 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 3, No. 2, May, 2000, pp. 97-104 Original article THE INFLUENCES OF IONIC CONCENTRATIONS AND THE INTERVALS BETWEEN CURVES ON VASCULAR TISSUE RESPONSES ANDREW C. UGWU** AND JOHN C. McGRATH+ *Smooth Muscle
Physiology Unit, Department of Physiology, School Medicine, University of Benin, Benin City. NIGERIA and +
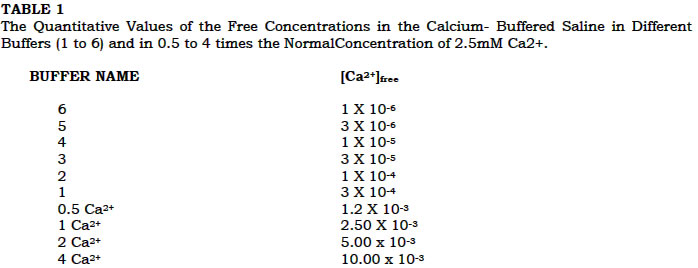
Institute of Biomedical Sciences, University of Glasgow, Glasgow, G12 8QQ. UNITED KINGDOM. Received: October 1999 Code Number: md00029 SUMMARY The effect of pre-exposure ("priming") of vascular smooth muscle to different levels of calcium concentrations before the construction of the normal concentration - response curves (CRCs) in different calcium concentrations, was investigated. The results showed that when the rat tail artery was primed with 3mM noradrenaline (NA) in 0.3mM Ca2+ or 2.5mM Ca2+ before constricting CRCs, desensitization was produced more quickly in the tissues primed in 2.5mM Ca2+ than the ones primed in 0.3mM. In either case, however, the sensitivity of the tissue later became reduced but more “stable.” This stable level is determined by the calcium concentration during priming and the maximum calcium concentration of the tissues’ CRC. The study apparently suggests that priming tissues at 0.3mM with CRC maximum at 0.3mM Ca2+ is more sitale for avoiding progressive desensitisation than when the tissue is primed in 2.5mM and its CRC maximum taken to 5mM Ca2+. It follows therefore that high calcium concentration or calcium overload reduces tissues’ sensitivity. The effect of length of intervals between calcium concentration-response curves on the desenitisation of the rat tail artery was also examined. It was observed that desensitisation was not a functionof time elapsed before first testing, but interval between curves as well as some other factors. The progressive loss of sensitivity could attenuated by increasing the interval between curves. Also increasing the tissue stabilisation period beyond an optimal level does not confer on the tissue a greater or lesser sensitivity. Key Words: Priming -Calcium Concentration-Respons-Noradrenaline-Interval Lenghts-Desensitisation-Stabilisation RESUME L’ effect de l’exposition des muscles vascularies non. stries aux differentes concentrations du calcuim (ca) suivit de la construction des curbes de concentration normale - reaction ces differentes concentration du calcuim etact experimente Les resullats ont montres que lorsque liartese de la queue du nat etait expose avec 3 um de noradrenaline (NA) dans 0.3 Mca2+ ou 2.5 mM Ca2+. l’insensitivite’ etait produit plus rapidement dans les tissues expose a 2.5 mMCa2+ que celles a 0.3 mMCa2+. Dans chaque eas, la sensitivite’ du tissue devenait plutard reduite mais plus stable. ce niveau de stabilite est determine par la concentration du calcium pendant l’exposition et la concentration maximale du ca dans les tissues. L ‘etude aqqaremment suggere que l’exposition - reaction maximale a 0.3 mMCa2+ est plus stable pour eviter l’insensitevite’ progressive que lorsque le tissue exposee a 25 mM et sa courbe de concentration - reaction a 5 mM Ca2+. il etait obsenve que la forte dose de concentration ducalcium reduit la sensitivite des tissues. L’effect de l’intervalle du temps entre la courbe de concentration-reaction du calcium sur l’insensitivite de L’artese dela queue du ret a ete examine’ iL a ete dsere que l’ensensitivite’ n’ etait jas function du temps avant le premier test mais l’ intervalle entre les courbes bienque d’autres fucteurs. La peite progressive de l’insensitivite’ pourrait etre attenue en augmentant l’intervalle entre les courbes. Aussi augmentant la periode de stabilisation du tissue au dela d’ un niveau optimal ne confere pas plus on moins sun le sensitivite du tissue. The progressive fall in the responsiveness of vascular smooth muscle tissues with time or with consecutive periods of activation by agonists or depolarising agents was observed by some earlier workers. Various tissues that had been used by such workers include the rat tail artery (Wade et al, 1970; McGrath et al, 1987; Ugwu, 1987); rabbit ear artery (Droogmans et al, 1977); canine vessles (Walus et al, 1983). The lack of information on the possible causes of the initial decline between the first and the subsequent responses has led to the neglect of the first responses or the first concentration-response curve, the second or even the third being taken by these workers as the control curve for the analysis of test drugs. It was, however, observed that some of these workers applied a “priming” or an “activating” or a “wake-up” or a “sensitizing” concentrations(s) or dose(s) of the drug to the tissue before applying the test drugs. By this manoeuvre, these workers were able to avoid the desensitisation problem of the second and subsequent curves. We have now examined the effects of priming (that is, pre-exposure) of tissue to drugs and different calcium concentrations on the responsiveness of the rat tail artery. Different workers in the field of vascular smooth muscle Physiology and Pharmacology had given differnt period of equilibration stabilisation and intervals between concentration response curves (CRCs) to suit the conditions of their experiments. However, the rationale for the choice of these periods is not clearly indicated by such workers. Ando et al. (1994) allowed a stabilization period of at least 1 hour before experimental protocol commenced while Daly, Gordon & McGrath (1992) utilised a stabilisation period of 15-45 mins for stained tissues in their experiments. Monge et al (1991) allowed 20-30 min, before CRCs; Spedding (1985) allowed 40 min. intervals between curves; Summers and Tillman (1979) allowed over 40 min. for equilibration of their expermental tissues whil Chang and Datar (1980) equilibrated the tissues for approximately 90 mins, allowed only 10-15 mins. Intervals between curves. It was howver obvious from these that the times given for equilibration of the tissues and between curves were aimed at establishing a non-dimunitive level of the tissue responses during the experimental period, so that the sensitivity of the tissue remains optimal. The aim of this second part of the study is to investigate how changes in these periods could affect the sensitivity of the tissue responses in a typical vascular smooth muscle. MATERIALS AND METHODS Two types of protocols were adopted for the different sections of the study. while the first protocol is on concentration of calcium ions as they affect tissue responses the second protocol centred in the intervals allowed between responses of the tissues for the first protocol. For the first protocol, male Wistar rats (300-350g) were killed by a blow to the head and exsanguinated. The ventral central tail artery was rapidly removed the placed in aerated of calcium - buffered physiological saline. The proximal end of the segment was gently cleared of adhering tissues, cannulated and subsequently mounted in a 5ml jacketed organ bath. It was perfused with and bathed in, medium of similar composition at a perfusion pressure of 34 to 38mm Hg and at a flow rate of 4ml per minute. The medium was made up of the following (in millimolar concentration, except when otherwise stated):- NaCl, 111.5; NaOH, 7.5 (This was to neutralise the acidic EGTA/NTA buffers which covers the range of [Ca2+] likely to be encountered. In addition, it was to minimize interference of the buffers with other ions or the properties of the tissue preparations. (McGrath et al, 1984); NaHCO3, 24.8; KH2 PO4, 1.2; MgSO4.7H2O, 1.2; KCl, 4.7; CaCl2, 2.5; Ethylene glycol bis - (- aminoethyl ether) N,N,N1-tetracetic acid (EGTA); 2.5 N,N- bis (carboxymethyl) glycine, free acid, i.e. nitrilotracetic acid (NTA), 2.5; glucose, 2g.l-1; cocaine, 4mM; propanolol,1M and Ethylene - diaminetetraacetic acid disodium salt (EDTA), 23mM. It was maintained at temperature of 37±C and at a pH of approximately 7.3. and equilibrated with 95% 02 and 5% C02 (approximately 630mm Hg partial pressure). The six bufferd physiological saline prepared contained varying levels of Ca2+ with Buffer 6 having the lowest [Ca2+]. These buffers were used so as to assist in the analysis of the [Ca2+] within the range of the the usually "indeterminate" nominally zero calcium (McGrath et al, 1984; Ugwu, 1987). The table below shows the range of free calcium concentrations in the buffers. In the first set, the tissues were either "primed" in 0.3mM with CRC maximum as 0.3mM or 5mM Ca2+ or the "unprimed" tissue had CRC maximum as 0.3mM Ca2+ only.In the second set, tissues were primed in 2.5mM Ca2+ with CRC maximum at 5mM Ca2+. In all these experiments, comparisons made between them and their corresponding "unprimed" control tissues. The results were then presented in such a way, as to use the -Log EC30 value for each individual tissue (the calcium concentration that produces 30% of the maximum response) against time to express the tissue sensitivity to calcium (Ugwu, 1997). Thus this EC30, as we have called it, is steadily increasing (or moving to the right in the absolute graph). This value was further expressed as the negative logarithm, so that the righward shift will represent a falling index of sensitivity (Ugwu, 1997). Most of the graphs in this study were therefore drawn to show the -log EC30 values against time in minutes in order to see what happens to consecutive curves in a series. Using this method, it was easier to follow the desensitisation process, which accompanies unprimed tissue activation in the presence of varying external calcium concentration. For the second protocol, the caudal artery of the rat was the vascular smooth muscle used for these experiments. Lengths of 1-2cm of the proximal segment were prepared for recording perfusion pressure in vitro. Twenty-four rats were utilized for the purpose of these experiments from which twenty-four proximal segments were prepared. Male Wistar rats (300-350 b.wt) were killed by blow to head and exsanguinated. The ventral central tail artery was rapidly removed and placed in aerated Kreb's physiological saline. The proximal end of the segment was cannulated and subsequently mounted in a 5ml jacketed organ bath. It was perfused with, and bathed in, medium of similar composition at a perfusion pressure of 34 to 38mm Hg. The medium was made up of the following (in millimolar concentration); NaCl,199; NaHCO3, 24.8; KH2PO4,1.2; MgSO4.7H2O, 1.2; KCl, 4.7;CaCl2, 2.5,EGTA, 2.5; NTA, 2.5; glucose, 2g.1-1; cocaine, 4mM; propranolol, 1M; and EDTA (ethylene-diaminetetra-acetic acid disodium salt), 23mM. It was maintained at a temperature of 37±C and at a pH of 7.3 and equilibrated with 95% 02, and 5% CO2 (approximately 630mm Hg partial pressure). The maximal changes in the peaks of the pulsatile perfusion pressure were taken for the measurement and calculation of vasoconstrictor responses. Concentration-response curves (CRCs) for external calcium, [Ca2+] (3 x 104 to 5mM), were constructed in the presence of 3mM noradrenaline (NA)(2.5mM each). Each curve took about 45min to construct and was separated from the next curve by 15min equilibration period. This protocol was carried out for the control experiments and therefore allowed only a short "rest" period of 15min between exposure to the tissue activating agent, which was noradrenaline in this case. In the test experiments, the intervals between curves were increased to one, two and three and half hours in addition to a five hours stabilisation period, to show how these time intervals affected the tissue sensitivity to calcium. The results were then presented as in our earlier studies, in such a way as to use the -log EC30 values (30% of the control maximum response) against time to express the tissue sensitivity to calcium (Ugwu, 1987 and 1997). Using this method, it was easier to follow the desensitisation process which accompanied the tissue in the presence of varying external calcium concentrations. For both protocols the results were expressed, or represented on graphs as the mean ± SEM. Statistical analysis was performed using students' t test for paired and unpaired data, as appropriate and the 0.05 level of probability was regarded as significant. RESULTS The effect of limiting the maximum calcium concentration in the construction of calcium concentration - response curve (CCRCs) to [Ca2+] maximum levels of 0.3mM (buffer1) and 5mM (2Ca2+ - see Table 1 above - in "unprimed" and "primed" tissues are clearly shown in Figs. 1 and 2 below. When the tissues were exposed for 15mins. to NA (3mM) in 0.3mM calcium (Buffer 1) ("primed") before constructing the first CCRC (up to a limiting " maximum" of 0.3mM Ca2+ (Buffer 1) or 5mM Ca2+ (2Ca2+) - see Table 1 - desensitisation was partially arrested (Fig 1). Therefore, either priming in 0.3mM Ca2+ (Buffer 1) or taking CRCs to a "maximum" [Ca2+] of 0.3mM Ca2+ (Buffer 1) reduced desensitisation (Figs. 1 b). Combining the two was even more effective: the EC30 for the 6th CRC was not significantly different from the first (Fig.1b). Of course, the EC30 of the first CRC of the "primed" tissues (■) was slightly less effective than that of the "unprimed" (·), so that the stable level of the 1st CRC of the "primed" tissues was actually slightly desensitized when compared with that of the "unprimed" tissues for the same limiting maximum of 0.3mM Ca2+ (Fig. 1). Similarly, when the tissue were primed in 5mM Ca2+ and /or the limitimg maximum was taken to 5mM Ca2+(D) (Fig.1a), desensitisation was reduced but not as much as when the tissues were primed in 0.3mM Ca2+ and the limiting maximum taken to 0.3mM Ca2+(0) or when the tissues were unprimed and taken to a limiting maximum of 0.3mM Ca2+ (■) (Fig.1b). When the tissues were unprimed and the limiting maximum was taken to 5mM Ca2+ ( ) Fig. 1&b), these tissues experienced the greatest desensitisation; the stable levels of their CRCs being much lower than in the other protocols. Likewise, the desensitisation level of the unprimed controls of limiting maximum 0.3mM was observed to occur half way between that of unprimed controls with limiting maximum of 5mM Ca2+ and that of the tissue primed in 0.3mM Ca2+ and of limiting maximum 0.3mM Ca2+ (Fig. 1b). Priming in 2.5mM Ca2+(1 Ca2+)- see Table above) (Fig. 2) accelerated desensitisation for the first two curves, although there was some recovery thereafter. This shifted the first curve to the position of the usual second curve. The second curve was shifted to the position of the usual sixth curve (Fig. 2). Thus, While this procedure produced a degree of stability, it did so by making the tissue insensitive to Ca2+ by approximately one log unit. The results of the second protocol, on intervals between the two curves, indicate that long intervals minimize desensitisation. In our earlier experiments on the desensitisation or responses of the rat tail artery, we described the protocols as those which allowed only a short "rest" or equilibration period of 15min between exposures to noradrenaline (NA) (3mM). In the present set of experiments, we increased the "gap" between the calcium concentration responses curves (CCRCs) and this manoeuver resulted in reduced desensitisation. In such a procedure, increasing the interval to 2 hours after three CCRCs at 15min gaps ("rest" periods), partially arrested deterioration and allowed some restoration of sensitivity after a 2nd 2 hours interval (Figure 3a). This observation induced us into further increasing the intervals between curves since 2 hours appeared insufficient to allow full recovery to initial sensitivity, but indicates that some recovery towards initial levels is possible. When only one hour gaps between CCRCs were allowed, desensitisation still occured, though more slowly (Figure 3b), and this was slower than in the case of the intervals of 2 hours. However, we observed that virtually, no desensitisation occured when 3.5 hours was allowed between the 1st and 2nd CCRCs; but it did occur when a subsequent short gap of 15min was allowed before the 3rd CCRCs (Figure 4). This is indicative of tissue recovery of its original sensitivity after 3.5 hours' period. Another very important observation in our study was that a 5-hour stabilisation period of the tissues before the construction of the CCRCs instead of the usual 90mins (11/2hr), did not affect the tissue sensitivity. No desensitisation or increase in the sensitivity of the tissue as judged by the EC30 values, was observed (Fig.5). Subsequent 15mins rest periods between CCRCs again resulted in the desensitisation of the tissue (Fig.5). DISCUSSION One of the most important observations in this study is that priming the tissue in 0.3mM Ca2+ (Buffer 1) produces less desensitisation than when the tissue is primed in 2.5mM Ca2+. Similarly, the higher the calcium concentration of the tissue's CRC limiting maximum the greater the desensitisation in the unprimed tissue. But priming the tissue initially reduces the tissue sensitivity (as seen with the first curve) but later (in subsequent curves) confers on the tissue a greater stability against desensitisation. The final sensitivity of the tissue after the initial priming procedure is therefore significantly higher in primed tissues than the sensitivity of the unprimed tissues. In the unprimed tissues, no stable sensitivity is generally achieved and in such tissues,the decline in tissue sensitivity is greater with the first two CRCs of the tissue (as shown by their EC30 values - Fig. 1a & b and Fig. 2a). These first two CRCs,could well be regarded as "priming contractions" in the unprimed tissues since the tissue's sensitivity thereafter declined at significantly reduced rate than in the first two CRCs, thus showing comparable curves. The highest calcium concentration to which the tissue was exposed affected Ca2+ sensitivity. The higher the [Ca2+]o, the greater the desensitisation. This suggests that Ca overload may be responsible for the deterioration of responses in this smooth muscle as it does in cardiac muscle (Allen, et al, 1985). It has been proposed that an internal binding site for calcium on the cell membrane regulates the rate of desensitisation (Nastuk and Parsons, 1970; Debassio et al, 1976). An accumulation of excess free internal calcium, in "Ca overload", may contribute to desensitisation of this tissue via such an internal binding site. This seems to be the case also in guinea - pig ileum where excess calcium accelerates desensitisation (Magaribuchi, Ito & Kuriyama, 1973). It is of interest to note that priming in 0.3mM Ca2+ (Buffer 1) leads to less desensitisation. Therefore, another probable explanation to our observation is that on the first activation of the tissue, calcium channels open "more" than on any subsequent occasion. Therefore, if extracellular/external calcium concentration is NOT high the first time the tissue is activated, the calcium overload does not occur. Second activation of the tissue produced "less" channel opening. Therefore, if priming is the first activation of the tissues, then the first curve is equivalent to the second activation and thus produces less damage to the tissue. This is because, by the second activation (or by time the first CRC is constructed after priming of the tissue), it is probable that the large influx of calcium into the tissue cells from the calcium channels overloads the tissue with calcium ions. But because the rate of efflux of calcium is later highly overwhelmed by the rate of influx as a result of the initial surge of Ca2+ into the calls, a new homeostatic status of influx/efflux equilibrium is established in which the tissue sensitivity is now slightly decreased. In such a calcium overload process, the mechanism of regulation of the ion is by activation mechanism whereby the channel is activated. In such process, when Ca2+ binds to a channel, it becomes inactive. As [Ca2+] increased, the probability that a Ca ion will associate with the channel increases. Thus channel activity (the amount of time the channel spends open) is dependent on Ca2+ concentration (Lewis and Donaldson, 1990). In general, it can be stated that different degrees of desensitisation produced by priming in different concentrations of Ca2+ shows that priming could produce some stability of subsequent responses but that the remaining level of sensitivity will depend on [Ca2+] both during priming and in the subsequent tests. Therefore priming initially accelerates desensitisation but later leaves the tissue relatively insensitive by approximately one log unit. This stabilisation may explain why many workers initially activate their tissue preparations several times until the responses are reproducible. Clearly, avoidance of high concentrations of calcium during priming as well as during subsequent parts of the protocol leads to stable preparation, which are significantly (p<0.05) less desensitised. Another major observations in this study include the following: in the first instance, it was clear that recovery occurred with time. It is noteworthy that our main protocol, with only 15min equilibration ("rest") period between the end of one CCRC and the start of the next, allowed insufficient recovery so that desensitisation became cumulative. However although 1 hour intervals reduced the rate of desensitisation, there was need to allow a very long gap of 3.5 hours for complete recovery. From this observation it seems unlikely that such gaps would be employed by most workers so that we can assume that this type of desensitisation will commonly be present. Long intervals between CCRCs attenuated desensitisation and also allowed some recovery of already desensitised tissues. It has been noted that in the intestinal muscle of guinea pig that the degree of desensitisation and the time needed for recovery are directly related to concentration of substance P and contact time (Holzer and Petsche (1983). Considering the fact that increase in the time of stabilisation of the tissue from the usual 11/2 hour to 5hr, did not produce any difference, in the desensitisation phenomenon, it is thus obvious that we have provided evidence that desensitisation is dependent on activation by calcium, not just time. In conclusion it is apt to state that while many factors influence desensitisation, it is possible to reverse spontaneously desensitisation due to calcium overload by leaving long intervals between tests. ACKNOWLEDGEMENTS We are grateful to the Commonwealth Scholarship Commission in the United Kingdom and the Association of Commonwealth Universities for the Commonwealth Scholarship to Dr. A.C. Ugwu with which part of the study was carried out at the University of Glasgow. We are also grateful to the University of Benin Research and Publication Committee (URPC) for the Grant (Ref.No. 60/592) with which the study was concluded. REFERENCES
© 2000 - Ibadan Biomedical Communications Group
The following images related to this document are available:Photo images[md00029t1.jpg] |
| |||||||||

{kind=link}