 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
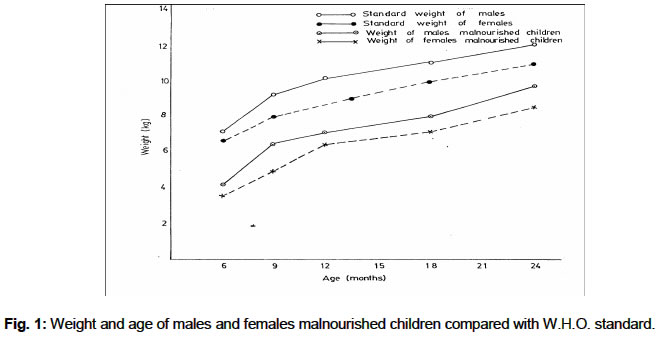
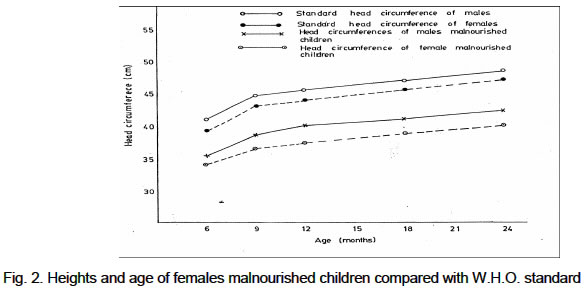
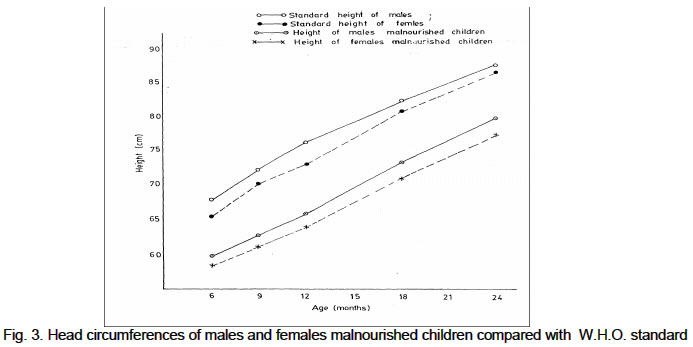
African Journal of Biomedical Research, Vol. 6, No. 3, Sept, 2003, pp. 123-127 PREVALENCE OF PROTEIN-ENERGY MALNUTRITION IN MAIDUGURI , NIGERIA*HAMIDU, J.L., *SALAMI H.A, **EKANEM A.U AND *HAMMAN, L. Departments of Human Physiology* and Anatomy**, College of Medical Sciences, University of Maiduguri . Maiduguri , Nigeria . Received: April 2001 Code Number: md03052 Nutritional disorders are common in young children in developing countries and constitute a major public health problem. In this study, the relationship between the dietary pattern of malnourished children on hospital admissions to the socio economic and educational status of the parents was investigated in one hundred and twenty (70 male and 50 female) children (6 – 24months) at the paediatric wards of the University of Maiduguri Teaching Hospital and the State Specialist Hospital, Maiduguri, Nigeria. Laboratory findings showed all the children had one or more form of infections associated with PEM. (41.6%) had gastro-enteritis 26 (21.7%) malaria, 18 (15%) pneumonia, 8 (6.6%) measles, 6 (5.0%) Pulmonary TB, and 12 (10%) had associated iron-deficiency anaemia. The results indicated the prevalence of marasmus was highest in the age group of 6 to 12 months in both sexes (34.3% and 36% for males and females, respectively while Kwashiorkor was highest among the children in the 13 to 18 months age group in both males and females. The results did not show any statistically significant sex difference in the prevalence of PEM. Educational and socio-economic status of parents (especially mothers) of the children bearing age showed that 80% of the mothers of the malnourished children had no formal education, 8.3% attended primary school, 1.7% had Islamic education only, while 10% had post-primary school education. None had higher education. The implications of these findings were discussed. Keywords: Protein-Energy Malnutrition, children, Maiduguri, Nigeria, Prevalence INTRODUCTION Nutritional disorders are common in young children in developing countries and constitute a major public health problem. The incidence rate varies from country to country, depending on the biological characteristics and socio-economic status of the population. The importance of adequate nutrition of infants has been recognised. Earlier studies on the aetiology of malnutrition showed evidence or inadequate protein, energy, vitamins and minerals. Dallman et al (1984) confirmed that inadequate iron intake lead to anaemia with low Packed Cell Volume (PCV) and Haemoglobin concentration. Watson and Petson (1984) earlier reported nutritional disorder as a major contributing factor predisposing malnourished children to infections and increased incidence and prolongation of diarrhoea and vomiting in infants. This is because the mucosal surfaces in these children are particularly susceptible to invasion by micro organisms, and decreased immune system within this age range. Protein Energy Malnutrition (PEN) is particularly serious in post-weaning and often associated with infections (Donald, 1991). The most common diseases associated with severe PEN are respiratory infection, diarrhoea and vomiting, with high morbidity. The report also suggested that PEN has lasting effect on growth and development of children, learning ability and social adjustment. The term PEN covers a whole range of deficiency states, from mild to severe and is defined as a range of pathological conditions arising from coincident lack in varying proportions of protein and calories, occurring most frequently in infants or young children. The clinical disorders present either as kwashiorkor (insufficient high quality proteins) or marasmus (deficiency of calories) or a mixture of the two; Marasmic- Kwashiorkor. Listemick (1985) reported that in developing countries, approximately 65% of children under the age of 5 years are malnourished and 50% of these children die as a result of PEM. In Nigeria, most of the data reported on PEM are from the southern part of the country. These data indicate PEM to be one of the major causes of child—death in Nigeria. This is because most families do not provide enough protein supplementation to their weaning children while carbohydrate is usually adequate. This study was therefore intended to investigate the relationship between the dietary pattern of malnourished children on hospital admissions to the socio economic and educational status of the parents in Maiduguri, Nigeria. MATERIALS AND METHODS Subjects One hundred and twenty (70 male and 50 female) children were studied at the paediatric wards of the University of Maiduguri Teaching Hospital and the State Specialist Hospital, Maiduguri for the State of the weaning Children in Borno State. The children were between the ages of 6 and 24 months. The investigation covered a period of 4 months during which all the cases of malnourished children admitted were recorded. The diagnosis of protein-energy malnutrition was based on the usual standard, i.e. mid-arm and head circumferences, skin folds, height and weight, modified on Wellcome's classification. Data on the education status of mother, occupation, family size, birth interval, feeding habit, age and immunization status of children were obtained through oral interview of mothers. Anthropometric Indices Mid-arm and head circumferences, height, and weight of malnourished children were measured according to the techniques described by Baker et al workers (1982). The mid-arm circumference was measured by placing the tape round the mid-arm. Head circumference was measured by placing the tape firmly over the glabella and Supra orbital ridges interiorly, then the tape wound round the head and measurement recorded. Heights were taken with child in supine position with the heels close together and arm by the side. The tip of the tape was placed 2cm above the ear, and straight to the heels. The height, weights, mid-arm and head circumference were compared with WHO Standards. Collection of Blood Samples The tip of the index finger was cleaned with spirit and dried in air. A finger prick was done to collect blood samples from all patients using a sterile lancet for each patient. The blood samples obtained were used for the various haematological analyses. The haematological examination were performed according to standard methods. Haematocrit was determined by the method described by Wakama (1984). The PCV of each sample was determined using a Hawskey micro-haematocrit centrifuge at 12,000 rpm for 5min. Heamoglobin (Hb) concentration was determined using Sahli's method. RESULT S A total of 120 malnourished children (age range: 6 - 24 months) were studied. The patients were on admission at the paediatric wards of the University of Maiduguri Teaching Hospital and the State Specialist Hospital, Maiduguri. The patients were classified into three groups, kwashiorkor, Marasmus, and Marasmic-Kwashiokor using Wellcome's classification criteria. This is shown in Table 1 according to age and sex. The results indicated the prevalence of marasmus was highest in the age group of 6 to 12 months in both sexes (34.3%) and 18 (36%) for males and females, respectively. Kwashiorkor was highest among the children in the 13 to 18 months age group in both males and females. Table 2 shows the prevalence of PEM in percentage by sex. The results did not show any statistically significant sex difference. Educational and socio-economic status of parents (especially mothers) of the children bearing age showed that mothers of 96 (80%) of the malnourished children had no formal education, 10 (8.3%) attended primary school, 2 (1.7%) had Islamic education only, and 12 (10%) had post-primary school education. None had higher education.The influence of socio-economic status of parents, the dietary pattern of the children was also investigated. The result is presented in Table 3. Immunization status of the affected children also showed that 56 (46%), 64 (53.3%) have been immunized only against either measles or small-pox. The Laboratory findings showed all the children had one or form of infections associated with PEM. (41.6%) had gastro-enteritis 26 (21.7%) malaria, 18 (15%) pneumonia, 8 (6.6%) measles, 6 (5.0%) Pulmonary TB, and 12 (10%) had associated iron-deficiency anaemia. The anthropometric measurements in both sexes are presented in figures 1, 2I and 3 and compared with W.H.O. standard. Table 1: Distribution of types of PEM by age group in both males and females
Table 2: Prevalence of PEM (%) by sex
Table 3: Dietary pattern of the 120 malnourished children
DISCUSSION The incidence of malnutrition in Borno State, Nigeria for the period of 4 months was investigated in this work. Only children between the ages of 6 to 24 month old were examined. Factors ranging from lack of maternal education to poor socio-economic statuses of the patients were identified. This is in agreement with the observations of Bithoney (1985). According to their reports it was clear that poverty might lead to malnutrition in a number of ways. The observation of a greater number of paediatric patients with marasmus compared with those of kwashiorkor and marasmic- kwashiorkor is in agreement with the report of Bithoney (1985) in the United States. However, Fatunde et al (1995), in Ibadan (Southern Nigeria) observed high incidence of Kwashiorkor. This could probably be due to low protein-diet containing food stuff in that region when compared with the Northern part. In the northern region of Nigeria, the diet is more of inadequate calorie intake rather than inadequacy of protein in the diet. Marasmus was also found to be more common among children of the ages between 6 and 12 months while kwashiorkor and marasmic-kwashiorkor were highest between the ages of 13 to 18 months and 19 to 24 months, respectively. Majority of the malnourished children were resident in high-density areas or the areas of the town where poor home facilities, poor environmental sanitation and low socio-economic status of the patients were identified as key factors. In addition most of the mothers, 46 (81.7%) had no formal education or attended only primary or Islamic schools. Some of the mothers married at very early age when, they were nutritionally deficient. Others were married into polygamist homes. Doyin (1990) has observed strong association between family size and malnutrition. Birth interval might not have been associated with malnutrition since the birth intervals being practiced here ranged from 2 to 3 years. This was similarly reported by Doyin et al , (1990). Most mothers breast-fed for 12-24 month, and in cases the breast milk was not exclusive as pap and other carbohydrate introduced early (before 6 months). This contributed to the incidence rate of PEM as additional food might not have been hygienically handled. Therefore sporadic episode of diarrhoea and vomiting were common before this age. Prior to the presentation, some of the mothers had discontinued milk feeding. It was evident therefore, that the onset of the disease (PEM) was closely related to the age and practice of weaning. The study, also observed inadequate utilization of available immunization services. Only 28 (46.7%) of the malnourished children had received the full course of the triple vaccines while 32 (53.3%) of the children had been immunized against either measles or small-pox. However, this under-utilization is not peculiar to Nigeria. It is a phenomenon in most developing Countries (Fatunde, 1995). The predominant factor observed here was lack of education, ignorance and cultural beliefs. REFERENCES
© Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md03052f3.jpg] [md03052f2.jpg] [md03052f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}