 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 8, No. 1, 2005, pp.25-29 Full Length Research ArticleMalaria Prevention: Knowledge, Attitude And Practice In A Southwestern Nigerian Community. ERHUN W.O1*, AGBANI E.O2 AND ADESANYA S.O1 Department of Clinical Pharmacy and Pharmacy Administration, ObafemiAwolowoUniversity,
Ile-Ife, Nigeria. Received: July, 2004
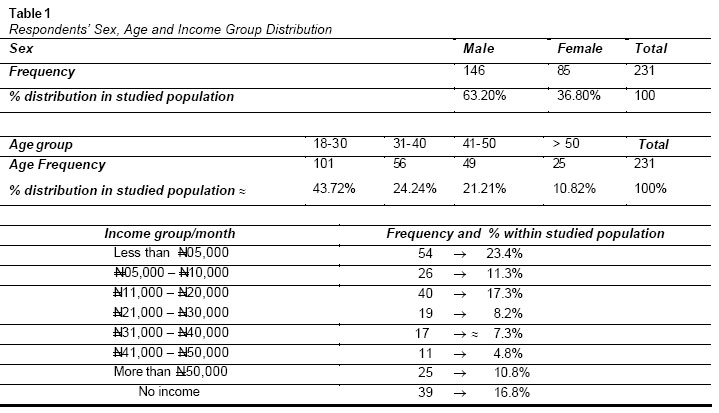
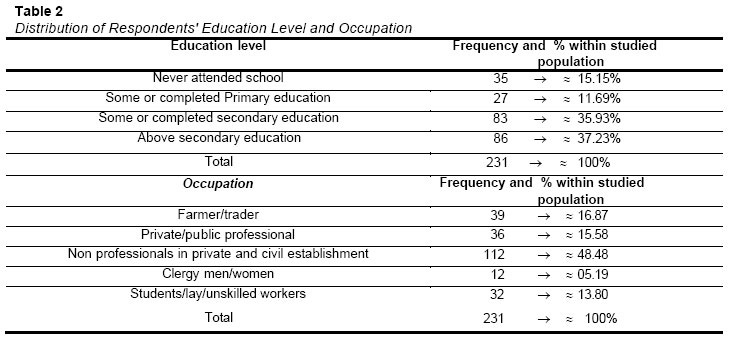
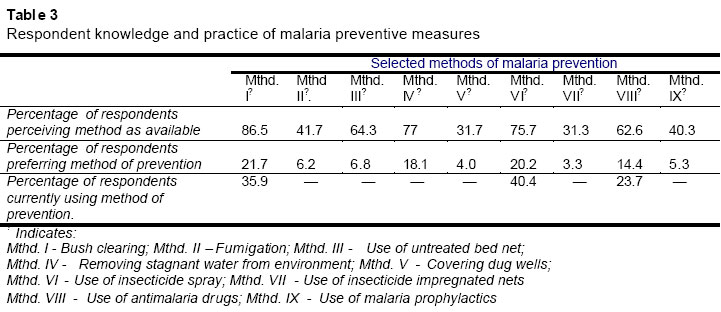
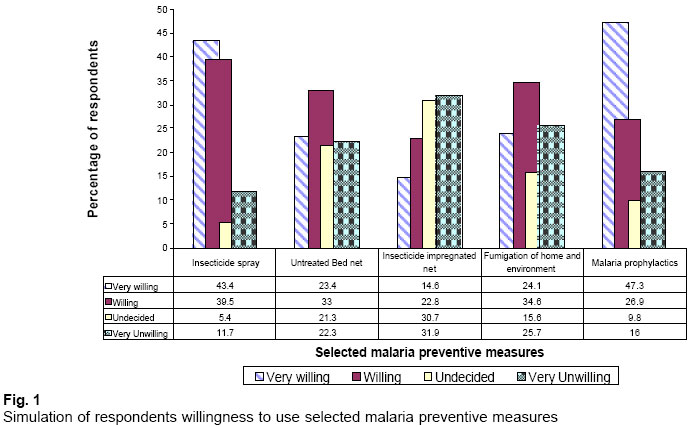
Code Number: md05004 Abstract Assessing and analyzing local malaria problems are a prerequisite for successful control interventions. We sought to assess the knowledge of the symptoms of malaria, attitude towards preventive measures as well as treatment seeking behaviors among members of the Ile-Ife community in southwestern Nigeria.A cross sectional study was carried out using a questionnaire, which was self or researcher administered to community members of semi-urban Ile-Ife.Analysis of “what respondents will do first” during malaria attack showed that 35.5%, 0.9% and 13.4% of respondents will use synthetic anti-malarials, consult a herbalist and use local herb, respectively, while 27.3%, 1.7% and 18.2% will go to the hospital, take spiritual/ritual waters for cure and just pray, respectively, with 3.0% of the respondents indicating that they will ignore the signs. Factors influencing respondents’ choice of malaria treatment and preventive methods included cost, religious beliefs, perceived safety, convenience and respondents’ state of health for 22.7%, 5.4%, 20.8%, 26.5% and 24.6% of the respondents, respectively. The use of insecticide impregnated net are uncommon amongst the respondents (0%). Treatment seeking practice in malaria was related to level of education and religion. We found that convenience and the severity of the disease affected respondents’ choice of treatment in more than 50% of the cases. We suggest that malaria public enlightenment efforts should be intensified, effective malaria preventive methods be made affordable and that support be provided to make malaria treatments at public hospitals free. Key words: Malaria, Attitudes, insecticide treated nets INTRODUCTIONAnnually, malaria kills more people in the tropics than any other infectious disease. The human and economic costs associated with declining quality of life, consultations, treatments, hospitalizations and other events related to malaria are enormous and often lead to low productivity and lost incomes. Experiences with malaria have shown that prevention is better and cheaper than cure; however the practice of malaria preventive measures has been related to the knowledge and belief of people and have been found to be low and difficult to implement when malaria risk is perceived to be low (Winch et al, 1994). Malaria-related knowledge, attitudes and practices (MKAP) have been examined in many rural and partly urban multiethnic populations in Africa (Okrah et al, 2002; Tsuyuoka et al, 2001; Dossou-Yov et al, 2001). Within Nigeria, surveys of residents of the Atlantic coast revealed a lack of knowledge and many misconceptions about the transmission and treatment of malaria, which could adversely affect malaria control measures and anti-malarial therapy (Afolabi- Web resource). Recommendations that preventive measures be incorporated into malaria alleviation programs in addition to developing an appropriate educational intervention strategy highlighting the importance of compliance have been made following results of “perceived malaria” management in a Nigerian setting (Erhun et al, 2002). MKAP is thus becoming more important to the design and improvement of malaria control activities, to the establishment of epidemiological and behavioral baselines and to identifying indicators for monitoring intervention programs (Schultz et al, 1994). This paper reports the results of the survey carried out to assess the MKAP of the multiethnic population of Ile-Ife town, Nigeria. Specific objectives were to ascertain the levels of knowledge regarding malaria, investigate attitudes and practices in the prevention and treatment of malaria and examine attitudes towards bednets and insecticide treatment MATERIALS AND METHODS A pre-coded questionnaire was self or researcher administered in a face-to-face interview approach. A team of 8 interviewers was trained by the researchers for three days before the start of data collection. The questionnaire was translated into Yoruba and a pre-test was conducted in Aba gboro and Parakin areas of Ile-Ife. Three hundred and twenty questionnaires were produced including 20 which were pre-tested across age and sex variables of target respondents. The results of the pretest were excluded from the analysis. The purpose of the study was very carefully explained to the target population (mainly decision makers for each selected household) and their consent individually obtained before the questionaire was administered. Ile-Ife (the study site) is an urban town in southwestern Nigeria; it lies in the tropical rain forest belt and has an estimated population of about 282,000. Ile-Ife has many satellite villages that are linked by a poor road network. For the most part, the villages have poorly developed infrastructures, often without access to either electricity or pipe-borne water. For this study, Ile-Ife (Figure 2) was divided into four regions consisting of 13 districts namely Iloromu, Ita-Olorun, Ibadan road, Eleiyele, Lagere, Modakeke, Igboya, Idio, Ilode, Arubidi, Iloro, Fashina and Ilesha road; one district was selected from each region into the sample to ensure geographic representation. The districts surveyed included Fashina in the central region, Ibadan road in the western region, Ilesha road in the eastern region, and Modakeke in the southern region. Sample selection involved the use of a two-stage cluster random sampling procedure at the district level to select sub districts and zones from where the study sample could be drawn. In each district, the area was broken down to sub districts from which three zones were selected based on population. Within the selected zones, households were randomly numbered, and houses assigned ‘odd number’ were selected into the final sample. A key decision-maker respondent (male or female) was identified for interview in the final sample population. Knowledge of malaria signs and symptoms, prevention methods such as bush clearing, use of insecticide impregnated nets, removal of stagnant water, use of insecticide, fumigation of homes and environment and the use of prophylactic anti-malarials were the main outcomes measured as determinants for “malaria prevention.”Statistical analysis was done using the SPSS version 10.0 software program. The research was funded by the authors. RESULTS Sample structureA total of 300 face-to-face interviews were conducted with respondents at their households. The sample was allocated to each district in proportion to its population. Proportionality was used in the allocation of sample down to the zone level. A large proportion of the sample was drawn from the districts of Ibadan road and Modakeke as they had the largest population among selected districts. The sample comprised about 63% male and 37% female respondents. This was designed to ensure a proportionate gender representation because both men and women play an important role in household decision making. Only 231 of the target population of 300 decision makers, (one for each sampled household) responded with 69 withdrawing (for reasons ranging from perceived anxieties that the results may be used for purposes other than earlier explained by the researchers and to what appears to be a general lack of enthusiasm toward surveys and apathy towards interventions perceived to be government oriented. There were questionnaires ‘dropped’ at the request of some household decision makers after initial interview that could not be retrieved as at collation time after several return visits, these were also tagged “withdrawn” Age distribution, education level and socio-economic status of respondentsThe majority of respondents were in the 18-40 age group (approx 70% of respondent) and approximately 30% were above 40 years old (Table 1) More than 23% of the respondents earned less than the national minimum wage (7,500 naira) (Table 1) while over 15% were without formal education (Table 2). Most households that were surveyed had 4 to 7 people (41.5%) and an average household size of six people. About 11% of households had nine or more members. Risk perception, malaria treatment and prevention factorsThe results indicated that over 90% of the respondents have had malaria at least once in the last one year and practice self medication. Most (73.5%) of the respondents willing to go to the hospital in the event of malaria attack, to use untreated bed nets (81.2%), insecticides sprays (72.4%) and insecticide treated nets (88.7%) as preventive measures have above secondary education. Most of the respondents (> 60%) are familiar with at least 3 signs/symptoms associated with malaria as defined by western medicine; 68.3%, 67.4%, 61.8%, 19.6%, 10.0% and 4.3% of respondents reported fever, headache, body pains, dizziness, vomiting and diarrhea respectively, as common symptoms of malaria. Table 3 shows malaria prevention methods studied and the respondents’ knowledge and practice of these measures. Figure 1 is an attempt to simulate the willingness of the respondents to use selected malaria preventive methods. Analysis of “what respondents will do first” during malaria attack showed that 35.5%, 0.9% and 13.4% of respondents will use synthetic anti-malarias, consult a herbalist or use local herbs, respectively, while 27.3%, 1.7% and 18.2% will go to the hospital, take spiritual/ritual waters for cure or just pray, respectively, with 3.0% of the respondents indicating that they will ignore the signs. Factors influencing respondents’ choice of malaria treatment and preventive methods include cost (22.7%), religious beliefs (5.4%), perceived safety (20.8%), convenience (26.5%) and respondents’ state of health (24.6%). DISCUSSION Malaria intervention goals in endemic areas should be to prevent mortality
and reduce morbidity as well as associated socio-economic losses. This
requires the progressive creation of capacities for assessing local malaria
situation and the selection of appropriate control measures. The study highlights
respondents’ perception of vector control methods and shows that the use of
untreated bed nets, fumigation and insecticide impregnated bed nets were not
common in the communities studied (Figure
1); for reasons bordering mostly
on perceived ineffectiveness and inconvenience. The use of bed nets reduce
the degree of human-vector contact and malaria transmission and the prevalence
of malaria infection can be significantly lowered by the use of insecticide
impregnated bed nets (Erhun.et al, 2002; El Nur, 1995–2000; Schultz et al,
1994). Thus, report shows that impact on malaria of insecticide-treated nets
seems good when compared with spraying trials (Mathenge et al, 2001). The survey
reveals that many of the respondents do not know that nets could be impregnated
with insecticides (68.7%, Table
3) not to mention using it as a control measure.
A sizeable proportion (86.5%) of the study population sees bush clearing as
effective malaria prevention method and about 36% are currently using this
method (Table 3). Generally this may not be an effective method for malaria
prevention. While current international effort at malaria control are targeted
toward the use of insecticide treated nets (ITN) for prevention via vector
control (8, 9, 10) only 31.3% of the respondents perceive this as an available
malaria prevention method and 3.3% preferring it as method of malaria prevention
with no respondent currently using ITN (Table
3). It is paradoxical that the
respondents were willing to buy malaria prophylactics and insecticide sprays
yet unwilling to utilize insecticide treated bed nets. Perhaps the initial
purchase cost may be a major factor here especially as over 50% of the respondents
earn Special strategies are needed to deliver subsidized ITNs to vulnerable populations in areas where malaria and poverty are most severe. The lack of shops with ITNs can be a major constraint to bednet ownership and use in these areas. Educating community members regarding the beneficial effects of using insecticide impregnated bed nets and implementing their use is an appropriate intervention to achieve high control of malaria vectors in endemic areas (Mathenge et al, 2001)) like Ile-Ife of Nigeria. The results indicate that the study population has a fair knowledge of the life cycle of malaria vectors as over 75% agreed that stagnant water could serve as breeding sites for mosquitoes (Table 3). Similarly, most of the respondents (> 60%) were familiar with the signs and symptoms associated with malaria; this is expected for a population in a malaria endemic area and with close to 80% having been formally educated. However a large percentage of the respondents practice self-medication; this is a very common practice in most malaria endemic countries (www.rbm.who.int; Curtis et al, 2000) Convenience and the severity of the disease were major indicators in over 50% of the respondents’ choice’ of treatment, thus indicating that they were used to malaria and have a reduced malaria risk perception. The endemic nature of the disease and the respondents confidence in self medication appear to make malaria “trivial” - a perception that is at variance with the emergence of drug resistant strains of malaria parasites from inappropriate therapy. Additionally, the study established a relationship between levels of education and appropriate malaria risk perception and attitude; as over 72% of respondents willing to go to the hospital in the event of malaria attack, use untreated bed nets, insecticide sprays and insecticide treated nets as preventive measures are educated to at least secondary school level. The socio-economic challenges in Nigeria have led many into looking unto a divine being for succor; however, The study showed that a sizeable percentage (19.9%) of the respondent population will first resort to spiritual means as a treatment method during a malaria incident. This is not very surprising since the belief in divine healing is not uncommon in the part of the country covered by this study. This may indicate a lack of confidence in malaria medicines. Conclusion Malaria public enlightenment efforts need be intensified, effective malaria preventive methods should be affordable and support should be provided to make malaria treatments at hospitals free. REFERENCES
The following images related to this document are available:Photo images[md05004f1.jpg] [md05004t2.jpg] [md05004t3.jpg] [md05004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}