 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
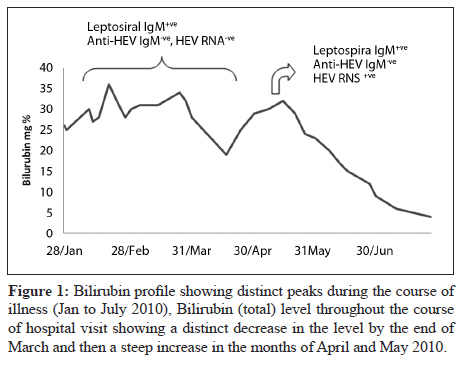
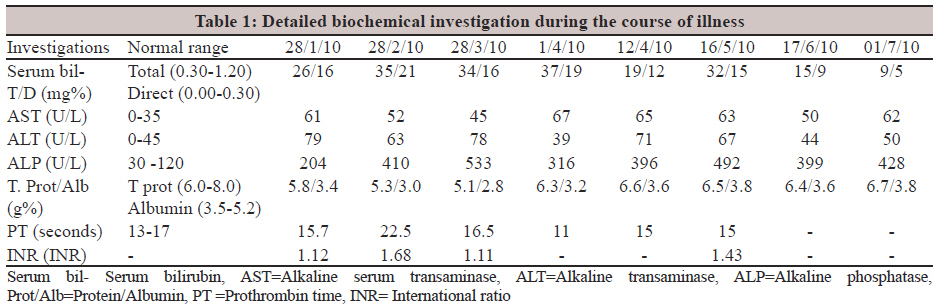
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 103-106 Case Report Prolonged jaundice attributed to super infection of hepatitis E virus in a case of resolving leptospirosis MP Singh1, M Majumdar1, A Sharma2, Y Chawla2, RK Ratho1 1 Department of Virology, Post Graduate Institute of Medical Education and Research, Chandigarh, Punjab - 160 012, India Correspondence Address: Code Number: mb12022 PMID: 22361773 DOI: 10.4103/0255-0857.93067 Abstract India is endemic for both Leptospira and hepatitis E virus (HEV). The clinical presentations of these diseases have overlapping features. We report a case of superinfection of HEV in a patient with resolving leptospirosis with underlying Hodgkin lymphoma. The diagnosis of HEV in our case was established by HEV-RNA PCR as our patient was immunosuppressed. The present study highlights the need for molecular diagnosis in the case of HEV infection with strong clinical suspicion and negative serological results. Keywords: Hepatitis E virus, leptospirosis, superinfection Introduction Leptospirosis is a zoonotic disease, caused by spirochetes and is endemic in India. [1] It is characterized by a broad spectrum of clinical manifestations varying from self-limiting anicteric illness to severe form (Weil's syndrome) presenting with jaundice, renal failure, haemorrhage and meningitis/meningoencephalitis. The disease is transmitted through contact of mucous membranes or broken skin with water or ingestion of food, vegetation contaminated with the urine of infected animals. India is also endemic for hepatitis E virus (HEV) infection and many water-borne outbreaks have been reported. [2],[3] HEV clinically presents with a self-limiting acute hepatitis or fulminant hepatic failure, with a sudden onset of hepatic encephalopathy, coagulopathy, jaundice and multi system organ failure. India is endemic for these pathogens and both these diseases have a common mode of transmission. Hence, there are chances of dual infection. The clinical spectrum of the two disease overlaps, further complicating the diagnosis. We report a case of HEV super infection on resolving leptospirosis in a patient with underlying Hodgkin's lymphoma. Case Report A 28-year-old male presented to the hepatology outpatient department on 1 April 2010 with complaints of yellowish discoloration of skin, sclera and urine. It was associated with pruritus and abdomen pain. The patient′s history dated back to 3 months when he had an episode of high grade, intermittent fever which lasted for a week. This was followed by development of jaundice. The patient did not give any history of gastrointestinal bleeding, altered sensorium, and seizures. On physical examination, the patient was conscious, afebrile, there was no clubbing, lymphadenopathy or pedal oedema. On systemic examination, the abdomen was soft, liver was 4 cm below the right costal margin, firm and nontender. The ultrasound examination revealed an enlarged liver and a normal spleen. He was hospitalized on three occasions in local hospitals between January and March 2010 because of jaundice, where he was diagnosed as a case of leptospirosis on the basis of positive anti-leptospira IgM by the enzyme-linked immune sorbent assay (ELISA). Despite treatment, the jaundice progressed because of which the patient was referred to our institute. The patient was admitted from 1 April to 5 April 2010 in our centre and extensively investigated after taking written informed consent. His autoimmune markers namely LKMA, ANA, ASMA, AMA were all negative, so also the viral markers like anti-HAV IgM, HBsAg, anti-HBc-IgM, anti-HCV, HCV RNA quantitation assay, anti-HEV IgM, anti-VCA IgM, CMV IgM, HSV IgM and dengue IgM. He however responded to general supportive therapy and ceftriaxone (2 g IV, BD for 7 days). The bilirubin levels of the patient during the entire course of illness are depicted in [Figure - 1]. The detailed biochemical parameters are shown in [Table - 1]. During this time, the patient as a part of local religious belief took some traditional medication which involved drinking water from a well where hundreds of jaundiced patients were supposed to get cured. Unfortunately, the patient's jaundice worsened and he presented back to the department after a month of decreasing jaundice. Due to a relevant history of drinking water from a common source leading to cholestatic jaundice within a week, enteric hepatitis viruses were highly suspected in the present episode. However, both anti-HAV and anti HEV IgM were found to be negative. Due to strong clinical suspicion, the patient's blood collected at this point of time was subjected to detection of HEV RNA by reverse transcriptase polymerase chain reaction (RT-PCR) as described by (Kumar et al., 2007), which detects the RNA-dependent RNA polymerase gene and it was found to be positive. [4] This was confirmed by taking a repeat sample after a week which was also positive for HEV RNA. The PCR product was subjected to sequencing after gel purification and the obtained sequence was analysed using the NCBI basic local alignment search tool and was found to have 95% sequence similarity with reference North Indian HEV strain (AF459438.1), hence found to be genotype 1. Retrospectively, the first sample collected on 2 April 2010 was tested and found to be negative for HEV RNA. Also, another sample collected on 19 July 2010 was found to be negative for HEV RNA. The anti-HEV IgM antibodies consistently remained absent in all the sequential samples. Thus, it is apparent that the patient initially presented with leptospirosis as evident from a positive anti-leptospira IgM and later on during the resolving leptospirosis he succumbed to HEV super infection. However, the patient had persistently elevated alkaline phosphatase and was on follow up. During this time, magnetic resonance imaging (MRI) of liver and magnetic resonance cholangiopancreatography (MRCP) were done which showed the presence of retroperitoneal lymph nodes. A biopsy of the lymph node was done and histological examination revealed Hodgkin's lymphoma. Discussion Epidemiological and clinical similarity exists between Leptospira and HEV as both these infections are transmitted through contaminated water and present with jaundice per se. However, to differentiate clinically between leptospirosis and acute hepatitis caused by enteric hepatitis viruses is difficult. A recent North Indian study has reported an increasing trend of leptospirosis [1] and also outbreaks of Hepatitis E have been reported from this geographical region. [2],[3],[4] To the best of our literature search, only few case reports of concurrent infection of HEV and Leptospira is documented and in all these cases infection with HEV was diagnosed on the basis of anti-HEV IgM. [5],[6] The present case depicts super infection of HEV on a resolving leptospirosis which presented with worsening of clinical presentation and prolonged hyperbilirubinaemia spanning over a period of more than 6 months. The diagnosis in our case was possible only by HEV RNA RT-PCR as anti-HEV IgM antibodies remained consistently negative throughout the course of illness. The conventional detection of anti HEV IgM antibodies has good sensitivity and specificity. However, detection of HEV RNA is the gold standard [7],[8] and should be carried out in cases with strong clinical suspicion and absence of anti-HEV IgM. We were also perplexed by the continuous IgM negativity in spite of RT-PCR being positive in two successive samples. We repeated all the sequential samples with two different IgM detection kits, all of which yielded similar results. At this point of time, the diagnosis of Hodgkin′s lymphoma was established in the patient, which gave us the answer for the absence of IgM antibodies. A previous study by Tavitian et al. has also shown that anti- HEV IgM antibodies may not be diagnostic in a case of immunosuppression. [9] We suggest that in cases of leptospirosis with prolonged jaundice and in areas endemic for HEV, the possibility of dual infection should be borne in mind and molecular techniques should be used for diagnosis if the conventional serology fails especially in cases of immunosuppression. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12022f1.jpg] [mb12022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}