 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 3, No. 3, 2000, pp. 123 - 128 REVIEW OF A COMMUNITY ORAL HEALTH PROGRAMME IN NIGERIA AFTER TEN YEARS ADERINOKUN GBEMI. A[1] Department of Preventive Dentistry, College of MedicineUniversity of Ibadan. Ibadan, Nigeria.[1] Address for Correspondence: Dr G.A. Aderinokun, Ibadan, Nigeria. e-mail: gpo@hjnet.com Code Number: md00039 This paper reviews the activities of a model community oral health programme (COHP) which is situated in Idikan, a low income urban community in Ibadan, south western Nigeria. The programme which has been in existence since 1988, is part of a comprehensive primary health care (PHC) delivery system that caters for the basic health needs of members of the community. The programme was designed to prevent diseases of the oral cavity and to provide basic oral care services. It comprises school health programmes, health education programmes for specific target groups, examination for early detection of diseases and provision of dental services at the clinic located on site. Within the first ten years under review (1988-1997), a total of 780 patients were seen at the dental clinic. Three hundred and eighty one were(381) males, while 399 were females and their ages spanned a wide range. Many were petty traders(43.3%), 187(23.9%) were students and 131(16.8%) were skilled artisans. Pain was almost invariably the presenting complaint. In many instances, pain was accompanied by dento-alveolar abscess. Only in a few cases did patients present for routine check-ups or for aesthetic purposes. Periodontal disease in varying degrees of severity was the most prevalent diagnosis (37.2%), and this was followed by dental caries (21.9%). Apart from these, a wide spectrum of conditions such as trauma, chronic gingivitis and necrotising ulcerative gingivitis were treated. An early diagnosis of squamous cell carcinoma was made amongst the patients attending the clinic. Extraction and dental prophylaxis were the treatments most frequently carried out. In many cases, antibiotics and analgesics were administered before the definitive treatment or referral. The clinic utilisation pattern indicates that the majority of the patients attend only once except in cases where the pain is not relieved after the first visit. Even though this programme is considered effective and appropriate, more effort is required in the area of health education to enable residents adopt more prevention oriented behaviour. Key Words: Primary Health Care, Community Health, Oral HealthPrimary health care (PHC) was adopted in Nigeria in the mid 80's as a strategy for attaining the goal of ‘health for all by the year 2000’. Oral health was not a component of PHC at the outset and in order to rectify this omission, some health practitioners evolved a model for the integration of oral health into PHC. A review of the first ten years of one of the earliest such efforts: the Community Oral Health Programme (COHP) is presented below. BackgroundThe community oral health programme (COHP), located in Idikan, Ibadan was initiated out of the conviction that the prevailing system of health care delivery could not adequately fulfil the purposes of primary and secondary prevention of diseases of the oral cavity in a developing society like Nigeria. It was also in response to results of routine surveys among school children which indicated a poor oral health status. In addition, the University of Ibadan wanted to set up a community-based oral health programme where students could be introduced to the knowledge and skills required in community dental practice. This programme commenced in January 1988. The COHP is an integral part of the comprehensive Community Health Programme of the Preventive and Social Medicine (PSM) department of the University of Ibadan. At the time the oral health component was starting, the original programme had been in existence for over 25 years. In that period, it had succeeded in encouraging the community to form a health committee, composed of highly respected members of the community and the health officers in charge of the programme. This body bears the responsibility for organising activities relating to health by soliciting the assistance of the relevant health care providers. Through this committee, advances have been made in improving sanitation, immunisation, water supply and other health-related matters. At the introduction of the COHP, members expressed enthusiasm and pledged maximum support in terms of finance and community mobilisation. The Community Oral Health Programme The COHP was designed to fulfill the following specific objectives: (a)
Prevention of dental diseases through health education programmes in schools
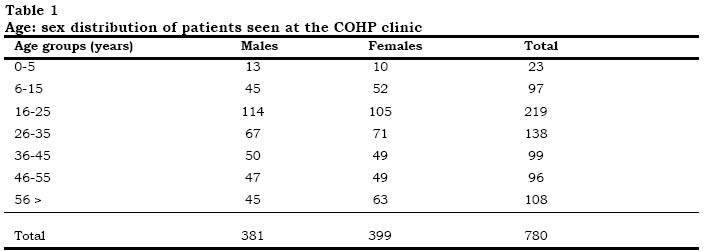
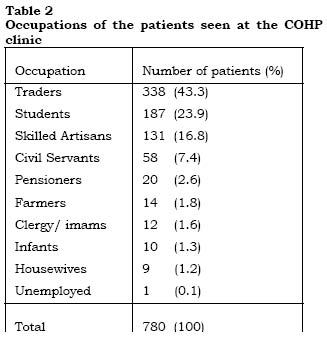
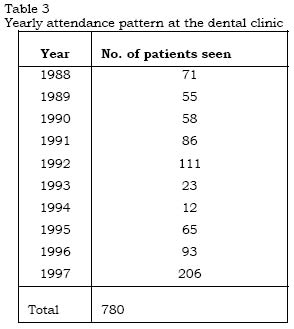
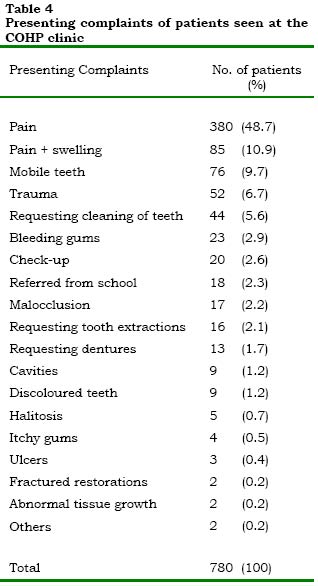
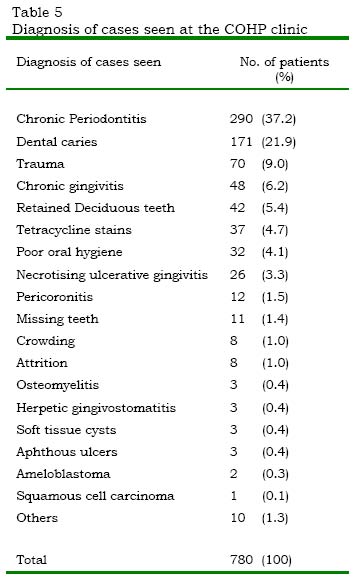
and other selected subgroups. Apart from periodic intra-oral examinations for case finding, the main thrust of activities in the three elementary schools in the area is the health education programme. The remarkable strength of the programme is derived from the educational package which was designed with maximal participation of the users - the pupils. The educational package includes: instruction on the causes and prevention of common oral diseases, demonstrations, participatory classroom activities, goal setting and reinforcement. The educational package was based on results of interviews, focus group discussions and an art contest. Class teachers, who had been trained, were expected to lead the pupils in daily class activities geared at positively influencing their knowledge, attitudes and oral health practices. The educational intervention has resulted in a significant improvement in these different parameters. Health Education Programmes for Other Specific Target Groups Health talks are periodically organised for different groups within the neighbourhood. Expectant and nursing mothers constitute an important target audience. As part of the maternal and child health welfare activities, these groups of women assemble once a week to learn about nutrition and food preparation in a practical session. Twice every year, oral health matters, especially as it relates to food choices and substitutes are discussed at such gatherings (Fig 1). Another auspicious opportunity for oral health talk is the end-of-year celebration for infants and their mothers. It has become customary to award prizes to mothers who demonstrate sound knowledge on preventive dental care. The organisers of the programme have also sought opportunities to give oral health instructions at religious gatherings. Questions concerning the services offered at the health clinic are often addressed at these gatherings. In other instances, oral health campaigns have been brought closer to the people by holding them in the family compound. Identifying Early Stages of DiseaseIn a bid to establish baseline data for different subgroups in the community, oral health surveys were conducted. It has been possible through such activities to identify cases needing treatment and to refer them appropriately. In the course of one exercise, it was noted that the prevalence of subclinical cases of necrotising ulcerative gingivitis(NUG) among pre-school children was high. Consequently, the attention of mothers was called to the need to improve their children’s nutrition and oral hygiene. Similar surveys among the adults revealed high prevalence and severity of periodontal disease resulting in tooth mortality. Provision of Basic Oral Health ServicesOne of the essential roles of oral health care is to provide adequate treatment to those with oral lesions so that the disease is arrested at an early stage and loss of function prevented. In the COHP being described here, demands for treatment are honoured and those found to need treatment during the surveys are similarly advised to get treatment. Services delivered at the clinic located in the Idikan community are very basic. Infra structural facilities which are very simple consist of a two room apartment. The inner room serves as the surgery, while the outer and bigger room is the waiting and conference room. The central focus of the surgery is the locally fabricated dental chair- the RASANO 1087 (Aderinokun, 1990) (Fig 2). Even though it is not electrically powered, it fulfils all the basic requirements of a dental chair in its maneuverability. Other equipment and materials comprise those needed for sterilisation, examination, dental prophylaxis and simple extractions. Facilities are also available for taking and casting alginate impressions, which are then transferred to the teaching hospital for further processing. Community health workers, who are trained in sterilisation procedures, record keeping, oral health education and post-operative care, are the most regular staff of the clinic. Based on a set of standing orders, they are able to provide services for the relief of pain and limit the spread of infections. Thus when the dentist is not available, they prescribe medications and refer appropriately. Being themselves members of the community, they serve as the link in planning outreach programmes as well as follow-up home visits. Since the community members can identify well with them, they constitute a strong factor in the successful implementation of the various programmes. Another significant member of the oral health team is the public health nurse. With a background in clinical nursing, she is able to oversee training and the maintenance of sterility in the operatory. She, in addition, schedules and ensures follow-up visits to the homes as well as giving health talks. A dental surgeon is always assigned to the clinic. His role is to carry out all the clinical procedures and participate in the planning and execution of field activities. Depending on patient turn-out, he may not need to be present in the clinic everyday. The programme coordinator is involved at the macro-planning and policy decision level. A dental hygienist or dental therapist would have been a useful addition to the oral health team. Students on posting are expected to participate in the health education programmes and offer treatment under supervision. They also design and conduct epidemiological studies towards their group project. Results of some of these have been published. Analysis of Patient Attendance PatternIn the period under review (1988-1997), seven hundred and eighty (780) patients were registered and seen. Three hundred and eighty one (381) of these were males while 399 were females. Their ages ranged from 1 month to 83 years, having a modal class in the age 16-25 years (table 1). Many of those attending were traders (43.3%); 187 (23.9%) were students, and 131 (16.8%) were skilled artisans (table 2). The yearly attendance pattern is presented in table 3. This shows a general increase except between 1993 and 1994 when the rate of attendance dropped drastically. The presenting complaint for a significant number of patients was pain. In many instances pain was accompanied by a dento-alveolar abscess. In few cases however, patients presented for routine check-up or for aesthetic purposes, such as tooth crowding and discoloured enamel (table 4). It is noteworthy however that attendance for the purpose of routine examination and other preventive care were more frequent in the latter years. In 1997 alone, for instance, 38 patients requested for cleaning of their teeth as well as for routine examination. As shown in table 5, periodontal disease in varying levels of severity was the most prevalent diagnosis (37.2%) and this was followed by dental caries (21.9%). Apart from these, a wide spectrum of conditions such as trauma, chronic gingivitis and necrotising ulcerative gingivitis were treated. An early stage of squamous cell carcinoma was diagnosed in an elderly female patient who presented with ulceration of the mouth. After initial treatment failed to effect a cure, she was referred to the University College Hospital, Ibadan, where histological diagnosis of the lesion was made and treatment promptly commenced. Tooth extraction and dental prophylaxis were treatments most frequently carried out. In many cases, antibiotics and analgesics were administered before the definitive treatment or referral. Analysis of the utilisation pattern indicated that patient attendance gradually increased over the years, being very scanty in the early years. It has been further revealed that the majority of the patients attended only once, except in cases where pain was not relieved after the first visit. As a measure of its appropriateness to the community being served, the clinic was assessed to have successfully catered for approximately 82% of the immediate needs of those attending, thus it was only in 18% of cases that immediate treatment could not be effected. Even in such cases, appropriate counsel was given and referral made. Similarly, because inexpensive, locally sourced equipment and materials were employed, cost to the recipients was minimal. The COHP is now efficiently operated as it is self-sustained on a revolving fund system from which salaries are paid and drugs and materials are bought. DISCUSSIONIn Nigeria, access to oral health care is limited, especially for rural dwellers who constitute the majority of the population. In order that the oral health needs of Nigeria’s rural population be adequately met, alternative oral health delivery methods are required. A number of innovative programmes have been instituted in various parts of the world to overcome peculiar oral health needs of some population groups. One of the most successful is the New Zealand dental nurse scheme which was initiated in the 1920's and which was geared towards prevention and treatment of dental problems in children (Gruebbel, 1950). Malaysia similarly sought to cater for the oral health of its people living in remote areas by establishing the Mobile Oral Health Squad Scheme. These mobile squads made use of vehicles suited to the terrain to meet the basic oral health needs of preschool children (3). Another notable programme is the Community Oral Health Care Model in Chiang Mai, Thailand. This was established with the assistance of the World Health Organisation (WHO) and is based in the Inter- Country Centre for Oral Health (ICOH) in Chiang Mai. Significant in this model is the use of a special bamboo couch on which patients are placed while their teeth are being cleaned by a unique category of oral health care workers called ‘Surface Workers’ (WHO, 1987). Like in other parts of the world, the COHP- Idikan model, has in its own way, succeeded in achieving the primary objective of improving the oral health of the Idikan community. It has, however, been plagued with many problems. The attendance recorded in the period under review was very low. This may be attributed to the low level of community awareness at the beginning. Attendance gradually improved until the political crises of 1993 and 1994 paralysed the entire programme. The COHP has recently witnessed a significant turn-out. Similarly, the cases presented have changed over the years. In the early years, many of the patients presented with complications. In recent times, relatively fewer such cases are seen. Health education which is a major part of this community work appears to be yielding good results. One may yet not be able to assess its long-term effects, nevertheless, knowledge, oral hygiene habits and indeed oral cleanliness have been improved significantly among the school children. Caries prevalence has however not decreased. Situated near the city trading centre, residents of the Idikan community are exposed to great variety of sugar and sweets. Intense efforts at educating children on food choices should go a long way in reversing this trend. Furthermore, fluoride therapy at the community level will be beneficial. In conclusion, even though there is a lot of room for improvement, especially with regards to encouraging the adoption of primary preventive behaviour in the people, one may confidently recommend the adoption of this model and its integration into existing PHC by other communities with comparative circumstances. AcknowledgmentsThis programme was at inception sponsored by a grant from the Federal Ministry of Health, Nigeria. Subsequently, grants and technical assistance have been received from the University College Hospital(UCH), and the College of Medicine, University of Ibadan, Nigeria. The contributions of past and present dental officers who have rendered services at the clinic and school health programmes are here acknowledged. The Public Health Nursing Department of UCH is similarly recognised for its immense contribution to the programme REFERENCES
© 2000 - Ibadan Biomedical Communications Group |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}