially relevant as a screening tool. In a case series from India, most common ultrasound and CT findings were single or multiple hypoechoic focal lesions, splenic abscess, calcifications, and isolated splenomegaly. CT demonstrated lesions in most of the patients having ultrasonographic findings of isolated splenomegaly. [3] However, histopathological diagnosis is required to pinpoint the aetiology. There are controversial reports from studies showing sensitivity of fine needle aspiration cytology (FNAC) in the diagnosis of a tuberculous pathology in the spleen. [13],[14] Tubercular infection can be histopathologically identified by the presence of typical caseation along with granuloma of epithelioid cells and Langhans giant cells. Final diagnosis may need splenectomy although CT-guided splenic puncture and aspiration biopsy is emerging as a more ideal and popular methods nowadays. Laparoscopy has role in the diagnosis of splenic TB and has proved to be a minimally invasive approach avoiding unnecessary splenectomy specially when there is reluctance of patient to accept this. In case of solitary splenic TB, microbiological and molecular examinations are necessary in establishing etiological diagnosis. [9] Molecular techniques like real-time PCR can be used for detection of tubercle bacilli directly on clinical specimens but they have limited role in resource poor, developing countries. In most of the reported data of splenic TB, patients presenting with FUO and splenomegaly had undergone splenectomy for confirmation of diagnosis. Evidences support use of antituberculous therapy alone in splenic TB where a definite diagnosis can be reached without splenectomy. [2],[15] A treatment similar to that for other extrapulmonary sites is recommended. A few controlled studies suggest a 12-month course of anti-tuberculous treatment to be appropriate for the treatment of patients with splenic TB. However, there are also reports available showing inadequate or the absence of response to antituberculous therapy without splenectomy. [6],[11] In our case, the patient presented with the only symptom of persistent fever. Careful abdominal examination revealed only splenomegaly. Contributory laboratory data consist of anaemia, elevated ESR, and positive tuberculin test. Our experience although in a single case showed that antituberculous drugs could be used alone to treat tuberculous splenic lesions. A surgical procedure may be required when the patient is not responding to treatment. The case being reported is one of the very few reported cases where diagnosis was confirmed by demonstrating AFB on ZN stain. It also highlights that an image-guided aspiration biopsy can obviate the need for more invasive diagnostic surgical procedures and expedite the planning of therapy. Acknowledgment The support from EKO CT and MRI scan centre (A unit of EKO Diagnostic PVT.LTD) - A Joint Venture with EKO Diagnostic Pvt. Ltd and Dept. of Health and Family Welfare, Govt. of West Bengal in the diagnostic work-up of the patient is gratefully acknowledged. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12021f1.jpg] [mb12021f2.jpg] |
| |||||||||

{kind=link}
{kind=link}