 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 7, No. 3, Sept, 2004, pp. 119-123 Full Length Research Article ACUTE OSTEOMYELITIS IN CHILDREN IN IBADAN, NIGERIA. IS SURGICAL DECOMPRESSION NECESSARY? S.O. OGUNLADE[*], A.B. OMOLOLU AND T.O. ALONGE Department of Orthopaedic and Trauma,
University College Hospital, Ibadan. Nigeria. Received: February 2004 Code Number: md04026 A total of 17 Children with acute osteomyelitis presenting to division of orthopaedics and trauma surgery is presented. The male:female ratio is 1:1:3, mean age of 6.12 years. The median time of illness before presentation is 8 days. The Tibia bone is the most common site of infection (52.9%) while multifocal infection occurs in 35.3% of the patient. Staphylococcus aureus is the most common isolate (47.1%) while Salmonella typhi occurred in 23.5% of the patients, all with sickle cell disease. There was positive bone aspirate in all the patients while all patient had surgical intervention with sequential intravenous - oral antibiotic therapy with an excellent outcome in 94.1%. Surgical intervention appears to be essential to cure of acute osteomyelitis in addition to antibiotic use. INTRODUCTION Acute osteomyelitis (AO) most often involves rapidly dividing bones as illustrated by the striking age distribution of the disease, over 85% of the cases reported in large series have occurred in children (Shandling 1960). Acute osteomyelitis in children begins with a "cellulitic phase' in which no obvious pus is formed, if this infection is unchecked, it leads to formation of abscess (Green 1994). AO is an inflammation of bone caused by bacteria that reach the bone via the hematogenous route. AO always means an emergency with high diagnosis and therapeutic demands. The goal of treatment is to prevent complications such as concomitant septic arthritis with its high risk of persistent joint damage, growth disturbance, or chronic osteomyelitis. The treatment of AO includes symptomatic measures, bed rest, operatives intervention if necessary with drainage of pus and debriment of any necrotic material together with antibiotic treatment in sufficient concentration and for sufficient duration (Lamprecht 1997). The purpose of this study was to prospectively evaluate the occurrence, clinical feature, infecting organisms, stage of presentation (i.e. cellutic or abscess formation stages) and outcome of treatment. MATERIAL AND METHODS A prospective clinical study was carried out between March and July 2001 on all children referred to the Orthopaedic and Trauma Division, Department of Surgery, UniversityCollegeHospital, Ibadan with suspected A.O. A presumptive diagnosis of AO was made on the basis of fever, bone pain, decreased limb use and tenderness of the affected bone (Karwowska 1998). A pre-designed data sheet was used to collate symptoms and signs, history of fall, investigation result, treatment, and outcome. The investigations are full blood count, westergreen erythrocyte sedimentation rate, haemoglobin electrophoresis, bone aspirate for microscopy, culture and sensitivity, and x-ray of the involved bone. Empirical intravenous cefuroxime was commenced after blood samples and bone aspirate were taken and adjusted if need be based on bacteriological culture results. Intravenous antibiotics are changed to oral, once clinical response is seen and temperature has remained settled for 48 hours. Anti-microbial chemotherapy was given for 6 weeks. The diseased limb was also splinted. Bone aspiration was performed on every patient using wide bore needle over area of maximal tenderness. Operative management consisting of drainage of abscess, debridement of any necrotic material with bone drilling if pus or seropurulent fluid was aspirated. A total of Seventeen (17) children with acute Osteomyelitis were recruited into the study. Statistical Analysis The Statistical Package EPI-INFO version 6.02 was used for data entry, editing and cleaning. The necessary data check was introduced into the entry module of the package to ensure the reliability and validity of the data entered. The data file was subsequently converted to SPSS for statistical analysis. In cases where the assumption of normality and homoscedascity were not satisfied, the Mann Whitney U test, a non-parametric test was used t o compare any two groups. All statistical tests were two tailed and were carried out at 5% level of statistical significance. RESULT Demographic Distribution of the children Table 1 shows the distribution of the children's demographic characteristics. The mean age of the children was 6.12 years and a standard deviation of 3.17 years. The majority of the children were aged 6years and above (52.9%). The female children dominated the study (58.8%) and most of the children were living with their parents (88.2%). Only 23.5% of the patients had history of fall. Presentation Time. Statistics of the patients' duration of illness by patient's sex and history of fall was shown in table 2. The average duration of illness before presentation was 9.65 days, standard deviation of 5.11 days and a median time of 8 days. The earliest presentation was in 3 days while the latest was 21 days after the illness. The female children had a slightly higher duration of illness before presentation (mean = 10.00, s.d. = 5.87) compared to the male with average presentation time of 9.14+4.18 but the mean difference was not statistically significant (P>0.05). Similarly, children with history of fall had a lower duration of illness before presentation (mean = 6.5days, s.d. = 3.7days and median of 5 days) compared to their counterparts with no history of fall with average presentation time of 10.62+5.21 and median time of 9days, the difference was also not statistically significant. Table 1: Summary Statistics and Frequency Distribution of Patients' Characteristics
Symptoms and Signs on Presentation Figure 1 shows the distribution of the symptoms associated with the illness on presentation. All the children had fever and bone tenderness at presentation, a high majority of the patients also had decrease limb use with bone pain and swelling (94.1%). A small proportion of the patients had Headache (17.6%), vomiting (11.8%), joint pain (29.4%). Table 2: Summary Statistics of Duration of illness before presentation by Patient's characteristics
Table 3: Distribution of Investigation done and Treatment Administered
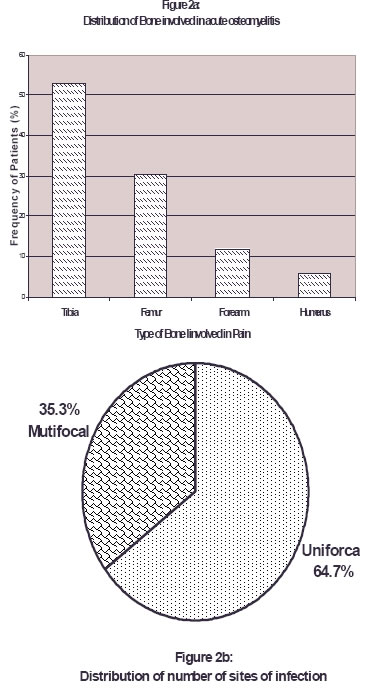
The distribution of bone involved and the number of site are shown in Figure 2. The most common site is Tibia bone (52.9%), while Femur accounted for 30.4% forearm bones (11.8%), and humerus (5.9%). Most of the children (64.7%) had single bone involvement (unifocal) while remaining 35.35 has more than one bone involvement (multifocal) (Fig. 2b). Investigation and Treatment Administered Table 3 shows the distribution of the Investigation and treatment administered. The x-ray of the bone was done for all the patients. There was no evidence of acute osteomyelitis i.e. no bone lesion in more than half of the children (52.9%), the x-ray revealed features of acute ostemyelitis for the remaining proportion of the children (47.1%).The genotype shows that 43.8% were HbA patients, 37.5% were HBS and 18.8% were HBAS. All the patients had purulent bone aspirate, the culture grew staphylococcus aureus in 47.1%, Salmonella Typhi in 23.5% and Klebsiella species in 17.6%. Less than 10% of the patient had Escherichia Coli (5.9%) there was no growth and only one child reported no growth. All the children were given antibiotics. Bone decompression surgery was also done for all the patients. A high proportion of children (94.1%) had splint/POP applied. Table 4: Distribution of Patients' Symptomatic Response to Treatment
* Within 2 weeks of treatment Symptomatic Response to Treatment Table 4 shows the patients' symptomatic response to treatment at two weeks of treatment. The majority of the patients (82.4%) had pain reduced after receiving the treatment. The temperature of the majority (88.2%) was also normal while the body swelling has subsided for most of the patients (76.5%). More than half of the patients (58.8%) had no complication at the end of treatment. The most reported complication was septicaemia reported by 17.6% of the patients and only 1 patient reported each of lung complication, reactive effusion, pathological fracture and progression to chronic osteomyelitis. All the patients had their illness resolved at the end of the treatment except the patient with chronic osteomyelitis. DISCUSSIONAcute Osteomyelitis is a common disease in Childhood. If treated early, conservative management is possible (Spindler 1998). In developed countries, early presentation of patients coupled with the availability of imaging techniques like ultrasound, bone scan and magnetic resonance enhance early diagnosis (Kaiser 1998). The median duration of complaints prior to presentation in our study was 8 days, which indicate that our patients do not present early when compared with median duration of complaint prior to admission of 4 days in a retrospective study of acute Osteomyelitis in children in Norway (Dahl 1998). In our study, there was male: female ratio of 1:1.3 which is similar to findings in Norway (Dahl 1998). However in this study the mean age is 6.12 years with no child below 2 years. This may be due to small number of patients in the study, and the age of the children could account for no single complication of septic arthritis in the study, though there was a single case of reactive effusion, as onset of acute osteomyelitis in early infancy is one of the risk factor for unfavourable course of the disease. In discussing the aetiology of the disease, trauma has been implicated by some authors. As formation of haematoma in the metaphysics following trauma could enhance bacterial infection in the borne (Green 1994), in our study there was history of preceding fall and trauma in 23.5% of patient. The most common presenting symptoms in study are fever and decrease use of the limb while the most common signs are bone tenderness and swelling. This agrees with findings of other authors (Karwowska 1998, Savvidis 1997). The lower extremities, were the most common region affected with the Tibia bone being the most common site of infection which is similar to findings in other series (Dahl 1988, Trobs 1999, Sadat 1998). The infection was multifocal in 35.3% of our study which is similar to 33.3% in a study of sickle cell patients with acute osteomyelitis by Epps et al. (Epps 1991). All the six patients in our study with multifocal infection are sickle cell patients (hemoglobin S). There was no radiological evidence of acute osteomyelitis of the bone in 52.9% of the patients, this is due to the fact that bone changes takes up to 14 days before it becomes visible radiologically (Green 1994). All our patients had positive bone aspirate which are either purulent or seropurulent. This is due to the late presentation of acute osteomyelitis. The bone aspirate showed positive culture in 94.1% which supports the view that bone aspirate still remains the best method of isolating the causative organism in acute osteomyelitis (Karwowska 1998). Staphyloccus aureus was the most common organism isolated (47.1%) in our study, followed by Salmonella typhi in 23.5%, the Salmonella typhi organisms were isolated from the children, with sickle cell disease (Hemoglobin S). This study agrees with other authors who confirmed that Staphylococcus aureus was the most common organism isolated in acute osteomyelitis while Salmonella typhiorganism is a common isolate in acute osteomyelitis in children with sickle cell disease (Lamprecht 1997, Karwowska 1998, Dahl 1998, Sadat Ali 1998). Bone aspirate to decompress the bone also help to relieve pain in acute osteomyelitis (Booz 1990). All the children had surgical intervention which include incision and drainage of the abscess, bone decompression with excision of all necrotic tissue in addiction to intravenous antibiotics. The surgical intervention is important as it prevents progression of the infection to chronic osteomyelitis (Sadat Ali 1998). Surgical intervention is supported in children with acute osteomyelitis presenting late and in acute osteomyelitis in sickle cell patient (Lamprecht 1997, Sadat Ali 1998). Sequential intravenous - oral antibiotics therapy has been shown to have an excellent outcome and the median duration of intravenous antibiotic therapy was 11 days in study that monitored the erythrocyte sedimentation rate and C - reactive protein as an indices of response to therapy (Karwowska 1998). This compares with our study in which we found that the Temperature became normal and was maintained for 48 hours and beyond when the median duration of intravenous antibiotic was 14 days. We suggest that the use of Patient Temperature to guide duration of intravenous antibiotics in acute osteomyelitis in our environment is recommended as it is noninvasive with no additional laboratory cost. Oral antibiotics was administered to make a total of six weeks on antibiotic. The outcome was satisfactory in 94.1% of children with complete resolution of the infection, only one patient progressed to chronic osteomyelitis. In conclusion, acute osteomyelitis in children do present late to hospital in our environment. Surgical de-compression together with sequential intravenous - oral antibiotic usually gives an excellent outcome. REFERENCES
© 2004 - Ibadan Biomedical Communications Group
The following images related to this document are available:Photo images[md04026f2.jpg] [md04026f1.gif] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}