 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 5, No. 1-2, Jan & May, 2002, pp. 1-3 RISK FACTORS ASSOCIATED WITH EYE DISEASES IN IBADAN, NIGERIA *A.I AJAIYEOBA1 AND S.C.O SCOTT2 Ophthalmology1 and
General Out-Patient2 Departments, University College Hospital, Ibadan,
NIGERIA Received: February,
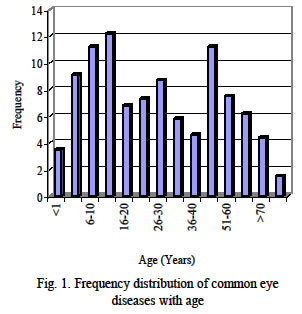
2001 Code Number: md02001 Four hundred and eighty-two patients who presented in the General Outpatient Department with eye diseases between July and December 1989 were included in the study. Risk factors considered were residential age, sex, residential address, occupation, previous eye medication and socio-economic status. The study showed that no age-range was spared even though more adults (64%) presented with eye diseases than children. There was slight male preponderance. Majority (70.7%) of patients had tried one form of treatment or the other. Most (73.2%) of the patients were of the lower socio-economic groups. School children, farmers, welders and panel beaters were particularly at risk of ocular problems from injuries with potential for blindness. These groups of people at risk of eye conditions can be targeted for health programmes e. g health education particularly at the primary heath care level. Key words: risk factors, eye diseases, Ibadan INTRODUCTION The pattern of eye diseases has been observed by Topalovo (1984) to show very wide variation in different parts of the world. Such factors include age, sex, residence socio-economic, occupation, geographical, racial, dietary, customs, tradition and the major environmental factors prevalent in that region. In a ten-year study of eye injuries necessitating admission, Canavan et al (1980) found that 84 percent of the cases were males. Also, more than three-quarters of them were less than 36 years of age, suggesting some form of effect of sex and age in eye diseases epidemiology in their study. Some eye diseases are also known to be rampant among certain professions or occupations. Certain ocular diseases are therefore gender related since certain employments are strictly reserved for a particular gender. For example Alakija (1988) observed a high prevalence of ocular morbidity amongst welders whilst Abiose et al (1981) noticed it amongst Nigerian factory workers. Also Olurin (1971) identified peasant farmers working in western Nigeria to be at high risk of vegetable injuries to their eyes. Ajayi et al (1986) emphasized the potential for blindness in such injuries if such injuries were not promptly and adequately managed. The environment is such a strong determinant factor involved in the epidemiology of eye diseases, as Rodger (1981) observed that certain infective eye diseases are relatively uncommon in temperate climates but are rampant in tropical environments. There is need to identify the risk factors associated with eye diseases, as such information will go a long way in planning strategies for prevention by health planners. Such groups of people can be targeted for intervention at the primary health care (grassroots) level. MATERIALS AND METHODS All new patients presenting to the General Out-patient (GOP) clinic of the University College Hospital (UCH) Ibadan, Nigeria with ocular problems from July to December 1989 were studied. These patients were registered and had a structured questionnaire which comprised personal, epidemiological and information on medical background administered to them. Registration included recording the name, residential address, age, sex, occupation (or father’s occupation in the case of a child) of all respondents. The questionnaire, which was administered by one of the authors (SCOS), consisted of series of questions and in the same sequence. There were a few unstandardized questions especially those pertaining to demographic data. Although during the interview, open-ended questions were asked, allowing the respondent to express him/herself, the questionnaire was filled-in along pre-determined guidelines, applied to everyone so as to make the answers comparable. In the case of children, parents or guardians were the informants. Patient’s ages were considered under the sub-divisions ‘Children and Adult’ based on the definition of Child21 in the Laws of Oyo State. Patient’s socio-economic group was based on his/her occupation or on that of the most-dependent relative according to the pattern used in the Department of Preventive and Social Medicine and Institute of Child Health, both of the University College Hospital, Ibadan. The data was analyzed using the Epi-Info (version 6) statistical package. The procedure as approved was in accordance with ethical standards of the Medical Ethics Committee of the University College Hospital, Ibadan. RESULTS Four hundred and eighty two patients were registered and included in the study. Age: The ages of the respondents ranged from less than 1 to over 70 years old. There were 174 children (36%) and 308 (64%) adults. 24% of these patients were between 21 and 50 years of age, while 49% of them were of school-going age (5 - 19 years). Figure 1 shows the age distribution of patients presenting with eye diseases in GOP clinic. Sex: The study comprised of 281 males and 201 females with a male to female ratio of 1.4:1.0. Residential Address: Majority of the patients (79%) were from within Ibadan metropolis. Previous treatment 341 (70.7%) of the patients had had some form of treatment prior to presenting in this clinic. About 30% (141) did not have any pre-treatment. Twenty-two percent of them had used some form of self-medication, either alone or in combination with other methods. However there was no significant association between previous treatment and prevalence of eye diseases. Table 2 shows the type of previous treatment eye patients had before presentation. DISCUSSION More adults had ocular problems than children, in this study, however this observed difference was not statistically significant. Earlier, Majekodunmi (1979) had reported a similar trend; with only 23.6% of her 727 patients being children. Possible explanation for this observation may be that eye symptoms may be sometimes subjective and majority of children cannot adequately express themselves, and until the signs are sufficiently gross to be noticed, children may not present in hospital. This may be the reason why some defects not usually detected until adulthood. TABLE 1: Socio-economic classes of some of the Eye-Disease Patients seen
TABLE 2 Previous treatment of 482 Eye Disease Patients
This finding therefore also corroborates the views earlier expressed by Majekodunmi (1979) that eye-diseases in children could possibly be under-diagnosed. More male than female patients had eye diseases. Both Abiose (1985) and Ajaiyeoba (1987) also noticed this trend in their studies. In our society, more males are gainfully employed while many women are full-time housewives who depend on their husbands for financial support. The fact that more men can afford hospital bill may also be a point to consider. This explanation may not hold for children registration of children is still free and the drug-cost is presently subsidized by hospital. Our observation that majority of our patients reside in Ibadan is not surprising as our hospital is strategically located within Ibadan metropolis and therefore very accessible to patients from anywhere in Ibadan. However it should be pointed out that majority of our patients come from what can be described as urban slums. The significance of this is enormous as Rodger (1981) observed that many infective eye conditions are rampant in such environments. In most African communities, the man is usually the breadwinner and has the responsibility of providing for their wives and children hence the usual classification of social class by the type of job the man is engaged in. Majority of the patients involved in this study were from the lower socio-economic class. Ajaiyeoba (1996) has linked the significance of this in relation to certain eye diseases particularly of nutritional origin to ignorance, poverty and dirty environment. Women empowerment by engagement in education to acquire knowledge and in economically beneficial vocations may be the key to improvement in the outlook of nutritional blindness in children. Also injuries to the eyes have been linked to certain occupations as hazard e. g vegetable injuries in farmers and metallic intra-ocular foreign bodies in welders by Olurin (1971). There is the need to educate our farmers and welders of the need to wear protective goggles at work. The difference between the pattern of eye diseases among the patients who had pre-treatment and those who did not have was of no statistical significance. The fact that both groups presented at this clinic suggests that the pre-treatment did not bring about any significant improvement to the ocular problem. The direct and indirect effects of this pre-treatment would need a bigger study for full assessment. In this study there was no statistically significant difference between those patients with and without treatment. However some of the patients presenting with chemical burns, corneal ulceration, corneal perforations, gave histories of having-used non-propriety methods of treating their epidemic hemorrhagic kerato-conjunctivitis. These included topical instillation of sulphuric acid electrolytes from car batteries (called ‘battery water’), salt solution, sugar solution, Cow-urine, Camphor (naphthalene balls) and others. Mcmolli et al (1986) reported an increase in the degree of morbidity caused by bot the delay and sequele from the inappropriate treatment. In this study, although the effect of the delay and non-orthodox treatments were not determined, such patients were found to present in more morbid states than does the viral conjunctivitis - a disease which normally is self-limiting. It is not surprising that most of our patients had had one form of treatment or the other before presentation. This is because drugs are freely dispensed across the counter without the patient producing a prescription authorized by an authentic medical doctor. Moreover traditional eye medications which may be harmful to the eyes are available from traditional healers who display their drugs conspicuously in most public places like the big markets. The role of traditional healers and their medications in most African communities is well known and has been documented by Ayanru (1982). Ayanru (1974) had earlier observed that harmful traditional eye medication could lead to blindness. It is desirable to identify the above risk factors involved in the causation of eye diseases for the simple reason that it becomes imperative and easier to target these groups of people for health intervention purposes. REFERENCES
The following images related to this document are available:Photo images[md02001f1.jpg] |
| |||||||||

{kind=link}