 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
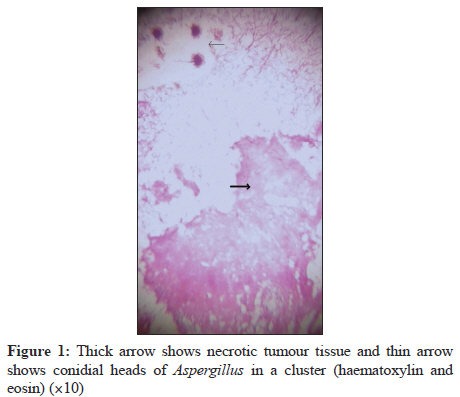
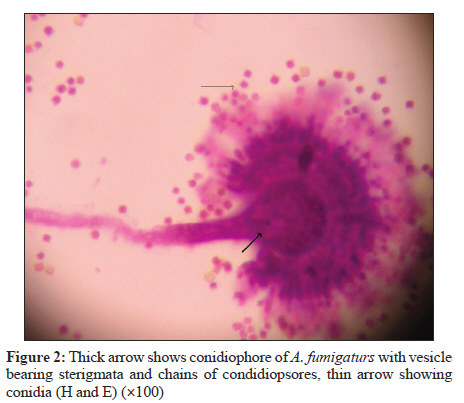
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 106-108 Case Report An unusual case of non-disseminated bladder aspergillosis in a setting of transitional cell carcinoma S Siddappa1, KM Mythri2, R Kowsalya3, M Shivalingaiah4 1 Department of Pathology, Institute of Nephrourology, Victoria Hospital Campus, Bangalore - 560002, Karnataka, India Correspondence Address: Date of Acceptance: 19-Oct-2011 Code Number: mb12023 PMID: 22361774 DOI: 10.4103/0255-0857.93071 Abstract A bladder infection of Aspergillus with no evidence of dissemination is rare. We present a case of Aspergillus infection with transitional cell carcinoma of the urinary bladder without any evidence of systemic involvement. A 65-year-old male diabetic whose main complaints were intermittent painful haematuria and nocturia had undergone nephroureterectomy a year and a half back for transitional cell carcinoma of right renal pelvis. Cystoscopy revealed bladder mucosa having fixed broad tumour with encrustation and bleeding on touch at the right vesico-ureteric junction. The histopathologic diagnosis was a high-grade transitional carcinoma with Aspergillus infection. Fungal culture of urine obtained after bladder wash yielded Aspergillus fumigatus. Keywords: Aspergillus, dissemination, transitional cell carcinoma Introduction Aspergilli are hyaline septate monomorphic moulds that commonly cause opportunistic infections in humans. Human aspergillosis is generally seen in chronic debilitating conditions. A majority of the invasive aspergillosis cases have been attributed to Aspergillus fumigatus. In immunocompromised hosts, A. fumigates represents a major cause of morbidity and mortality. Aspergillosis limited to the urinary tract is a rare disease, often occurring in immunocompromised patients. Although the kidney is the most frequently involved part of the urinary tract, invasive aspergillosis of both bladder and prostate are described. Aspergillus renal disease takes two main forms: parenchymal and pelvic aspergillosis. The first form is more common and usually both types are blood borne although occasional reports have shown apparently isolated fungal balls in the bladder without upper tract disease. In most instances, the portal of entry for fungal propagules is either through a break in the epidermis or by the way of the lungs. Noted exceptions to this include introduction to the body by means of contaminated surgical instruments, prosthetic devices or other contaminated materials or solutions associated with surgery and or routine health care. [1],[2] Here we present a rare and unusual case of aspergillosis in the bladder accompanying a bladder malignancy. Case Report A 65-year-old diabetic male presented with complaints of intermittent painful haematuria, hesitancy and nocturia for the past 3 months. The patient was a known case of transitional cell carcinoma of right renal pelvis for which he had undergone right nephroureterectomy a year and half back. On physical examination, his vitals were found to be were normal and unremarkable. There was no organomegaly, lymphadenopathy or renal angle tenderness. Routine urine analysis revealed the presence of numerous dysmorphic RBCs, pus cells (8-10 cells/hpf) and proteinuria of 3+ (300 mg/dl). The chest X-ray and bone scan were normal. His blood counts, liver function and renal function test were all within normal limits. Both fasting and postprandial blood sugars were raised with values 255 and 295 mg/dl, respectively. Urine cultures were negative for bacteria and fungi. On ultrasonography, multiple small irregular lesions adherent to the right lateral and left lateral wall of the bladder were noted. Cystoscopy was performed and revealed bladder mucosa having fixed broad tumour with encrustation and bleeding on touch at the right vesico-ureteric junction. A biopsy of cystoscopic specimen revealed malignant cells possibly of transitional origin. A transurethral resection of bladder tumour was performed. The histopathologic diagnosis was a high-grade transitional carcinoma. Also seen were acute angled branched hyaline septate hyphae with vesicles and conidiospores [Figure - 1]. Bladder wash urine specimen was obtained for culture. The sample was centrifuged and the sediment was inoculated on two sets of Sabourauds dextrose agar medium. These were incubated at 25 o C and 37 o C. Direct 10% KOH mount of the sediment revealed hyphal filaments. Fungal culture yielded Aspergillus species. Colonies were identified as Aspergillus fumigatus both macroscopically and microscopically by observing the colony characteristics and by hematoxylene eosin preparation, respectively [Figure - 2]. The patient was diagnosed as having aspergillus infection with transitional cell carcinoma of the urinary bladder without any evidence of systemic involvement. Intravesical mitomycin was administered post biopsy. Radical cystectomy with ileal conduit was finally performed. The post surgical period was uneventful and the patient was discharged with advice for regular follow-up. Discussion Aspergillus species are saprophytic, thermotolerant fungi that are ubiquitous in the air and the environment. Aspergilli comprise a group of rapidly growing; hyaline moulds that commonly cause opportunistic infections in humans. Aspergillus species can produce a spectrum of diseases, including allergic bronchopulmonary aspergillosis, aspergilloma, chronic necrotizing aspergillosis and life-threatening invasive aspergillosis. In addition, endocarditis, paranasal sinus granuloma, keratits, otomycosis and onychomycoses causes by Aspergillus species have also been described. Approximately 900 species have been described and remarkably only a few species cause disease. The most common ones causing invasive disease include A. fumigatus, A. flavus, A. niger, A. terreus and A. nidulans. A. fumigatus accounts for approximately 90% of cases of invasive aspergillosis. [3] Risk factors for invasive aspergillosis include granulocytopenia in leukemic patients, neutropenia following bone marrow or organ transplantation and high dose corticosteroid or cytotoxic drug therapy. [4],[5] A bladder infection of Aspergillus with no evidence of dissemination is rare. About four different modes of presentation of isolated bladder infection with aspergillosis have been reported such as isolated infection of the bladder with high-grade transitional carcinoma, [6] isolated bladder aspergillosis as the primary presentation of non-oliguric acute renal failure, [7] Aspergillus infection with squamous cell carcinoma of the urinary bladder [8] and fungal ball formation of Aspergillus. [9] Aspergillosis of the urinary tract may occur by three ways namely as ascending infection from the lower tract, from haematogenous dissemination or due to Aspergillus cast in renal pelvis. [10] Renal aspergillosis due to haematogenous dissemination is the most common while localized infection is rare. [11],[12] Our patient was diabetic and a known case of transitional cell carcinoma of right renal pelvis for which he was treated and had received chemotherapeutic agents, several antibiotics and was catheterized during the process. Computed tomography of the abdomen in our patient did not reveal any pathological conditions. Filamentous fungal infection could have been due to prior treatment with chemotherapeutic agents and indwelling catheterizations. Because systemic aspergillosis and renal aspergillosis were not present in the patient, it is likely that the route of infection was peritubular or intraluminal contamination via an indwelling catheter and that there was no endogenous infection. Both histological and bladder washes urine culture demonstrated Aspergillus confirming the infection. In conclusion, localized bladder aspergillosis may develop in diabetic patients having received various antibiotics, chemotherapeutic agents with history of urinary catheterization. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12023f1.jpg] [mb12023f2.jpg] |
| |||||||||

{kind=link}
{kind=link}