 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
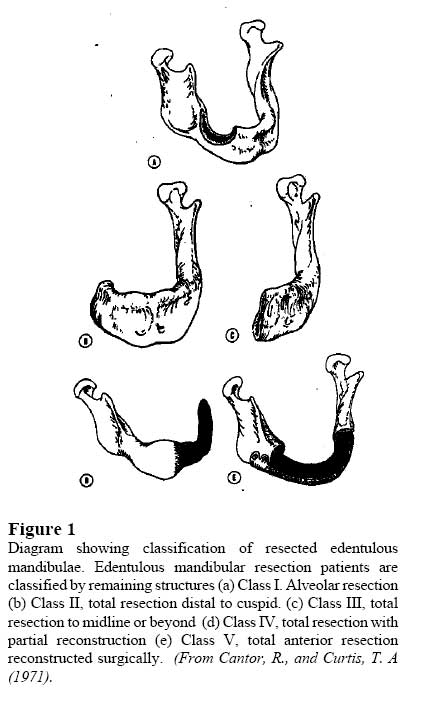
African Journal of Biomedical Research, Vol. 10, No. 2, 2007, pp. 197-201 Case Report Sectional Removable Partial Denture Design for the Treatment of Partial Mandibulectomy Patient: A Case Report Dosumu O. O., Arigbede A. O, Ogunrinde T.J. Department of Restorative Dentistry, University College Hospital, Ibadan, Nigeria Received: November 2006 Code Number: md07027 ABSTRACT Surgical removal of tumors in the mandible may result in discontinuity of bone which may require surgical reconstruction of the defect to provide a suitable tissue foundation for an acceptable prosthesis. Failure of reconstructive surgery for some mandibulectomy patients often make prosthetic rehabilitation extremely difficult. Due to financial constraints an acrylic sectional partial denture was fabricated for a class VI mandibular resection patient who had undergone anterior segmental mandibulectomy with no surgical reconstruction. The case was challenging and the prosthesis was well tolerated during a 6 months follow-up review. Keywords: Removable Partial Denture, Design, Mandibulectomy, Case report INTRODUCTION Tumors in the mandible usually require surgical removal with or without resection of normal bone at the margins of the lesion. Smaller lesions removed without discontinuity of the bone are relatively simple to restore with prosthesis while larger lesions may be more difficult to restore even though the continuity of the mandible is maintained (Shu-thic Mou et al,2001). The prognosis for edentulous segmental mandibulectomy patient becomes less favourable as the size of the resection increases (Shu-thic Mou et al,2001; Beumer et al, 1996). Success of prosthesis for resected edentulous mandibule is directly related to the amount of the remaining bone, the number and integrity of remaining teeth and continuity or discontinuity of the bone defect (Martin et al, 1994). Frequently surgical reconstruction of the defect is required to re establish the continuity of the mandible through bone graft or to create a buccal or lingual sulcus to provide a suitable tissue foundation for an acceptable prosthesis Cantor and Curtis (1971). In addition, pre-prosthetic implant placement may be required to improve denture retention and stability. Failure of reconstructive surgery for mandibulectomy patients often makes prosthetic rehabilitation extremely difficult. The presence or absence of natural teeth in a resected mandible often determines the approach to prosthetic rehabilitation. Cantor and Curtis (1971) classified edentulous mandibular resection patients by the amount of mandible that remains after resection and surgical reconstruction. Although the classification was suggested for edentulous patients, it is also applicable to partially edentulous patients (Firtell and Curtis, 2002). The classification aids the understanding of the treatment need of the patient and the challenges of prosthetic rehabilitation of mandibulectomy patient. Classification of Mandibular Resection Patient (Cantor and Curitis, 1971) In class I mandibular resection patient, there is radical alveolar resection and the continuity of the mandible is preserved (fig 1A). The class I patient functions well with removable partial denture, though may have some anatomic or functional limitations. In class II mandibular resection patient, the total mandible has been resected distal to the canine (fig 1B). In this class there is associated loss of function of the attached muscle resulting in deviation of the remaining mandible toward the surgical defect. When compare to class I patient, they are more difficult to rehabilitate with prosthesis The class III mandibular resection patient has the mandible resected to the midline or possibly beyond (fig 1c). The patient in this class presents with increased problems with mandibular deviation and denture instability. The Class IV mandibular resection patient has had a lateral resection and subsequent bone augmentation to form a pseudoarticulation of bone and soft tissue in the region of the ascending ramus (Fig 1 c). In this class of patients there is less mandibular deviation. In class V mandibular resection patient, there is anterior resection that crosses the midline but bilateral mandibular articulation has been maintained and the continuity of the mandible has been restored surgically by placing an autogenous bone graft. The class VI mandibular resection patient is similar to class V patient but the continuity of the mandible has not been restored surgically. Because each lateral fragment moves individually, the prognosis for a removable prosthesis is poor. Design of prosthesis for mandibular resection of partial edentulous patient should follow the principle of partial denture design5. However the application of these principles in mandibular resection patient may vary due to the specific need of each patient. Rehabilitation of class VI mandibular resection patient is a great challenge in prosthodontics. The independent movement of each lateral fragment gives unstable support for prosthetic fabrication and loss of anterior base of tongue leads to loss of tongue control and difficulty in controlling the prosthesis. Sectional Denture A sectional or two-part denture is a type of removable partial denture designed to overcome problems of opposing proximal undercut in relation to unilateral partial denture (Lamine and Laird, 1986; Walter, 1980) It is designed to engage and utilize opposing proximal undercuts on mesial and distal abutment teeth, which will result in positive retention in both vertical and lateral direction often without incorporating a conventional clasp. Each part of the denture will therefore have its individual path of insertion and once in position the part will be maintained in position by means of a locking bolt to form a whole unit. The technical construction of such an appliance is naturally more complex than a conventional denture. This article describes the fabrication of an acrylic sectional denture for a class VI mandibular resection patient who had undergone anterior segmental mandibulectomy with no surgical reconstruction. CASE REPORT A 37 year old female patient presented for removable partial denture replacement of missing
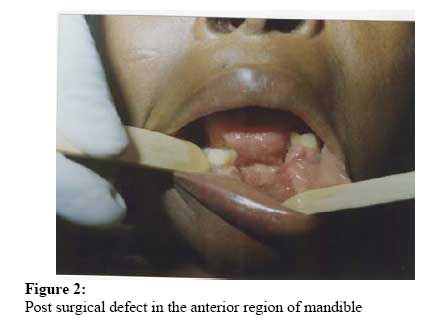
nine months post surgical resection of anterior segment of the mandible. On examination there is discontinuity defect of the anterior part of mandible with independent movement of the lateral segments (fig. 2). The right segment is relatively more stable than the left. The teeth remaining in the mandible were the
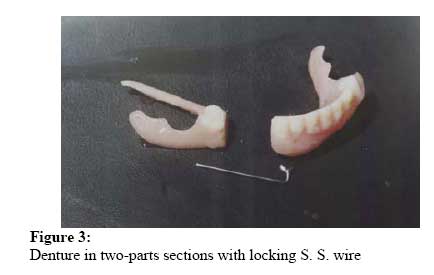
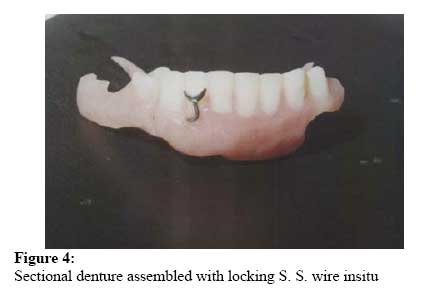
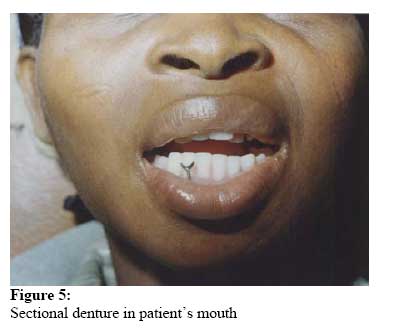
and the resected segment involved the sockets of Surgical reconstruction of the defect and prosthetic rehabilitation were suggested as treatment of choice. However, the patient refused any further surgical intervention because of financial problems. Therefore, it was decided that all acrylic sectional denture would be fabricated for the patient. Clinical and Technical Consideration in Prosthesis Fabrication A plastic stock lower impression tray was cut into two halves and impression of the lower arch was made with irreversible hydrocolloid in two separate sections; each segment of the arch in one-halve of the impression tray. The two halves impressions were poured separately in hard dental stone. The right and left lower arch casts obtained were occluded with upper arch cast and a locating overcast was made to the base of the right and left lower arch cast to align them. A record block was fabricated in wax and the bite registered. The registration of intercupsal position was achieved by manual guidance of the mandible into the required position. Wax trial denture was set up without the right lingual flange and try-in was carried out. The right lingual flanges were later waxed up with the set up trial denture. The whole wax denture was invested and processed in permanent heat cure denture resin. A gutter 2mm deep was then cut on the finished denture about 3mm below the gingival margins of the artificial teeth on the labial surface of the pink acrylic from the region of 3 extending to the flange on the natural standing 6 using a round acrylic bur. A prefabricated stainless steel (S.S.) gingival approaching wire clasp was adapted to the contour of the gutters trough along its length with the Ushaped end terminating on the labial surface of 3. The trough of the gutter and the S. S. wire clasp were coated with a separating medium (Vaseline jelly). Then a self-cure acrylic denture resin was mixed and poured over the wire in the gutter. During the polymerization, the wire was kept free in the trough by rotating, pulling and pushing back the wire in the gutter until the resin is set to create a channel. The excess bulge of acrylic on the labial surface was trimmed off and polished. A rotatory cutting disc was then used to slice this denture obliquely in two halves bucco-lingually between the artificial teeth 5 and 4 without the S. S. wire in position (fig. 3). The cut surfaces were highly polished to allow smooth sliding contact. The adjusted finished denture was inserted in sections. The patient was then asked to close the jaws and the S. S. wire threaded in the channel to lock the two sections (fig. 4). Patient was highly satisfied with the denture and was successfully followed up for 6 months. DISCUSSION The case presented was more challenging due to financial constraints of the patient, which restricted consideration for metal base and tooth support prosthesis and surgical reconstruction of the anterior mandibular defect which could have provided suitable tissue foundation for acceptable prosthesis. The mucosa-borne acrylic sectional denture was made as temporary measure later to be replaced with definitive tooth-borne metal base denture when patient is financially ready. The class VI mandibular resection patients are difficult to rehabilitate with prosthesis because of the independent movement of the lateral mandibular segments. Previous author4,5 have advocated no prosthetic rehabilitation for edentulous patient in this class however, literature on rehabilitation of resected partially edentulous class VI patients is rare. In this case, the two lateral jaw segments move independently and could only align when closed and their standing teeth occlude with upper arch teeth. Hence nothing can be introduced into the mouth as any attempt resulted in severe pain from the TMJ’s and soft tissues. A single lower arch impression was not possible thereby requiring taking the impression of each jaw segment separately. Also, the try-in of the wax trial denture was not feasible which necessitated try-in without the right lingual flanges. Fabrication of denture in the laboratory was less difficult because the models of the right and left mandibular segments have been aligned with a locating matrix. The finished denture was able to be inserted in sections and the two jaw segments allowed to move into occlusion before locking with the adapted S. S. wire. The locked sectional acrylic partial denture stabilized the two jaw segments to open and close (fig. 5). The denture provided gave support to the collapsed lip, restored function, improved the aesthetics and was well tolerated by the patient. REFERENCES
© Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md07027f5.jpg] [md07027f3.jpg] [md07027f4.jpg] [md07027f1.jpg] [md07027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}