 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 10, No. 1, Jan, 2007, pp. 9-18 Full length Research Article Determinants of Food Security Status of Rural Households Living With HIV/AIDS in Southwestern Nigeria Adenegan, K.O. and Adewusi O.A. Department of Agricultural Economics, University of Ibadan, Nigeria.. Received: October, 2006 Code Number: md07002 ABSTRACT The study assessed the determinants of food security status of households living with HIV/AIDS in Southwestern Nigeria. Eighty-five people living with HIV/AIDS were interviewed for the study. Descriptive statistics, cost of calorie measure and the Logit model were used in analyzing the data collected. The result shows that there is high prevalence of food insecurity among the households living with HIV/AIDS. The result of the Logit model also shows that gender, education, monthly food intake (Kcal), total monthly income, drug share and food share significantly influence the food security status of the households living with HIV/AIDS. To improve the food security status of households living with HIV/AIDS, it is recommended that economic policy should be directed towards the reduction of the food prices, thus reducing the food share of the household monthly expenditure Keywords: Food security, Rural household, HIV/AIDS, Southwestern Nigeria INTRODUCTION Food is rated as the most basic of all human needs (Koontz et al; 1983). Man needs food for life’s sustenance, prevention of sickness and in providing energy for the normal psychological activities of the body including the normal state of mind. Hence, the need for food security becomes pertinent as it eventually affects a nation’s productivity and growth. Food security requires access to food both in terms of availability which is described by the ability of the people to get food and for the people to buy the food. The bulk of food consumed in Nigeria is produced by small scale farmers whose small contributions are aggregated to meet the demand for food in the country, hence ensuring food security. Any medical problem which affects the health of these small scale farmers will affect their productivity. HIV/AIDS is one of such medical problems, but it also has social and economic dimensions. Its impact can affect labour and potential income of the victims and their families, which results in neglect or reduction in productive activities. Acquired Immunodeficiency Syndrome (AIDS) is a condition of illness caused by a virus known as human immunodeficiency virus (HIV). The devastating nature of this disease in the world today is unquestionable. No part of the world and no section of the population have been left untouched. Not only individuals and families but also the whole social environment itself is in danger. Of the 2.9 million HIV-related deaths in 2003, 2.2 million were from sub-Saharan Africa (UNAIDS, 2004). Alarmingly, the sub-Saharan African region contains only 10 percent of the world’s population, but accounts for 60 percent of the worldwide HIV/AIDS cases (25 million HIV/AIDS cases out of a worldwide total of 39 million) (UNAIDS Africa Fact Sheet, 2004). Thus, Sub-Sahara Africa where an estimated 26.6 million people are living with HIV and approximately 3.2 million new infections occurred in 2003 -is the region of the world that is most affected by AIDS (CTA, 2004). The HIV/AIDS pandemic has claimed the lives of over 20 million people in Sub-Saharan Africa (SSA), where the majority of the people live in rural areas and more than 80% are dependent on agriculture for their livelihood. . Also, most rural areas in SSA are typified by their poor access to health and education services, and limited use of agricultural inputs. HIV/AIDS represents a severe burden on SSA countries and it is compounding poverty in the continent. While by the end of 2004 over 2.3 million Africans had died of the disease, 25.4 million people were living with the HIV virus. Among those living with the virus, more than half (13.3 million) were women (UNAIDS, 2004). The first case of HIV/AIDS in Nigeria was reported in 1986. In 1991, the Federal Ministry of Health conducted the first sentinel sero-prevalence survey in Nigeria. In Nigeria, however, HIV prevalence rate is lower than that in some other African countries, but the absolute number of people affected may be larger in some cases. The 1991 sentinel survey showed that Nigeria, with a population of over 120 million had a national average seroprevalence of These surveys show a rise in HIV infection in Nigeria: from 1.8 percent in 1991 to 3.8 percent in 1995, to 5.4 percent in 1999, and 5.8 percent in 2001. These figures indicate that about 3.5 million Nigerians between the ages of 15 and 49 years are infected with HIV (NPC,2000; National AIDS/STD Control Programme/FMOH, 2001). Thus, HIV/AIDS normally hits the most sexually active part and most economic active segment of the population, which includes farmers, and the skilled and trained labour force. The most recent National HIV/syphilis sentinel seroprevalence survey was in 2004 and it estimated that there were 3,300,000 adults living with HIV/AIDS in Nigeria, 1,900,000 (57percent) of these are women. In this survey, the national prevalence rate had fallen to 5 percent from 5.8 percent in 2001(Adeyeye, 2005). Insecure livelihood is one of the means to increase the vulnerability to risky behaviours and HIV infection through immoral actions. People engage in high-risk survival strategies that increase their chances of contacting or spreading HIV and other sexually transmitted infections. Such strategies may be the only means of feeding one’s family during desperate times of food insecurity like lean periods, drought, economic decline or war. During these periods of food insecurity, male family members migrate in search of work and are separated from their wives and families for long periods of time. This increases the chances that they will take on multiple casual sex partners. The fact that families often split up while flee insecurity can also easily contribute to the spread of HIV (WFP,2003). Increased adult mortality leaves large number of surviving family members with lower incomes, worsened health and reduced prospects for the future. Also, women are important actors in relation to food security and development and their role is very critical for food security in Nigeria. They are the primary agricultural producers they prepare food and take care of the family. According to Meludu et al (1999), women produce between 60-80 percent of food in Nigeria. Their high vulnerability to HIV/ AIDS poses a big problem for the future of agriculture. As the HIV/AIDS pandemic has evolved, it has become apparent that the increasing contact between rural and urban areas through trade, migration and improved transportation networks have made HIV spread fast to rural areas and this in turn has affected the labour intensive sectors such as agriculture. For poor households, HIV/AIDS represents one more often massive and temporary shock that can seriously affect their ability to sustain their livelihoods and remain food secure. As impoverished families try to cope with HIV/AIDS morbidity and mortality, they become incrementally poorer after reducing their meager assets, sometimes to a crisis point that threatens to dissolve the family unit. Faced with significantly reduced income, fewer people available to work and an unrelenting need for food and medicine, family members may be forced to adopt high-risk behaviours (such as trading sex for food) just to survive. Poor people who are affected by HIV/AIDS need both treatment and food. And this ultimately affects the food security of households, communities and the nation as a whole. The issue of food security and HIV/AIDS is perceived to be inseparable. Indeed, food security can be seen as one more way to prevent the spread of AIDS, and reduce its impact (WFP, 2003). HIV/AIDS mortality also affects food security by reducing household’s ability to produce and buy food by depleting assets; reducing agricultural productivity by affecting labour availability, thus forcing households to remove labour from agricultural production to care for the HIV affected members of the family. This is also linked up with the economic situation of the household. Since HIV/AIDS is a medical problem, which has social and economic dimensions and is becoming a particularly big problem in rural Africa, Nigeria inclusive, it is pertinent to look into the effects of the disease on the food security of rural households. This study therefore seeks to determine the food security profile of the HIV/ AIDS households and identify the determinants of food security. Conceptual Framework Food security is defined as physical and economic access to sufficient, safe and nutritious foods which meet the individual’s dietary needs and food preferences for an active and healthy life. There are three key dimensions to household food security; food availability, food access, and utilization of food by the body (Kennedy, 2003). Food security in general is a concept that integrates a number of important issues the magnitude of which range from microeconomics to macroeconomics. The World Bank (1986) however defined household as a group of individuals living under the same roof and eating from the same pot or source of provision of food. For households to achieve food security, they must have the means to produce or purchase the food they need to ensure that the dietary requirements of all family members are met. The inter-relationship between HIV/AIDS and food security is very strong. HIV/AIDS reduces food availability through falling production, loss of family labour, land and other resources; loss of livestock assets and implements. It also reduces food access through declining income for food purchases. In addition HIV/AIDS reduces the stability and quality of food supplies through shifts to less labour intensive production (Loewenson and Whiteside, 2001). Impact of HIV/AIDS on households can also be analysed from a livelihood perspective, looking at access to resources of households especially farmers. In terms of human capital, HIV/AIDS leads to loss of labour of the infected person, but eventually time allocation of his or her caretakers and those attending funerals will be shifted away from productive labour. Human capital is not only about manual labour but also about knowledge and skills. Illness and death of parents prevent the transfer of knowledge to their children on land preparation, crop cultivation, cultural beliefs and traditions. In terms of financial capital, direct expenses for the infected individual concern medical and funeral expenses. Loss of income of infected person may also have serious consequences. More indirectly, access to credit or savings becomes difficult as affected households become less credit worthy (Bechu et al, 1997). In terms of social capital, the generation of orphans constituted an important loss of social capital without access to formal or informal training, or access to resources. Hence, their opportunities to build up a safe and adequate livelihood are minimized. Social networks often provide safety nets for those having problems. Yet the stigma attached to HIV/AIDS may lead to exclusion from social networks for those needing support. Feared stigma may prevent people to acknowledge their status. Furthermore, poor families have less access to social networks as these are built upon the concept of mutual assistance (Shah et al, 2002). In terms of physical and natural capital, HIV/AIDS leads to the neglect of infrastructure. Lack of labour leads to reduced soil fertility maintenance because most of these activities are labour intensive. The reduction in capital will lead to insecurity of livelihoods and thus food insecurity. The negative impact of HIV/AIDS on nutrition and food security expands from the household to the community to different parts of the country. The socio-economic deterioration will eventually lead to a decrease in the labour force, worker productivity, total outputs and overall economic growth which would lead to a decline in national food supplies and a rise in food prices. The epidemic has a major impact on development because it undermines three of the main determinants of economic growth: physical, human and social capital. Many agricultural and rural development institutions can no longer achieve their planned programme output. Without the necessary institutional support services, the agricultural and rural development sectors are failing to realize the forecasted growth rates and planned production targets (FAO, 2005). The impact of HIV/AIDS on crop production relates to a reduction in land use, a decline in crop yields and a decline in the range of crops grown. The reduction in land use is incurred as a result of sickness and death in households, leading to fewer family members available to work in the fields and thus reduction in the size of the land that can be cultivated. This ultimately results in poverty, which results in malnutrition, and which in turn affects the health of family member and their ability to perform agricultural work, and which leads to reduced cash incomes needed to purchase inputs such as seed and fertilizer. The impact of HIV/AIDS on livestock production has been felt in so many ways. Cattle are frequently sold to pay medical bills and funeral expenses and decrease in labour availability result in lower levels of care for livestock. HIV/AIDS can manifest itself in various ways. It may result in labour shortages, forcing farm households to shift from cash to subsistence crops when food security is being threatened. Moreover, in rural Nigeria, where farming is predominant, youths and adults in their most productive age groups are the most vulnerable and at highest risk to AIDS. The high death rate among young adults (20 to 40 years of age) is depleting human capital and the skill base necessary for social development and economic growth. The high replacement cost of workers and rising labour costs caused by diminished productivity, sick leave, and absenteeism discourage investments, and hence reduction of farm labour results which will force farmers to switch from large scale commercial farming to subsistence agriculture. As a result, the high rate at which this group is being infected is currently a matter of concern to the governments at all levels since these youths constitute virtually 75 percent of the Nigerian labour force (Oke, 2000; USAID, 2000). The rural sector is also not unaffected in several other ways because the households sometimes sell their production assets in order to pay for medical bills and take care of infected member(s). This, no doubt will reduce productivity, diversification of sources of income and outputs, food security, nutritional status, and sustainability of resources (CTA, 2004). OBJECTIVES OF THE STUDY The main thrust of the study is to identify the determinants of food security status of rural households living with HIV/ AIDS in southwestern Nigeria. The specific objectives are to:
METHODOLOGY The Study Area The study area is the southwestern Nigeria. The technical report of the National HIV sero-prevalence sentinel survey FMOH, Abuja (2003), records the prevalence in such peri-urban areas as Ejigbo, Saki and Eruwa in the southwestern parts of Nigeria. Ejigbo has the highest prevalence and is therefore chosen as the case study for this research. Ejigbo is a peri-urban center with rural suburbs located on latitude 7.95 degrees north of the equator and longitude 4.40 degrees west of the Greenwich meridian in South Western Nigeria. Emigration is a prominent feature of Ejigbo households with close to four fifths of the members being migrants at one time or the other. The causes of their movement being employment seeking in other African countries like Ghana, Togo, Republic of Benin and most especially Cote d’ivoire. Sampling procedure The study used primary data collected with the use of structured questionnaires. The target populations were men and women who had tested positive to HIV/AIDS and were receiving aids and antiretroviral drugs at the Baptist Hospital, Ejigbo. One hundred questionnaires were administered, out of which only eight-four were properly completed and returned. Data were collected on household head age, sex, marital status, family size, primary occupation, household health information, household income, household expenditure, and household food consumption and household coping strategies against food insecurity. Methods of Data Analysis Analysis was carried out using descriptive statistics, Greer and Thorbecke food security measure and the Logit model. The food security for the households was measured from the food insecurity line which was constructed with a regression model using the cost of calorie method proposed by Greer and Thorbecke (1986). The cost of calorie function of these forms were estimated LnX = α+βC ……………… (i) Where X = food expenditure C = calorie consumption The calorie content of the recommended daily nutrient level (L = 2250Kcal) was used to derive the food insecurity line Z. Z = e(α+βL) ………………. (ii) People below this line are classified as food insecure. Calorie consumption per adult equivalent of households were estimated following Oguntona and Akinyele, (1995)’s table of the nutrient composition of commonly eaten foods in Nigeria while the determinants of food insecurity of the households under study were identified using the Logit model. THE LOGIT MODEL. The logit model postulates that the probability (p1) that a household living with HIV/AIDS is food secure as a function of an index (Zi). Zi is also the verse of the standard logistic cumulative function of Pi i.e. Pi (y ) = f (Zi) Zi is also the verse of the standard logistic cumulative function of Pi i.e. Pi (y =1) = f (zi) The probability of a household living with HIV/AIDS being food secure is given by Pi (y = 1) = 1/1 + e-zi
The dependent variable (Yi) is a dummy. It takes the value of 1, if a household living with HIV/AIDS is food secure and 0 if otherwise because dependent variable is binary. The maximum likelihood estimate is used to analyze the model. The probability of a household living with HIV/AIDS being food secure (Pi) by an household is calculated from YI value: Yi = bo + b1 x1 + b2 x2 ----------- + bn xn where b0 = constant The explanatory variables Xi are: X1 = Age (years) X2 = Age squared X3 = Gender (1=male-headed household, 0 if otherwise) X4 = Household size X5 = Years of formal education X6 = Non-farm income ( X7 = Monthly food intake (Kcal) X8 = Total household monthly income (household monthly expenditure used as proxy) X9 = Food share of the total household monthly expenditure X10 = Drug share of the total household monthly expenditure RESULTS Household Socio-Economic Characteristics The household’s socio-economic characteristics were described using descriptive statistics of frequency and percentage distribution tables. Table 1 show that the mean and the modal age of household heads with people living with HIV were 44.72 years and 45 years respectively. This indicates that on the average, household heads of households with people living with HIV are in their economic active years. Table 1: Socioeconomic characteristics of HIV household heads
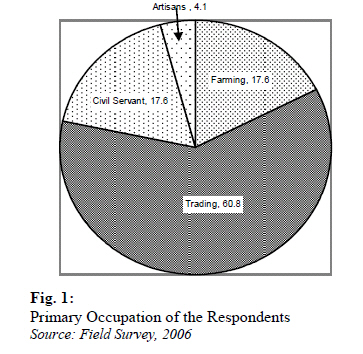
Source: Field Survey, 2006 On the average the mean and modal household size was four with a low standard deviation of 1.57. This shows that most of the HIV households were small. The average years of formal education of the HIV-infected household heads 5.71 while a larger proportion of the household heads had no formal education. Thus, on the average, the household heads had at most primary education. This reflects a characteristic of rural and peri-urban centres The results in Fig 1 indicate that only 17.6 percent of the household heads were farmers while 83.4 percent are engage in non-farm activities as their primary occupation. About 60.8 percent were traders. This indicates that the major primary occupation in the study area is trading. The mean drug expenditure, food intake and food share of the monthly expenditure are Household Food Security Profile The Ordiary Least Square (OLS) regression model for estimating the constant value in the cost-of calorie function used in determining the food security profile of the household. This regression result was significant at 5 percent level and has a direct relationship with food expenditure. The coefficient of determination is 0.301 meaning that calorie consumption explains about 30.1percent of the variability of food expenditure. Table 2: Statistical distribution of household monthly drug expenditure, food intake and food share
Source: Field Survey, 2006 Table 3: The Result of the OLS Regression Analysis of the Cost of Calorie
R-squared= 0.301054; Adjusted R-squared 0.290982 Table 4: Distribution of household food security
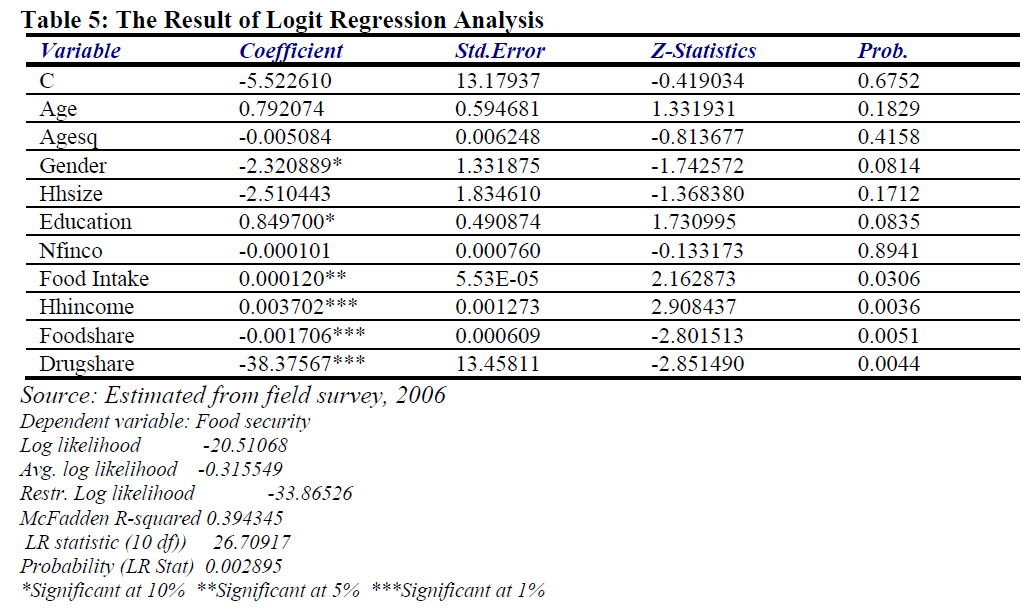
Source: Field Survey, 2006 The explanation of this result is that, a large proportion of the income of the respondent is spent on drugs. Thus affecting the amount available to them to spend on food, this in turn affects the quantity of food available to the household to meet their daily food requirements. The food insecurity line Z was estimated to be 45,987.926 Kcal. The findings on Table 4 show that majority (80 percent) of the households living with HIV/AIDS fell below food security line. Thus, there is high prevalence of food insecurity among the households living with HIV/AIDS. Determinants of household food security The determinants of household food security were identified using the logit model. The result of the model is given in Table 5. The model has the log likelihood value of -20.91178 and is significant at one percent. This indicates that all the independent variables jointly explain the dependent variable and that the model displays good fit. The result shows that gender, years of formal education, monthly food intake (Kcal), household monthly income, drug share and food share significantly influence the food security status of the households living with HIV/AIDS. Food intake, years of formal education and household monthly income have direct relationship with the probability of the household being food secure while gender, years of formal education, food share and drug share of monthly expenditure are inversely related to the probability of the household being food secure. The result indicates that an increase in food intake (Kcal) and total household monthly income would result in increase in the probability of the household being food secure. Thus, a household with high monthly income stream is expected to have high calorie consumption and be food secure. Also, an increase in years of formal education, would result in increase in the probability of the household living with HIV/AIDS being food secure. This indicates that education is a means to enhancing food security in the rural areas. This could be because education enhances early adoption of innovation which would result in higher productivity and farm income. Also, education could enhance household engagement in non-farm activities, thus increasing household income. Households with higher income would spend less proportion of household income on food. Thus, a reduction in the food share of the monthly income would result in increase in the probability of the household living with HIV/AIDS being food secure. This is consistent with Engel’s law that the higher the income the less the proportion of the income spent on consumable goods, while the higher proportion is spent on luxuries. Households with higher food share are food insecure and low-income earners, who spend a higher proportion of their monthly income on food. Also, a decrease in the drug share of the total household monthly income would result in an increase in the probability of being food secure. This indicates that if the prices of the anti-retroviral drugs are reduced, the households have additional money to augment their food need. Furthermore, a decrease in male-headed households living with HIV/AIDS would result in increase in the probability of the household being food insecure. This indicates that female-headed households living with HIV/AIDS are more food secure. Summary, Conclusion and Recommendations The study shows that on the average, household heads of HIV infected households are in their economic active years and the mean household size was four. The average years of formal education of the household heads was 5.71years while a larger proportion of the household heads had no formal education. Thus, on the average, the household heads had at most primary education. A larger proportion (80 percent) of the households living with HIV/AIDS was food insecure. The result also shows that gender, years of formal education, monthly calorie consumption, household monthly income, drug share and food share significantly influence the food security status of the households living with HIV/AIDS. Food intake, years of formal education and household monthly income have direct relationship with the probability of the household being food secure while gender, years of formal education, food share and drug share of monthly expenditure are inversely related to the probability of the household being food secure. Since female-headed households living with HIV/AIDS are more food secure than those of their male counterparts, efforts should be intensified on empowering the female household heads in terms of capacity building, access to livelihood assets and finance. Furthermore, food policy should be directed towards the reduction of the prices of food items, thus increasing the purchasing power of households living with HIV/AIDS and consequently reducing the food share of the household monthly expenditure. Government should also ensure availability of highly subsidized anti-retroviral drugs in all the sentinel centres. Increasing Government expenditure on the Universal Basic Education is not sufficient, the constitution should enforce adherence of the populace to the policy, especially in the rural areas. REFERENCES
© Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md07002f1.jpg] [md07002t5.jpg] |
| |||||||||


{kind=link}
{kind=link}