 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 7, No. 3, Sept, 2004, pp. 149-151 Short communication GLYCEMIC CONTROL AND PAIN THRESHOLD IN ALLOXAN DIABETIC RATS IBIRONKE. G. F[*].; SABA .O J. and OLOPADE F.O Dept
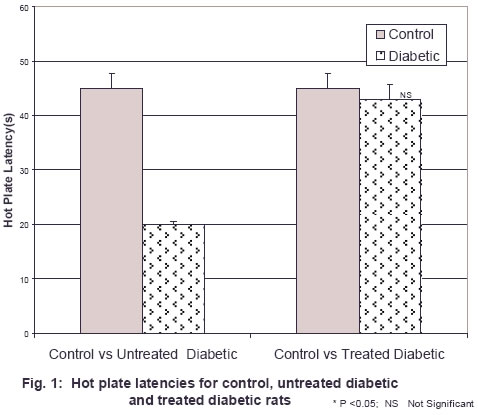
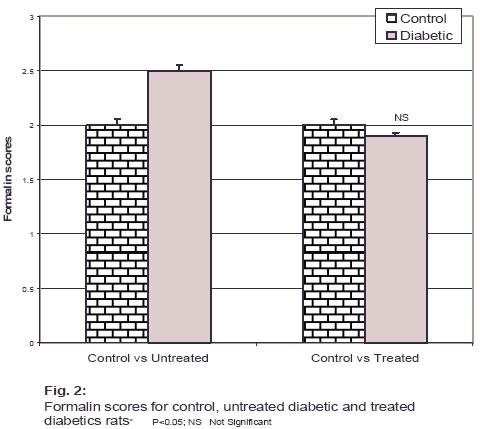
of Physiology, College of Medicine, University of Ibadan Received: December 2003 Code Number: md04032 Insulin dependent diabetes mellitus (IDDM) is associated with several complications including painful diabetic neuropathy. Previous animal and human studies have indicated that nociceptive thresholds are decreased by acute hyperglycemia. Furthermore, it has been suggested that glucose may be an important mediating factor in these painful symptoms. In the present study, pain threshold was assessed via the hot plate and formalin tests in control, untreated diabetic and treated diabetic rats. Hyperglycemia induced by 40mg/kg alloxan significantly lowered the pain threshold as revealed by a decrease in the hot plate latency and increased mean formalin score. In contrast, the hot plate latency was significantly increased and the formalin score significantly reduced in the diabetic rats following normalization of blood glucose level. These results suggest that hyperglycemic states contribute to a decrease in pain threshold in the alloxan diabetic rats. INTRODUCTION Pain is a common manifestation of diabetic neuropathy (Brown And Asbury, 1984). However, the aetiology of the neuropathic pain is still not determined. Diabetic neuropathic pain may originate from regenerating axon sprouts (Asbury and Fields, 1984, Buchiel et al, 1985). However, diabetic subjects with such neural changes may not experience neuropathic pain (Said et al, 1983). Metabolic factors and stringent regulation of blood glucose levels may also contribute to the development or amelioration of diabetic neuropathic pain (Samanta and Burden, 1985). Thus painful diabetic neuropathy may be the result of interplay between peripheral neuropathy and the metabolic changes in the central nervous system caused by the diabetic state. Experimental evidence relating to the effects of diabetes on pain perception is contradictory. Chan et al, (1986) reported a higher level of pain threshold streptozotocin diabetic (STZ-D) male rats via the hot plate device, likewise Levine et al, (1982), demonstrated prolonged tail flick latencies to radiant heat stimulus in diabetic mice. In contrast to these findings, Forman et al, (1986), reported a significant reduction in the pain threshold of STZ-D male rats via the hot plate device. Morley et al. (1984) also demonstrated a lowered pain threshold in humans rendered acutely diabetic by glucose injection. Raz and co-workers (1988) reported that neither acute nor chronic states of hyperglycemia altered pain thresholds of laboratory animals as measured by the hot plate device. This study was therefore undertaken to resolve aspects of the conflicting evidence relating to the effects of hyperglycemia on pain perception. MATERIALS AND METHODS Animals: Eighteen adult male Wistar rats (200-250g) purchased from the pre-clinical animal house of the College of Medicine, University of Ibadan, Nigeria were divided into three groups: control, untreated diabetic and treated diabetic. The animals were housed in-groups of eight in plastic cages at room temperature with a 12-h light/dark cycle. Standard food pellets and water were available ad libitum. Pain rating was carried out using the hot plate and formalin tests. Hot Plate Test: The hot plate latency was measured using a modification of the original method of Eddy and Leimbach (1953). Briefly, the modified apparatus consists of an electric cooking plate (Saiso, Japan) with a 1500 Watts stainless steel heating element connected to a thermostat (0-400°C), a thermocouple connects the thermostat to a chrome plated drip pan. The thermocouple together with the thermostat control the temperature of the hot plate within the desired range once set. Pain sensitivity was evaluated by the response latency for paw licking on the hot place. In order to avoid tissue damage, the maximum time the animal could spend on the hot plate was pegged at 60 seconds. Response latencies were measured at 15 minutes intervals and the average of the results was taken. Formalin Test: The rats were acclimatized to the experimental arena for 15 minutes and anaesthetized with 5% halothane (Yamamoto and Yaksh, 1991). Formalin (50mL, 0.25- 5%) was injected sub-cutaneously (sc) into the large lateral foot pad on the plantar surface of the left hind paw. The rats were placed in a transparent rectangular plastic box with the top opened for an unobstructed view of the response to formalin injection which was measured using the weighted scores method (Coderre et al, 1993) The pain rating was carried out in the control, untreated diabetic group after alloxan injection and in the treated diabetic group after insulin administration. In all experiments, the control animals had 10mls/kg normal saline sc. Induction of Diabetes: Following a 48h fast, 8 rats received intraperitoneal (i.p) injection of alloxan (40mg/kg). Within 48hrs after alloxan administration, blood glucose concentrations were measured via tail clip sampling. Briefly the tip of the tail (approximately 2mm) was clipped off using a sterile blade and 1-2 drops of blood from the cut surface were used for measurement of blood glucose concentration using the glucose oxidase method. Animals with blood glucose concentrations less than 250mg/dl were excluded from the study. Beginning from the third day after alloxan treatment, diabetic rats received daily injections of regular insulin (2 units/animal, s.c) between 17.00 and 19.00h for a two week period. Statistical analysis: All data are presented as means ± SEM. Significant differences in hot plate latencies and formalin scores were determined by students’ t-test. A value of p<0.05 was regarded as significant. RESULTS The hot plate latencies of hyperglycemic alloxan – diabetic rats (mean blood glucose level > 250mg/dl) were significantly less (20.0±0.59s vs 45.0± 2.80s, P<0.05,n=8) than those of control non diabetic rats. (fig 1) However, the mean formalin scores in alloxan diabetic rats were significantly higher (2.5±0.07 vs 2.0 ± 0.05, P<0.05, n=8) than those in control, non – diabetic rats (fig2). The results are consistent with increased pain sensitivity in the diabetic state. When these same diabetic rats were tested, when the blood glucose levels were in the euglycemic range (75.0 ± 17.1 mg/d1) after insulin administration, the hot plate latencies and formalin scores were similar to those of control rats (45.0±2.80s vs 43.0 ± 2.65 and 2.0±0.05 vs 1.9±0.03 respectively) figs 1 and 2. DISCUSSION Our results indicated that in the male rat, an acute state of hyperglycemia in the form of an intraperitoneal injection of alloxan lowered the pain threshold as determined by the hot plate and formalin tests. Diabetic animals clearly demonstrated an increased sensitivity to pain when hyperglycemic. Our findings agreed with previous studies which suggested that acute hyperglycemia may increase pain sensitivity (Morey et al, 1984; forman et al 1986), but contrast some other reports (Levine et al, 1982; Chan et al 1986). There may be several explanations for these inconsistent findings, for example several methods have been used to access pain thresholds and results of pain experiments have been shown to be test dependent, for instance in our own study we used the hot plate and formalin tests while Levine et al (1982) employed the fail flick test. While the fail flick test measures spinal reflexes as a result of heat application, the hot plate test measures supraspinally organized responses to heat. These differences may contribute to variations in the observed result. Apart from the type of test employed, the choice of animals might also influence the results. While Levine et al (1982) used mice, we used albino rats in own study. The exact mechanism by which hyperglycemia increases pain sensitivity is not known, but several suggestion have been made, for example the decreased pain thresholds have been attributed to hyperisulinemia induced by hyperglycemia. Insulin is known to stimulate the Na+/K + ATPase in cell membranes (Clausen and Kohn, 1997) and this could change nerve function directly by stimulation of ATPase on nerve issue or indirectly by universal changes in ion distribution induced. Another suggested mechanism is that a hyperglycemic state induces overproduction of intracellular sorbitol in tissues (Malone and Lowittts, 1992), which increases intracellular osmotic pressure that modulates several ionic conductances and increased Ca2+ -influx and membrane depolarization (Viana et a,, 2001), both of which are known to increase pain sensitivity. Also contributing to decreased pain threshold in the hyperglycemic state is the level of exogenous opiod peptides (b endorphins). It has been established (Basbaum and Field, 1984) that increase in b endorphin levels in the cerebrospinal fluids ameliorates pain perception. Forman et al, (1986) noted that plasma pituitary and hypothalamic levels of the endogenous opiod peptides were reduced in female rats eight weeks following the induction diabetes using streptozotocin. These reductions in the b endorphin levels were related to the hyperalgesia observed in the streptozotocin diabetic rats. While these results are extremely suggestive, no strong conclusions may be drawn at this point until studies are carried out to determine the exact mechanism of lowered pain threshold in the diabetic state. In summary, the present findings support the idea that hyperglycemia does contribute to a state of hyperalgesia in alloxan- diabetic rats. These results may have important clinical implications as well. If increased blood glucose levels are responsible in part for the neuropathic pain in diabetic subjects, it is suggested that this knowledge could be used to guide the treatment and prevention of painful diabetic neuropathy in human subjects. REFERENCES
© 2004 - Ibadan Biomedical Communications Group
The following images related to this document are available:Photo images[md04032f1.jpg] [md04032f2.jpg] |
| |||||||||

{kind=link}
{kind=link}