 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
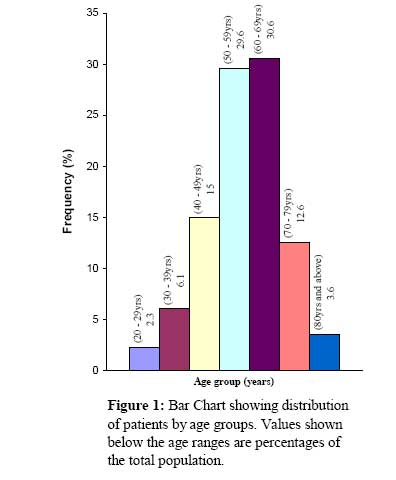
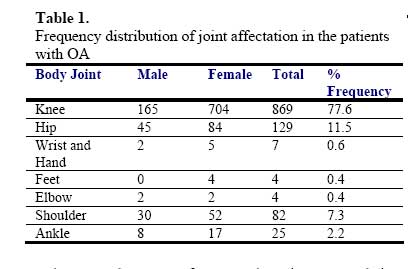
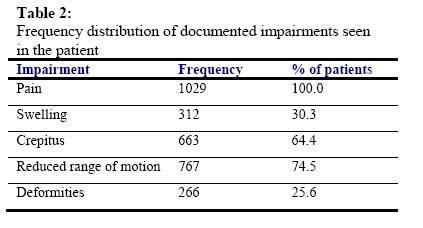
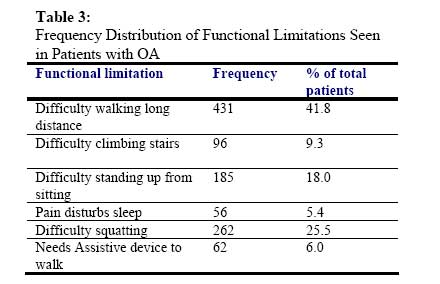
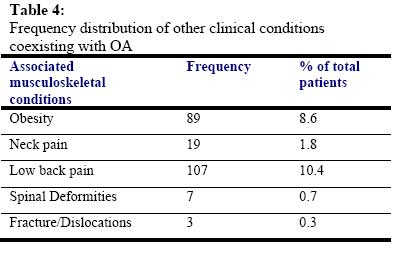
African Journal of Biomedical Research, Vol. 10, No. 2, 2007, pp. 111-115 Full Length Research Article Pattern of Osteoarthritis Seen In Physiotherapy Facilities in Ibadan and Lagos, Nigeria Aderonke O. Akinpelu; Oyindamola O. Alonge, Babatunde A. Adekanla and Adesola C. Odole Department of Physiotherapy, College of Medicine, University of Ibadan. Ibadan, Nigeria Received: February 2007 Code Number: md07015 ABSTRACT Osteoarthritis (OA) is the leading cause of disability in the elderly. Studies on its prevalence and pattern in Nigeria are few. The aim of this retrospective study was to describe the pattern of OA seen in 10 physiotherapy facilities in Ibadan and Lagos. The University of Ibadan/University College Hospital Ethical Review Committee approved the study. Information on age, gender, joint affectation, impairments, disabilities and co-morbidities were recorded from the hospital files of patients with OA in each hospital. The proportion of all new patients accounted for by OA during the 3 year study period was computed. Data was analyzed using descriptive statistics.The patients with OA, aged 56.8+ 12.6 years accounted for 8.9% of all (11574) new patients seen in the clinics during the study period. The female to male ratio was 3.5:1. The knee was the most frequently affected joint. Common impairments were pain (100%), reduced range of motion (75%), crepitus (64%) and joint swelling (30%). Common functional limitations were difficulty in walking long distances (42%), squatting (22.5%), standing up from sitting (18%) and climbing stairs (9%). Low back pain (10.4%) and obesity (8.6%) were the two most commonly documented comorbid conditions. It was concluded that OA is a common condition seen in the Physiotherapy facilities in Lagos and Ibadan, accounting for about 9% of new patients; it is more common in females than males (3.5:1) and the knee joint is the most frequently affected. Keywords: Osteoarthritis, Pattern, Physiotherapy clinics, Nigeria. INTRODUCTION Osteoarthritis (OA) is a chronic degenerative joint disease and a leading cause of disability, affecting 60-70% of the population older than 60 years (Lane, 1997). It is a slowly progressive disease characterized by reduction in proteoglycan aggregates within the joint cartilage matrix, leading to loss of cartilage, eburnation of bone and ultimately joint pain (Morehead and Sack, 2003). Its symptoms include joint pain, joint stiffness, tenderness, swelling, crepitus and a limited range of motion (Schnitzer, 1996). Although OA occurs all over the world, ethnic differences in its prevalence exist (Mody and Woolf, 2003). Prevalence of knee OA has been found to be higher in black South Africans compared to white South Africans and in Americans of African origin, especially women than in White Americans (Anderson and Felson, 1988). It has been reported to be more common in Europeans than in Chinese, Jamaicans and Africans from Nigeria and Liberia (Felson and Zhang, 1998). Studies from Asia (Mangat et al. 1995) and Africa (Eti et al 1998; Adebajo 1991; Obwueke and Imogie, 2003) have found the knee to be the most frequently affected joint. These studies have also reported female bias in the prevalence of OA. Previous studies on pattern of OA from Nigeria (Adebajo, 1991; Obwueke and Imogie, 2003) are few. The aim of the present study was to describe the pattern of OA in terms of age, gender, joint affectation, impairments, functional limitations and co-morbidity in patients seen in physiotherapy outpatient clinics of 10 tertiary and secondary health institutions in Ibadan and Lagos, Southwestern Nigeria during a 3-year period (September 1999 - August 2002). MATERIALS AND METHODS This retrospective study was carried out in all but one tertiary and secondary health institutions with physiotherapy facilities in Lagos and Ibadan, Nigeria between September 1999 and August 2002. Permission to conduct the study was not granted in one teaching hospital. The study excluded osteoarthritis of the joints of the spine because in many cases, lumbar or cervical spondylosis was not differentiated from back and neck pain due to nondegenerative causes. The University of Ibadan/University College Hospital Ethical Review Committee approved the study. The number of all new patients seen in each clinic during the period of study was recorded from the register of new patients. The hospital numbers of patients with OA were noted and the following information was recorded from the hospital file of each patient: sex; age; joint(s) affected by OA; impairments; disabilities; other clinical conditions co-existing with OA seen in the patients. The proportion of all the new patients accounted for by osteoarthritis was computed. Data was analysed using descriptive statistics (mean, standard deviation, and mode and frequency distribution). RESULTS A total of 1029 patients with osteoarthritis (OA) were referred to the 10 physiotherapy out-patient clinics during the study, accounting for 8.9% of all (11574) the new patients seen in the clinics during the study period. The gender of 6 patients was not documented. Seven hundred and ninety five of the remaining 1023 patients (77.7%) were females and 228 (22.3%) were males, giving a female to male ratio of 3.5:1. The age of 102 (9.9%) patients with OA was not documented. The age of the remaining 927 patients ranged from 21 to 91 years and the mean age was 56.8±12.6 years. Only 8% of the 927 patients were less than 40 years old, 15% were aged 40-49 years old and the rest (77%) were aged 50 years and above. The peak age of affectation was 50-69 years, accounting for 61% of the 927 patients whose age was documented (Figure 1). One thousand one hundred and twenty joints were affected by OA in the 1029 patients surveyed (Table1). Ninety one patients had bilateral knee (85) and hip (6) joint affectation. The joint most frequently affected by OA is the knee joint, accounting for 869 (77.6 %) of all the affected joints. The next most frequently affected joint was the hip, occurring in 129 (11.5%) cases. The involvement of the shoulder (7.3%) and ankle (2.2%) joint was low and that of the elbow and the respectively. Sixteen patients had limb length small joints of the hands and feet was extremely low discrepancy and 9 had genu recurvatum. (<1%). The order of joint affectation by OA was similar in female and male patients (Table 1). Pain was the most frequent impairment and it occurred in all the 1029 patients. Reduction of range of motion, crepitus and joint swelling were documented in 75%, 64% and 30% of the patients respectively. Two hundred and sixty six (25.6%) patients had deformities (Table 2). Genu valgus and genu varus occurred in 155 and 86 patients The common functional limitations reported by the patients were difficulties in walking long distance (42%), squatting (22.5%), standing up from sitting (18%) and climbing staircase (9%). Only few (6%) patients used walking aids and sleep disturbance was documented in the hospital files of 56 (5.4%) patients (Table 3). Low back pain and obesity were the two most common co-morbid conditions seen in the patients and they occurred in 107 (10.4%) and 89 (8.6%) patients respectively. Other conditions were neck pain (1.8%), spinal deformities (0.7%) and fractures/dislocations (0.3%) (Table 4). DISCUSSION The finding that osteoarthritis accounted for about 9% of all referrals to the 10 physiotherapy outpatient clinics in Ibadan and Lagos, Nigeria between September 1999 and August 2002 suggests that OA is a common health problem in Nigeria and one that is often referred for physiotherapy. Where community-based prevalence rate of a condition is not readily available for referencing, hospital-based data may provide useful indication of how common the condition is in that population. Ninety two percent of the 927 patients whose ages were documented in this study were aged 40 years and above. This finding supports the fact that OA is a common health problem in middle and old age (Altman, 1991; Dequeker and Dieppe, 1998; Obuekwe and Imogie, 2003). The sex distribution of OA patients in this study indicates a female bias and it corroborates the findings of previous studies (Adebajo, 1991; Eti et al 1998). The female to male ratio (3.5:1) found in this study is lower than 5:1 reported by Adebajo (1998). The findings that the knee joint is most frequently affected by OA and that the joints of the hands and feet are least affected by OA among Nigerian patients in this study agree with findings of previous studies (Altman et al, 1989; Dequeker and Dieppe, 1998; Adebajo, 1991; Obuekwe and Imogie, 2003). Heberden’s nodes were not documented in any of the patients’ hospital files. All patients had joint pain thus supporting the fact that pain is the most common complaint in OA and the main reason why patients seek medical attention (Carlos and Roy, 1996). Other documented impairments were limitations of range of joint motion, crepitus and swelling. We however noted that early morning joint stiffness, joint line tenderness, bony enlargement and absence of local warmth, which are common impairments and part of the criteria for clinical diagnosis of knee OA by the American College of Rheumatology were not documented in any of the clinics. This may be due to the fact that Physiotherapists in Nigeria work as second contact healthcare providers; hence most cases referred to them are already diagnosed. About a quarter of the OA patients had deformities and as would be expected, they were knee deformities. The activity limitations experienced by the patients (difficulty in walking long distance, squatting and standing up from sitting) were those related to lower limb functions, since the most frequently affected joints were the knee and the hip. Some of these activity limitations have implications on some activities of daily living, cultural and religious practices of the patients. For example, difficulty to squat may limit patients' ability to use pit or Asiatic toilet, which is common in Nigeria, especially in the rural areas. Difficulty to squat can limit patients' ability to wash up or hand-wash clothes at low or floor level. Cooking with firewood and low stove is a common practice in Nigeria and the cooks often need to sit on very low stool. Patients with painful knee or hip often have difficulty performing this duty. The ability to perform some religious activities, such as kneeling to pray by Christians, bending and sitting on the heel by Muslims during prayers is limited in individuals with knee and hip OA. These limitations are not socially acceptable by most patients, especially the Muslims. Female patients, especially those that belong to the Yoruba ethnic group from Southwestern Nigeria often experience difficulty to genu-flex in order to show courtesy when greeting elders. Difficulty in walking long distance and climbing may also limit the ability to visit friends, and attend social functions. This is especially true of patients who do not own cars and have to walk long distances and travel by public transport vehicles. The small percentage of patients using assistive devices, such as canes and walking frames may imply some cultural reluctance towards the use of walking aids among the patients in Ibadan and Lagos, Nigeria. We acknowledge some limitations of this retrospective study. For example, age, occupation, and probably some symptoms were not documented in some cases. Despite these limitations, the findings of the present study provide useful information on the pattern of osteoarthritis in Ibadan and Lagos, Nigeria. CONCLUSION Our findings suggest that osteoarthritis is a common condition seen in physiotherapy facilities in Lagos and Ibadan, Nigeria, accounting for about 9% of referrals; it is more common in females than males in the ratio 3.5:1 and the knee is the most frequently affected joint. REFERENCES
© Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md07015t3.jpg] [md07015t4.jpg] [md07015f1.jpg] [md07015t1.jpg] [md07015t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}