 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 3, No. 2, May, 2000, pp. 81-84 Original article EFFECT OF CONTROLLED BREATHING ON PAIN TOLERANCE ARINOLA O. SANYA* AND ADEMOLA M. ADEBIYI Department of
Physiotherapy, College of Medicine, University of Ibadan. Ibadan, Nigeria. Received: 12th July 1999 Code Number: md00025 SUMMARY The aim of this study was to see if specific techniques of breathing exercises could be employed to divert patient’s attention from the severity of pain during painful physiotherapy procedures. The painful procedure used in the study was faradic stimulation of the tibialis anterior muscle. Pain threshold and tolerance were assessed using the Visual Analogue Scale [VAS]. The breathing controlled techniques employed were normal, fast-shallow and slow deep breathing techniques. The results showed that the specific breathing techniques caused no significant difference in the pain threshold and tolerance of the subjects to faradic electrical stimulation of the tibialis anterior muscle. The controlled breathing techniques might therefore not be of significant clinical value in diverting attention from pain during painful and uncomfortable physiotherapy procedures. Keywords: Controlled breathing, Pain Tolerance, Nigerians RESUME L’objectip de cette etudevd’ etait obsenver si les techniques specifiques de respiration pauvaient. etre employees pour detourner l’attention du patient de la severite de la douleur pendant les procedes physiotherapeutiques douloureux. Le procede’ douloureux utilise dans cette etule est ta stimulation electrique du muscle du libia anteueur. Les limites de douleurs et de tolerance etaient mesurees a laide de l’echelle analoque vesuelle (EAV). Les techniques de respiration controlees employees etaient les techniques de profonde respiration ralentie et lente. Les Resultals montraient que les techniques specifiques de respiration ne causaient aucune difference significative sur la limite de douleur et de tolerance des malades vis a vis de la stimulation electrique du muscle du tibia antenieur. Les technique de respiration controlee pourrait donc ne pas etre cliniquement importantes dans le detournement de l’attention des patients de la douleur pendant les proceides physiotherapeutiques douloureux et inconfortable. The physical treatments given in the management of pain are numerous depending on the type, intensity, causative or predisposing factors of pain. However, some clinical treatment procedures are themselves painful or uncomfortable to varying degrees. Forced passive stretching, some massage manipulations and electrical stimulation are examples of painful or uncomfortable physical therapy procedures. Fear and expectation lowers pain threshold and have been associated with exaggeration of pain. Psychoprophylaxis, which includes basic teaching about the pattern of pain relaxation technique, breathing exercises, attention focusing and massage have been utilised during pregnancy and labour with the aim of reconditioning the pregnant women so that onset of uterine contraction will be met with the beginning of some activities like breathing exercises rather than fear or tension. Breathing exercises actively exert the muscles involved in ventilation, they improve the strength of muscles involved in respiration and enhance the ventilatory capacity. Thus breathing exercises as usually employed in physiotherapy are found to be effective in the physical management of pulmonary disorders (Kigin 1990). Specific breathing techniques have been urged to be beneficial in psycho prophylaxis (Marshall, 1981). This present study was designed to examine the effect of two breathing patterns on a short term painful physiotherapy procedure as in electrical stimulation of muscles. The main aim of this study was to ascertain whether some breathing techniques could be employed to divert attention or minimise or dampen pain during some painful or uncomfortable procedures in physical therapy such as in forced passive stretching of soft tissue, and other forms of manipulative techniques. MATERIALS AND METHODS SUBJECTS: Twenty-two normal subjects, who were volunteer pre-clinical Physiotherapy, Medical and Dental students of the College of Medicine, University of Ibadan, Nigeria., participated in the study. Informed consents were sought and obtained from the subjects. They were made up of five females and seventeen males. Their ages ranged from 20 to 25 years with the mean ± standard deviation being 21.727 ± 1.357. None of these subjects had experienced electrical stimulation of muscles prior to time of study. INSTRUMENTS
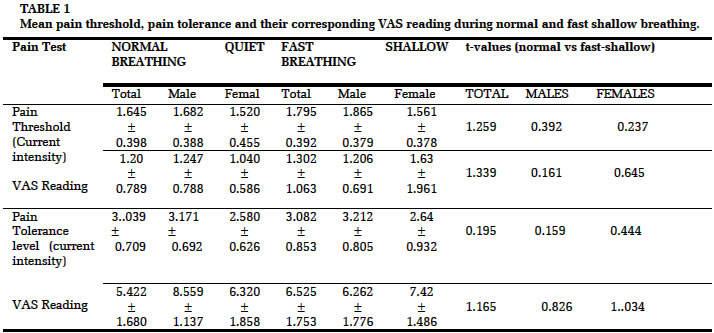
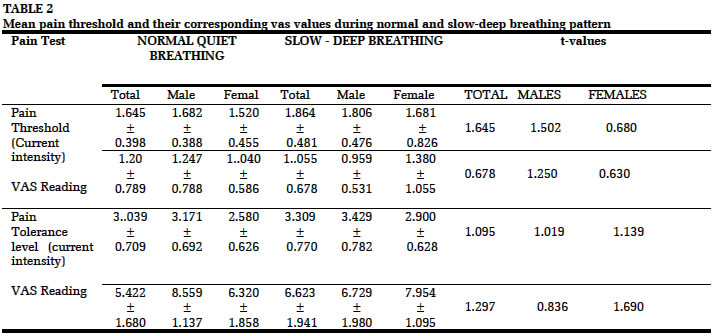
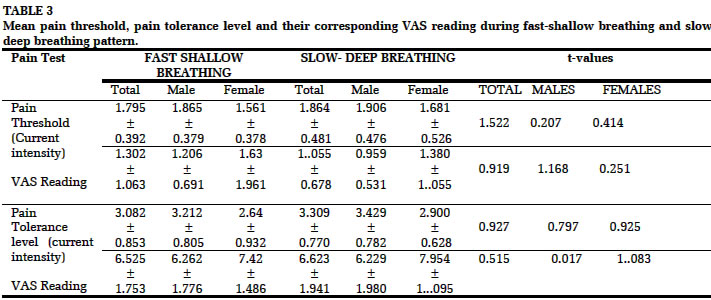
PROCEDURES The subjects were informed that the study was to investigate their sensitivity to pain and that the faradic current would cause muscular contraction. The subjects were told that immediately they experienced the slightest perceptible prickling pain sensation, they should give verbal indication of onset of the sensation and also indicate the intensity of this pain on the VAS. The corresponding level of current intensity was noted; these constituted the threshold values. Subjects were then told to bear the pain as much as they could, when they could no longer bear the discomfort they were asked to verbally indicate immediately. The intensity of this pain on the VAS and the corresponding current intensity were also recorded. These set of data constituted the tolerance values. All the subjects were given specific training on the rate and patterns of normal breathing, fast-shallow breathing and deep-slow breathing. The fast-shallow breathing pattern was taught at a rate of about 40 per minute while deep-slow was taught at a rate of about 10 per minute. With subjects in half lying position the indifferent electrode was placed around the head of the fibula, while the active disc electrode was placed at the appropriate motor point of the tibialis anterior muscle. During the first round of faradic stimulation, the subjects breathed normally. The threshold and tolerance level of pain ratings on the VAS as well as the corresponding current intensities were noted. For the second round of faradic stimulation the subjects performed the “fast-shallow” breathing pattern at a rate of about 40 per minutes. While the subjects’ tibilais anterior muscles were stimulated, the pain tolerance level stimuli (current intensities) were noted and recorded with their corresponding pain intensities (VAS ratings). For the third round of stimulations, while subjects performed the “slow-deep” breathing exercise at a rate of about 10 per minute, the tibialis anterior muscles was stimulated by faradic currents, pain threshold and pain tolerance level stimuli (current intensities) were determined and recorded with their corresponding VAS ratings. TREATMENT OF DATA The mean and standard deviation of each pain threshold stimulus, pain tolerance level stimulus and their corresponding current intensities were found for each breathing pattern, for the whole group, for the male and female groups separately. Paired t-test was used to find if the differences between the pain threshold stimuli and pain tolerance stimuli for 3 controlled breathing sessions were significant for the whole group and for the sex groups. RESULTSThe mean and standard deviation of the pain threshold and pain tolerance level of stimuli with their corresponding readings from VAS obtained during normal breathing compared with the readings obtained during fast-shallow breathing pattern for the whole group and sex groups as shown in Table 1. Changes noticed in pain threshold and pain tolerance level stimuli and their corresponding pain intensities obtained from VAS were not significant (P> 0.05). Table 2 shows the mean and standard deviation of the readings obtained during normal breathing compared with those obtained during slow-deep breathing technique. Changes noticed both in current intensities and VAS readings were not significant (p>0.05). Table 3 shows the mean and standard deviation of the readings obtained during fast-shallow breathing technique compared with those obtained during slow-deep breathing technique. Changes noticed both in current intensities and VAS readings were also not significant (P>0.05). DISCUSSION Controlled breathing patterns have always been one of the important components of psychoprophylazis. While deep breathing pattern specifically is part of relaxation technique (Marshall, 1981 and Mitchell 1985). Buxton (1970) however queried the importance of breathing techniques during the labour and claimed that they rather cause hyperventilation and increased the stress and anxiety, which actually they purported to relieve. Noble (1980) supported this claim and Mckenna (1985) also advised that mothers should be encouraged to breathe normally during labour and the breathing patterns inclusion in psychoprophylaxis is actually becoming obsolete. Some authors have however supported the fact that breathing techniques have pain threshold raising effects not only in obstetrics but also in the laboratory (Marshall 1981; Cogan and Kluthe, 1981; Mulcahy and Janx 1973). The mechanism by which these breathing techniques achieved their pain relieving and pain threshold raising effects had been said to be rather psychological because their accurate performance requires concentration which in turn raises pain threshold (Marshall, 1981). In this present study no statistical differences were noticed in both pain threshold and pain tolerance level stimuli using both fast-shallow and slow-deep breathing patterns, when compared to readings taken in normal breathing. This result tends to be in agreement with the results of Cogan and Kluthe (1981). In their experiment, the six subjects in their patterned breathing group showed what thy described as “ not reliable” change in their pain threshold using electro-sphygmomanometer compared with their control group. On the other hand Mulcahy and Janx (1973) recorded significant increase in their 20 subjects of both sexes compared with their controlled group and the initial reading. They used both fast-shallow and slow-deep breathing patterns and attention focusing all of which were performed in quick succession as the pain threshold stimulus was being determined using sphygmomanomter. The attention focusing used here might be responsible for the differences in the result and that of the present study and study of Cogan and Kluthe (1981). The non-significant effect noticed in this study and that of Cogan and Kluthe (1981) could be due to attention distraction from pain which has been said to accompany the accurate performance of these breathing patterns (Marshall, 1981). Meanwhile, relaxation and attention focusing has been documented to have pain relieving effects (Cogan and Kluthe 1981, Stevens and Heid, 1977). In conclusion, it is likely that the effects of psychoprophylaxis cannot be totally associated with breathing patterns but other constituents of the programme. If these constituents of programme are carefully studied and probably combined with some breathing techniques pain could probably be significantly dampened during painful physical therapy procedures. REFERENCES
© 2000 - Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md00025t1.jpg] [md00025t2.jpg] [md00025t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}