 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
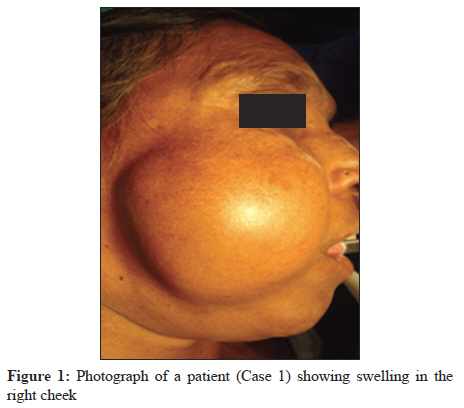
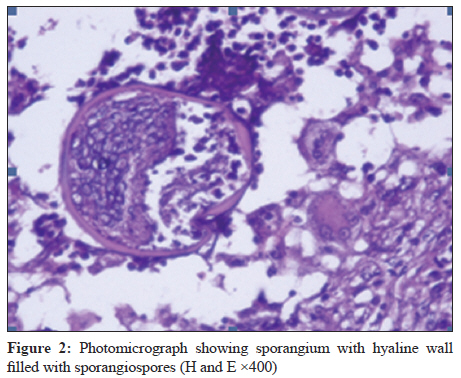
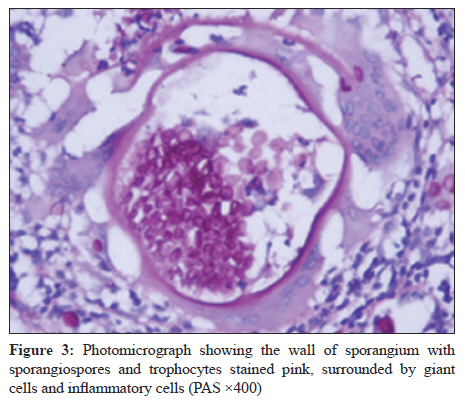
Indian Journal of Medical Microbiology, Vol. 30, No. 1, January-March, 2012, pp. 108-111 Case Report Rhinosporidiosis of the parotid duct presenting as a parotid duct cyst - A report of three cases V Sudarshan, R Gahine, A Daharwal, P Kujur, N Hussain, C Krishnani, SK Tiwari Department of Pathology, Pt JNM Medical College, Raipur, Chhattisgarh, India Correspondence Address: Date of Acceptance: 19-Dec-2011 Code Number: mb12024 PMID: 22361775 DOI: 10.4103/0255-0857.93079 Abstract Rhinosporidiosis is a chronic granulomatous infection caused by Rhinosporidium seeberi. Rhinosporidiosis has been reported from many countries but is endemic in certain parts of India and Sri Lanka. The common sites of involvement are the nose and nasopharynx followed by ocular tissue. Rhinosporidiosis is also known to involve many rare sites and may become disseminated to occur in a generalized form. Rhinosporidiosis of the parotid duct is rare and only five reported cases could be found in the literature. We report three cases of rhinosporidiosis of parotid duct presenting clinically as a parotid duct cyst. Rhinosporidiosis was diagnosed by histopathology. None of these patients had rhinosporidiosis at any other site Keywords: Histopathology, parotid duct, rhinosporidiosis Introduction Rhinosporidiosis has been reported from about 70 countries with diverse geographical features although the highest incidence has been from India and Sri Lanka. [1] In India, the disease is endemic in the states of Chhattisgarh, Kerala, Tamil Nadu, Orissa and West Bengal. Rhinosporidiosis caused by the organism Rhinosporidium seeberi is a chronic granulomatous infection involving the mucous membranes. The most common site of involvement is the nose and nasopharynx where the lesion presents as a polypoidal mass. The next common site is the eye. Lesions of rare sites have been reported such as bone, vagina, vulva, oropharynx, buccal mucosa, tongue, paranasal sinuses, skin and subcutaneous tissue, [2] penis, [3] urethra, [4] trachea, [5] larynx [6] and bronchus. [7] Rarely disseminated and generalized rhinosporidiosis occurs. [2] Most of these patients have a primary lesion in the nose. We present here three cases of rhinosporidiosis of the parotid duct who presented with cystic swelling in the parotid duct and were clinically diagnosed as ductocele. Rhinosporidiosis was diagnosed by histopathology. On searching the literature we could find only report of five cases of rhinosporidiosis of the parotid duct. The three cases reported here were detected over a period of 2 years (July 2009 to March 2011). A total of 81 cases of rhinosporidiosis were diagnosed during this period. In the 462 cases reported by us over a period of 12 years, we did not encounter any case of rhinosporidiosis of the parotid duct. [2] Case Reports Case 1 A 50-year-old female presented with swelling on the right side of cheek for the past 3 months. Local examination revealed a swelling of size 5 cm Χ 5 cm, soft in consistency [Figure - 1]. Ultrasonography of the neck showed a cystic lesion measuring 3.3 Χ 3.2 Χ 2 cm, with internal echoes in the right side of face in the subcutaneous plane. CECT showed a thick-walled peripherally enhancing lesion overlying right temporal muscle measuring 3.7 Χ 3 Χ 2.1 cm. A diagnosis of the parotid duct cyst was made. Cytology of aspirated fluid showed fair number of squamous epithelial cells along with neutrophils, few macrophages and lymphocytes. The parotid duct which was cystic was completely excised and sent for histopathology. Histopathology showed dilated ducts with the presence of chronic inflammatory cells comprised of lymphocytes and plasma cells along with the presence of giant cell granulomas. Some giant cells were seen surrounding the ruptured sporangia. Empty sporangia were also seen. A diagnosis of rhinosporidiosis of the parotid duct was made. The patient did not have any other lesion of rhinosporidiosis. As the lesion was completely excised, no further treatment was given. Ten months follow up has not shown any recurrence. Case 2 A 31-year-old male presented with painful swelling in the left cheek for the past 1 week. On examination, a swelling of 5 cm Χ 4 cm was seen in the left cheek. Overlying skin was normal. The swelling was soft and cystic and fluctuation was present. USG showed a mass of 4.2 Χ 2.6 Χ 4.0 cm with 20 cc fluid collection, thick margins and internal echoes. A clinical diagnosis of ductocele was made. During surgery, the parotid duct was found to be dilated and filled with pus. The ends of ductocele were ligated and excised. On histopathology, the parotid duct was dilated with squamous metaplasia of the lining epithelium. Plenty of chronic inflammatory cells were seen in the wall which consisted of lymphocytes and plasma cells along with few eosinophils. Sporangia filled with spores as well as empty sporangia were seen in the wall of the parotid duct [Figure - 2]. A diagnosis of rhinosporidiosis of the parotid duct was made. The patient did not have any other lesion of rhinosporidiosis in the body. The lesion was excised in toto and so no further treatment was given. One year follow up of the patient has not shown any recurrence. Case 3 A 42-year-old male presented with painful swelling over left cheek for the past 6 months with history of pus discharge in the oral cavity. On examination there was a diffuse swelling on the left cheek. Overlying skin was free and the mass was soft to firm in consistency. A clinical diagnosis of ductocele was made. So an operative procedure was planned. The parotid duct was identified which was dilated. The dilated part was dissected and excised and sent for histopathology. Histopathology showed the dilated parotid duct. Sporangia filled with sporangiospores were seen in the wall of the duct. It was surrounded by chronic inflammatory infiltrate consisting of lymphocytes and plasma cells. Few granulomas with foreign body type of giant cells were also seen. Special stains like Gomori methenamine silver, Periodic acid- Schiff stain (PAS) [Figure - 3] and Mucicarmine were also done. The patient was re-examined for any evidence of rhinosporidiosis at any other site but no other lesion was found. So a diagnosis of primary rhinosporidiosis of the parotid duct was made. Patient was not given any further treatment as the lesion was completely excised. One year follow up of the patient has not shown any recurrence. Discussion Rhinosporidiosis is a chronic granulomatous disease affecting humans and animals. The causative organism Rhinosporidium seeberi has been considered to be a fungus for a long time. Based on sequence analysis of 18S small subunit ribosomal DNA of the organism, the organism has been reclassified and included among mesomycetozoa, a clade of fish parasites that form a branch of the evolutionary tree near the animal-fungus divergence. [1] Primary lesion most often occurs in the nasal mucosa or conjunctiva where it manifests as slow growing polypoidal tumour like mass. Involvement of the parotid duct is rare with only five cases reported in the literature. [8],[9],[10],[11],[12] The first case of rhinosporidiosis of the parotid duct was reported by Topazian in the year 1967. Subsequently, there are only four published cases in the literature; all of them are from India. In all these cases, the patients presented with a cystic swelling in the parotid region and were clinically diagnosed as parotid duct cyst. Rhinosporidiosis was not suspected in any of these cases. In all three cases reported here, the patients presented with a swelling in the cheek and clinical diagnosis of ductocele was made. None of our patients had any primary nasal lesion and so rhinosporidiosis was not considered as a clinical diagnosis. Similarly, in other cases reported, the diagnosis of rhinosporidiosis was not suspected clinically as these cases presented as the parotid duct cyst. The diagnosis of rhinosporidiosis is established by histopathological examination of the affected tissue. In H and E-stained sections, the sporangia with its characteristic bilamellar thick chitinous wall and the sporangiospores can easily be recognized but can also be better visualized by special stains such as Gomori methenamine silver, PAS and Mucicarmine. Rhinosporidium seeberi can be differentiated from other organisms like Coccidioides immitis by the morphology and special stains. [8] A case of rhinosporidiosis of the parotid duct cyst not associated with nasal manifestations has been reported on fine needle aspiration cytology [10] though the fluid aspirated in one of our case did not show the presence of organism. The mode of treatment is surgical. Total excision with electrocoagulation of the lesion base is recommended for the nasal polyps. In all three of our cases, excision of the dilated portion of the duct was done as the lesion was thought to be ductocele and rhinosporidiosis was clinically unsuspected. Recurrences are known to occur due to spillage of endospores on the adjacent tissue or incomplete excision. Recurrence has not been observed in any of the three cases for the past 1 year. The only drug which has been shown to have some rhinosporicidal effect is Dapsone, which appears to arrest the maturation of the sporangia and to promote fibrosis in the stroma, when used as an adjunct to surgery. [1] The drug was not given to our patients. To conclude, the diagnosis of rhinosporidiosis was not clinically suspected in our cases, as all the three patients presented with swelling in the parotid region and there was no other lesion of rhinosporidiosis in the nose or nasopharynx. Rhinosporidiosis was diagnosed by histopathological examination of the excised tissue. Diagnosis of rhinosporidiosis should be kept in mind in all granulomatous lesions involving the mucous membranes in the endemic areas. In two of our cases there were many granulomas with giant cells and some were seen surrounding the sporangia. Rhinosporidium seeberi can easily be identified in the tissues and also sometimes in cytology because of its characteristic morphology. References
Copyright 2012 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb12024f3.jpg] [mb12024f2.jpg] [mb12024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}