 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
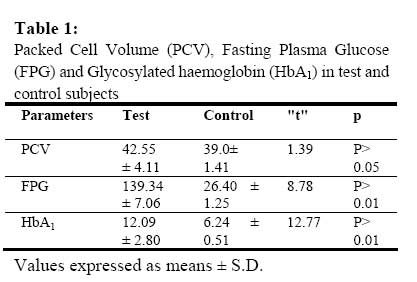
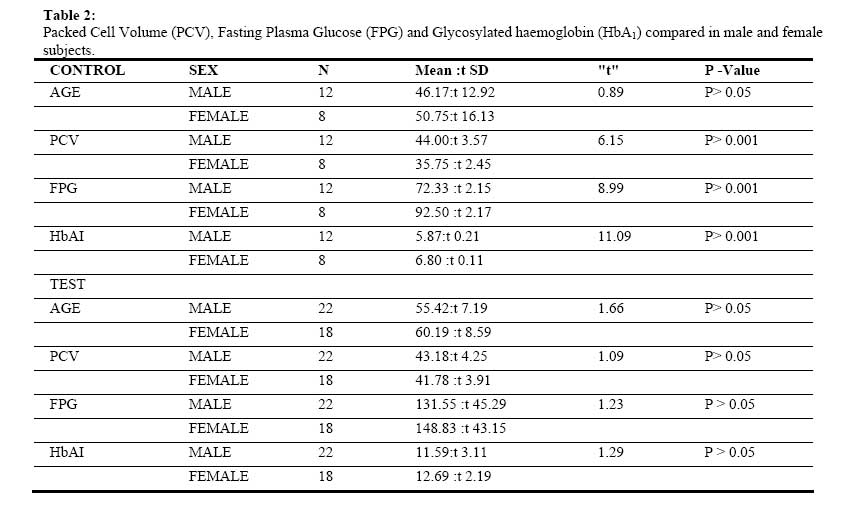
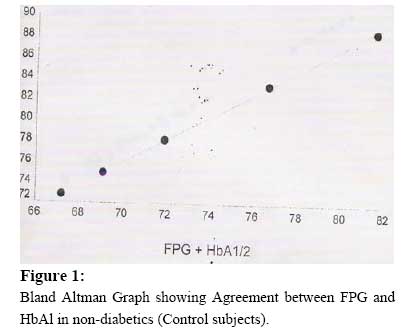
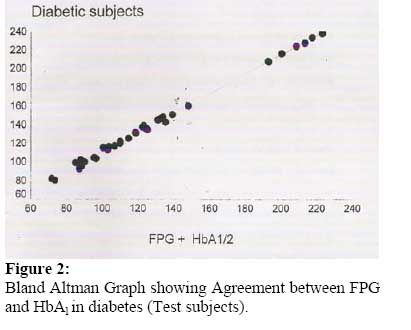
African Journal of Biomedical Research, Vol. 10, No. 2, 2007, pp. 127-132 Full Length Research Article Relationship between Fasting Plasma Glucose and Glycated Haemoglobin In Adult Diabetic Nigerians lAkinloye O.A, 2*Adaramoye O.A, 3Akinlade K.S, 2Odetola A. A. and 4Raji A.A. 1Department of Chemical Pathology, College of Health Science, Ladoke Akintola University of Technology, Osogbo, Osun State. Nigeria.2Department of Biochemistry, Faculty of Basic Medical Sciences, College of Medicine, University of Ibadan, Ibadan. Oyo State. Nigeria. . Departments of 3Chemical Pathology and 4Hematology, University College Hospital, Ibadan. Oyo State. Nigeria. Received: December 2006 Code Number: md07017 ABSTRACT The relationship between packed cell volume (PCV), fasting plasma glucose (FPG) and glycated haemoglobin (HbAI) was investigated in 40 diabetic patients (22 males and 18 females) and 20 apparently healthy controls (12 males and 18 females). Among the control subjects the FPG and HbA1 were significantly higher in the female than male subjects (P < 0.001). This gender differences was not found in diabetic patients (P < 0.05). While all the control subjects have FPG and HbA1 level within normal range (75- 115mg/dl and 5 – 8 %, respectively), 15 (38%) of the diabetic patients had FPG level within normal and only 5 (13%) had HbA1 level within the normal range. The FPG and HbA1 values were however, significantly higher in diabetic patients (139.34 ± 7.06 and 12.09 ± 2.80) than control subjects (76.40 ± 1.24 and 6.24 ± 0.51), respectively (P < 0.001). The PCV in controls correlated significantly with FPG and HbA1 (P < 0.001) while the FPG correlated significantly with HbA1 (P < 0.001). There was however only a significant correlation between FPG and HbA1 in the diabetic subjects. Bland Ahman graph shows a good agreement between FPG and HbA1, in both test and control subjects. These results show that PCV and gender factors have significant influence on FPG and HbA1 level in control subjects and were insignificant in diabetic patients. FPG and / or HbA1 are important and agreeable indices for assessment of glucose metabolism. Furthermore, there was an evidence of poor glycemic control in diabetic patients investigated in this study, probably due to poor compliance culture of the patients or inability to procure recommended drugs. INTRODUCTION Diabetes mellitus is a metabolic disorder characterized by raised plasma glucose levels. The relatively ineffective insulin in this condition results in hyperglycemia. Diabetes is becoming a major health problem in Nigeria with a prevalence of 1.4 – 2.7% (Erasmus et al., 1988; Ngumah, 1995; Bakari et al., 1999) and over 90% of these are non-insulin dependent (NIDDM) (Ohwworiole et al., 1988; National survey, 1997). Insulin enhances the entry of glucose into the tissue cells, where it is metabolized to produce energy. Excess cellular glucose is stored as glycogen, which may be catabolized in time of need. However, the presence of excess glucose circulating in the blood results in potential pathological complications (Morris et al., 1990; Philips et al., 1999). Diabetes causes prolonged ill – health, impose morbidity and mortality risk (Wokoma, 1999; Erasmus et al., 1999), necessitates a change in lifestyle with a meticulous daily routine and long – term self care with committed compliance to patients care plan (Bille, 1986; Hughes, 1987). Excess circulating glucose in diabetes is a reactant molecule that is involved in the glycosylated atom of other biomolecules and tissues. Glycosylation of haemoglobin is particularly popular and of great clinical importance. Glycated haemoglobin (HbA1) expressed as a percentage of total blood haemoglobin concentration gives a retrospective assessment of the mean plasma glucose concentrating during the preceding 6 – 8 weeks. Its measurement is therefore discussed as good method of assessing glycemic control (Nathan, 1995; Dandson and Schriger, 1999). The higher the percentage of circulating HbA1in the diabetes, the poorer the mean diabetic control. In the current study, FPG was correlated with HbA1 in order to investigate the possible relationship between FPG and HbA1 in established diabetic patients in Nigeria. The possible influence of gender and PCV was also investigated. This study also attempts to reveal the level of compliance of patients in this environment to diabetic care/control measures. MATERIALS AND METHODS Subjects: Twenty non-diabetic healthy looking subjects (12 males, 8 females) and forty diabetic patients (22 males, 18 females) attending medical out patient clinic (MOP) and metabolic research ward of Department of Chemical Pathology, University College Hospital Ibadan were recruited into this study. About 6-10mls of venous blood, fasting sample was collected and distributed into fluoride oxalate bottles for fasting plasma glucose (FPG), Lithium heparin bottle for Glycosylated haemoglobin (HbA1) and Ethylenediamine Tetraacetic Acid (EDTA) bottles for packed cell volume (PCV) estimation. Methods: Packed cell volume (PCV) was estimated by micro haematocrit method as described by Dacie and Lewis, (1991), while the Fasting Plasma Glucose (FPG) was estimated by glucose oxidase– protein precipitation (GOD-PAP) enzymatic colorimetric method of Barham and Trinder, (1972). Glycosylated haemoglobin was determined in whole blood using the ion-exchange resin method of Nathan, (1984). Briefly, the technique explores the ion charge on HbA1 to separate it from normal HbA. At the analytical pH the normal haemoglobin fraction (HbA) is retained by the ion-exchange resin, while the glycosylated haemoglobin fraction HbA1 has a net charge that will make it to remain in the supernatant. The rapid phase separation with the aid of plastic separator, separate the resin from supernatant, allowing a quick evaluation of the relative proportion of HbA1 with respect to total HbA. The optical density of each proportion was then measured spectrophotometrically. Statistical Analysis: Statistical Package for Social Sciences Software (SPSS) was used for the analysis of results. The results were expressed as means ±S.D. The paired "t" test was used to determine significant difference between test and control subjects. Statistical significant level was put at P < 0.05. Relationships between the investigated parameters were established using Pearson's correlation. RESULTS The means ± S.D. of packed cells volume (PCV), fasting plasma glucose (FPG) and glycosylated haemoglobin (HbA1) were presented in Table 1. This parameter was compared between test and control subjects using paired sample “t” test. There was significant increase in FPG and HbA1 of diabetic patient compared with control (t = 8.78 and 12.77 respectively, P < 0.01). However, there was no significant difference in their PCV (t = 1.39, P > 0.05). Table 2 shows a significant increase in PCV of male control subjects compared with female (P < .001) and a significant decrease in FPG and HbA1 (P < .001). This gender differences was however not observed in diabetic patients. Using Pearson’s correlation statistical method, gender difference (sex) shows significant positive correlation with PCV, FPG and HbA1 (r = 0.828, 0.912 and 0.914 respectively, P < 0.01) in control subjects. There was also a positive correlation between FPG and HbA1 (r = 0.723, P < 0.01). There was no correlation between gender (sex) and these parameters in test subjects, but FPG correlated positively with HbA1 (r = 0.616, P < 0.01). Furthermore, Bland Ahman graph shows agreement between FPG and HbA1 both in diabetes and control subjects (Figures I and II). DISCUSSION In developing countries the only means of screening for diabetes or monitoring its treatment is by determination of fasting plasma glucose concentration (Dandson and Schriger, 1999). The role and importance of glycated heamoglobin in the long-term assessment of diabetic patients has been recognized and appreciated (Malik et ai., 1996). This study demonstrated a good agreement between these two parameters in the assessment of glucose metabolism in the diabetes. A significant positive correlation was found both in diabetic patients and control subjects (r = 0.616 and 0.982 respectively, P < 0.001). This indicates that the higher the fasting plasma glucose the higher the glycated haemoglobin and thus implies that glycosylation of haemoglobin increases with increase in plasma glucose. It is of interest to note that gender difference and packed cell volume (PCV) of subjects correlated significantly with FPO and HbAI (P < 0.001) in control subjects. It is an established fact that PCV is generally higher in males than in females (Dacie and Lewis, 1991). This is consistent with the observation of the present study. However the relationship among PCV, FPO and HbA) in control and diabetic subjects has not been established. In this study, significant gender differences were found in FPO and HbAI of control subjects. FPO and HbA) were significantly higher in females than males.This may be due to lower packed cell volume in females, implying lower haemoglobin available for glycosylation and probably more plasma fraction of blood and hence more plasma glucose compared to male. This may be partially responsible for better glycemic control in male type 2 diabetic patients compared to females as reported by Valle et ai., (1999) Interestingly, this gender difference in FPO and HbAI was not observed in diabetic patients. This implies that the influence of gender (sex) and PCV on glucose metabolism is loss in diabetic patients. FPO and HbAI is therefore solely a representative of glucose metabolism in adult diabetes. This is further established by significant correlation between these parameters (r = 0.616, P < 0.001). The evidence available in this study may however not be able to prove that the same will be applicable to anemic patients, a very common problem in the tropics. The main use of glycated haemoglobin is to assess long - term glycemic control in the management of diabetic patients, to provide valuable informati<:m about the average blood glucose levels over the previous 1-2 months and to monitor compliance of patients to treatment regimens (Goldstein et al., 1982 & 1986; Meidema and Casparie, 1984; Lester, 1989) In this study, while all the control subjects have FPG and HbA) levels within normal range (75115mg/dl and 5 8%, respectively). About 15 (38%) of the diabetic patients have FPG within normal range and 28 (70%) have FPG below 140mg/dl, borderline for diabetes. Only 5 (13%) have HbAI within normal range (5 - 8%). There is a possible indication of poor glycemic control in the diabetic patients investigated in this study. This probably implies that these patients only prepared themselves for clinic days. This is consistent with the observation of Watkins, (1993). In conclusion, there is a good agreement and strong relationship between FPG and HbA]. Gender (Sex) and PCV influences FPG and HbA) in non - diabetes subjects but this influence is loss in diabetic patients. FPG and HbA, are therefore, main factors of monitoring glucose metabolism in diabetes. This study reveals a poor glycemic control in patients investigated and possibly poor culture of diabetes care. REFERENCES
© Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md07017f1.jpg] [md07017t1.jpg] [md07017t2.jpg] [md07017t3.jpg] [md07017f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}