 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 8, No. 1, 2005, pp.15-19 Full Length Research ArticlePrevalence of Hypertension in a University Community in South West Nigeria *ERHUN, W.O., OLAYIWOLA, G., AGBANI, E.O AND OMOTOSO, N.S. Department of Clinical Pharmacy and Pharmacy Administration, Obafemi Awolowo
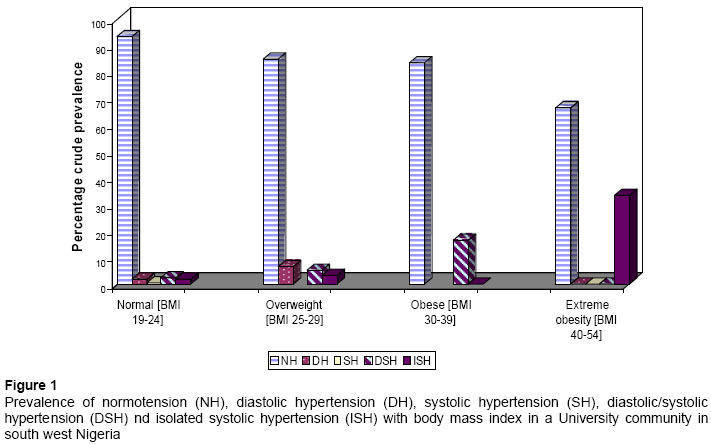
University, Ile-Ife, Nigeria. Received: July, 2004 Code Number: md05002 Abstract A worksite study of hypertension prevalence was carried out in a university community in Southwestern Nigeria. Overall crude prevalence was 21% in the respondent population. About 16% of these were already on treatment with medicines. The study established no significant (p>0.05) relationship between coffee consumption and hypertension. Prevalence was 32% in subjects with over 3 children, while among subjects with eye problem, diabetics and those who took local kola nuts and it was 18.6%, 1.9% and 7.4%, respectively. There is need for increased awareness of the disease and other cardiovascular risk factors within the populace and to encourage the possession or provision of self-measurement blood pressure devices. Keywords:Hypertension, Prevalence, University population, Nigeria INTRODUCTION Hypertension is a common health problem in developed countries and a major risk factor for cardiovascular diseases (CVD) (Castelli, 1984). Its prevalence is probably on the increase in developing countries where adoption of western lifestyles and the stress of urbanization both of which are expected to increase the morbidity associated with unhealthy lifestyles are not on the decline. (Castelli, 1984). Genetic and environmental factors are reported to play a key role in hypertension, 90% of which are better classified as idiopathic. High blood pressure in adults has a high impact on the economy and on the quality of life of individuals with important implications for resource expenditures. A number of studies revealing the prevalence of hypertension in populations of West African origin have been reported. (Cooper et al, 1997; Gwatkin et al, 1999; Cappuccio et al, 1997). Not much has been done to determine the magnitude and epidemiological characteristics of this disease in Nigeria and to particularly assess other cardiovascular risk factors within the population. Effective interventions will require the assessment of the socio-economic magnitude and extent of the burden of hypertension in the working class. To this end, a cross-sectional survey was carried out to estimate the currentprevalence and distribution of hypertension and to determine thestatus of hypertension awareness and control among a working population. The study was conducted in a federal University community in southwestern Nigeria. MATERIALS AND METHODS The study population was composed of adults aged 21 years and above whom at the time of the study was either academic or non-academic staffs in the federal university in South Western Nigeria, which was our study site. The consent of 1000 subjects drawn from all faculties and service units of the university was obtained of a target population of 5000 after explaining the purpose of the study. They were interviewed; a structured questionnaire was used to collect basic socioeconomic and demographic data and to identify history of hypertension. For those with a positive history of hypertension, further information was obtained on the duration of the disease, source of diagnosis (if not newly diagnosed) and whether treatment was being received at the time of the survey. Hypertension was defined as a mean systolic blood pressure (SBP) >140 mmHg, and/or mean diastolic blood pressure (DBP) > 90 mmHg, according to the report of the Joint National committee on detection, evaluation and treatment of high blood pressure (JNC-V, 1993) and/or by self-reports of a medical diagnosis of hypertension or by current treatment for hypertension with prescription medication. Isolated systolic hypertension was defined as SBP of 140 mmHg or more but with a DBP < 90 mmHg, while isolated diastolic hypertension was defined as a DBP of 90 mmHg or more and SBP < 140 mmHg according to (JNC-VI, 1997) and (WHO/ISH, 1999). The subjects were seated for at least five minutes, an appropriate sphygmomanometer cuff was applied to the right arm, and blood pressure was measured using a standard mercury sphygmomanometer. The first measurement was taken after a 10-minute rest in a sitting position and was followed by another at the end of the interview. Body weight was measured with subjects bare-footed and expressed in kilograms (kg) to the nearest 0.1kg and the corresponding height expressed to the nearest centimeters. The body mass index (BMI) (kg/m2 ) was used to define obesity (BMI > 30 kg/m2 ) and overweight (BMI > 25 kg/m2 ) Statistical analysis was done using the SPSS version 10.0 software program for frequency distribution and cross tabulations. Test for statistical significance were done by the chi-square test for categorical data and the Student t-test for quantitative data using bivariate correlation to determine the significance of between factor changes. RESULTS The respondent population was 1000; of these 66.5%, 33.5%, 13.3% and 86.7% were male, female, single and married, respectively. Crude prevalence of hypertension in the respondent population was 21%. Prevalence was 23.3% in males and 16.4% in females. A proportion of the total population (18.3%) was on prescription drugs and at least, an anti-hypertensive was present in 16% of the cases. About 15% of the hypertensive population had been previously diagnosed with the disease but only 4.8% of these had controlled BP; 6.4% of the respondent population was newly diagnosed with hypertension. The survey established a correlation (p< 0.05) between hypertension and the number of children in the married hypertensive population with 18.5% of subjects having 4 -7 children presenting with high blood pressures; 6.5% of these cases being isolated systolic hypertension. Crude prevalence was 32% and 7%, in subjects with children = 4 and children = 3 respectively; a direct relationship exist between number of children-respondent age and number of children-respondent monthly salary at 1% confidence interval. Figure 1 shows the prevalence of normal blood pressure, diastolic hypertension, systolic hypertension, diastolic/systolic hypertension and isolated systolic hypertension with body mass index in the total respondent population. Precisely 18.6%, 7.4%, and 1.9% of subjects with eye problem, who take kola nuts and diabetics, respectively, were hypertensive. Prevalence increased significantly with age (p<0.01) and Body Mass Index (BMI) (p<0.05); 2.4, 4.3, 7.4 and 29.3% of subjects within the age groups 21-30, 31-40, 42-50 and 51-60, respectively, were hypertensive. Direct associations were identified between BMI, alcohol (daily >14 g intake of ethanol determined from %v/v alcohol content of product and total volume consumed) and kolanut (at least one in two days) consumption in men and isolated systolic hypertension. The prevalence of isolated systolic hypertension (ISH) increased with age across the groups; this was 1.4% in age group 21-30 and 12.2% in age group 51-60 with the middle age of 31-40 revealing 0% crude prevalence for ISH in the study population. Similarly the prevalence of diastolic/systolic hypertension (DSH) in the respondent population was 2.4, 1.4, 2.5 and 9.8% in age groups 21-30, 31-40, 41-50 and 51-60, respectively. Table I shows the prevalence of hypertension with selected risk factors; 62% of the total population lived with at least 2 risk factors. A proportion of the diabetic population (20%) suffered from isolated systolic hypertension, 88.9% of the population presenting with eye problems were normotensive with the rest presenting mainly with diastolic/systolic hypertension. Only 15% of the population complaining of sleep problems were hypertensive; The study established no significant (p>0.05) relationship between coffee consumption and/or the smoking of 2-5 sticks of cigarettes/day and hypertension. DISCUSSION The level of the respondents awareness of hypertension calls for enlightenments programs that will emphasize the important role of individuals in the prevention and management of hypertension and other cardiovascular risk factors as well as measures to encourage routine blood pressure checks. Of the total 210 cases of hypertension, 6.4% were newly diagnosed with hypertension during the survey. The majority of the new cases (85.0%) were mild, (with DBP <100 mmHg), within ages 25-40 and might need only non-aggressive treatment and follow-up. A sizeable portion (14.6%) of the study population were cases of reported positive history of hypertension treatment as at survey time, of these however, only 4.8% had controlled BP; thus indicating a poor BP control level in this subgroup. Patient non-compliance with treatment is common in hypertensive therapy and could be a factor in these; however physician behavior has been implicated by many studies as a major cause of poor hypertension control (Hyman and Pavlik, 2002). The authors hold that proper education through programs directed at worksite will heighten sense of responsibility for the success of management strategies in hypertensive patients. The basis for the observed increase in hypertension prevalence with increasing number of children is not well known, however, considering the socio-economic challenges facing families in Nigeria, there are indications that higher number of children will increase stress though the respondent monthly salary appear to increase with the number of children. Psychological stress has been related to higher blood pressure and unfavorable cardiovascular profile (Fauvel et al, 2001), and there is moderate support for psychological factors as predictors of hypertension development, with the strongest support for anger, anxiety, and depression variables. Pooled effects for these factors are of sufficient magnitude to suggest potential clinical as well as statistical relevance (Rutledge and Hogan, 2002). though individuals have strategies for stress management, they are often complex so that a multi-dimension stress measurement strategy is needed for a detailed representative study. Our survey shows the prevalence of hypertension to be in the order of diastolic/systolic hypertension > diastolic hypertension > isolated systolic hypertension > systolic hypertension. The prevalence of isolated systolic hypertension (ISH) and diastolic/systolic hypertension increased with age across the groups, age group 31-40 showing the least prevalence for both types; the rise in systolic blood pressure and the increasing risk of isolated systolic hypertension with advancing age have been attributed, in part, to increased peripheral vascular resistance. Available evidence also suggests that at any given level of arterial pressure, overweight patients with hypertension have a higher cardiac output and a lower total peripheral vascular resistance than lean patients. The lower peripheral resistance associated with overweight patients may attenuate the rise in systolic blood pressure and modify the prevalence of isolated systolic hypertension with age (David et al, 2000). Reports from cross sectional, longitudinal, and randomised controlled trials show that isolated systolic hypertension constitutes a substantial cardiovascular risk. (Staessen et al, 1997). It however remains under diagnosed and rarely treated (Coppola et al, 1997) even though benefits of treatment have been established. (Staessen et al, 1997). Perhaps incorporating mandatory blood pressures check up at worksites as workers advance in age into National ‘working’ policy will further make for adequate monitoring and reveal points for intervention. Figure 1 shows the positive relationship that exist between BMI scores indicating overweight, obese, extreme obesity and hypertension; the result show that 16.7% and 33.3% of the obese and extremely obese, have diastolic/systolic hypertension and isolated systolic hypertension, respectively. BMI is one of the most accurate ways to determine when extra body weight translate into health risks. The higher the BMI, the greater the risk of developing health problems. Cardiovascular disease and high blood pressure have been linked with overweight. Reports that SBP and DBP are found to increase linearly over BMI range have been made. (Doll et al, 2002). Obesity; now recognized as an independent risk factor for cardiovascular disease is closely associated with hypertension (Wofford et al, 2002). The result emphasizes the need for some lifestyle modifications in the affected respondent population. Body weight reduction via dietary interventions and calorie restriction being a practical step to reduce BP in the overweight, obese and extremely obese hypertensive population; less alcohol consumption, salt restriction, potassium and calcium supplementation can all enhance the process of lowering BP (Cutler et al, 1990; National work group, 1993), Diet rich in plant fibres either alone or with a low fat, low sodium could lower BP by about 5 mm Hg in hypertensives (Chhabra et al, 2001). The survey shows that over 10% of the population taking kola nuts (at least one in two days) and or alcohol (daily consumption of >14 g ethanol) are hypertensive. This is expected as caffeine, a major chemical constituent of kola nuts (Evans, 2002) enhances BP increase. Alcohol has been reported to produce similar effect. (Mathews, 1976). Caffeine has significant hemodynamic and humoral effects that persist for many hours during the activities of everyday life. It may exaggerate sympathetic adrenal-medullary responses to the stressful events of normal daily life. Repeated daily blood pressure elevations and increases in stress reactivity caused by caffeine consumption could contribute to an increased risk of coronary heart disease in the adult population (Lane, 2002). The study identifies caffeine as a significant cause factor of hypertension in the subjects, but consumption of coffee drinks (which may contain a large amount of caffeine) showed no significant correlation with hypertension in the study population. A possible explanation is the total amount consumed and perhaps the availability and preference that the subjects show for decaffeinated coffee drinks. Studies have shown that over many years of follow-up, coffee drinking is associated with small increases in blood pressure, but appears to play a small role in the development of hypertension (Jee et al, 1999; Klag et al, 2003). Most working populations in Nigeria share a number of variables with the respondent population of this study; factors like salary structure, socio-economic upheavals, number of children, alcohol consumption, working hours, and multi ethnicity being common. The authors thus expect similar results from related studies in other working populations in Nigeria. It is expected that hypertensive subjects who possess a self-measurement blood pressure device would have a better knowledge of their BP and this will impact positively on treatment seeking behavior and compliance; where this cannot be afforded by the individual worker, employers need be educated to provide the device for the general use of their workers at worksites. There is need for increased awareness of the disease within the populace and to encourage the possession or provision of self-measurement blood pressure devices. Orientation measures to stimulate participation in long-term cohort studies that aims at defining the epidemiology of hypertension within the Nigerian population are also vital. REFERENCES
The following images related to this document are available:Photo images[md05002f1.jpg] [md05002t1.jpg] |
| |||||||||

{kind=link}
{kind=link}