 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Biomedical Research, Vol. 11, No. 3, May, 2008, pp. 297-303 Full Length Research Article The Association of Maternal Social Factors and Antenatal Care with Cord Serum Zinc in Full – Term Neonates Lasisi A. O, Kuti M.O., Adekunle A.O. Departments
of Otorhinolaryngology, Chemical Pathology and Obstetrics and Gynecology,
University of Ibadan, Ibadan, Nigeria Received: February
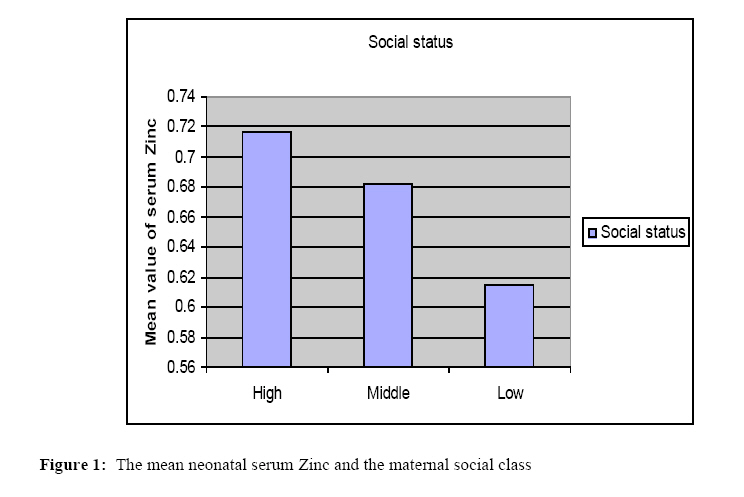
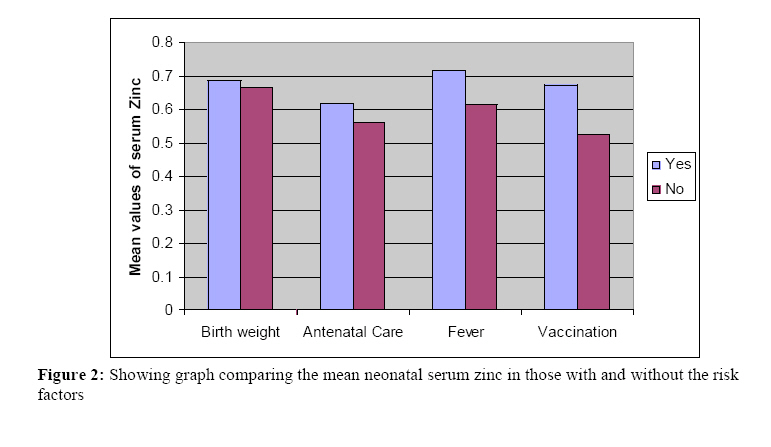
2008 Code Number: md08042 ABSTRACT Zinc is a crucial micronutrient in early childhood survival and the development of innate and acquired immunity. The objective is to determine the relationship between of maternal social class and antenatal care to serum zinc level in newborns in a tertiary and a rural hospital. It is prospective study using questionnaires on consecutive mothers with normal pregnancy(excluding sepsis and chronic illneses) and cord serum level of Zinc estimation in newborns using flame atomic absorption spectrophotometry. There were 106 mothers and neonates; were made up of 57 females and 49 males. The ages of the mother ranged between 21 years to 39 years, with a mean of 26 years; while the gestational age of the neonates ranged between 30 weeks and 45 weeks with a mean of 37.3. The range of the serum Zinc was 0.14μg/L – 0.92μg/L, with a mean of 0.64μg/L (SD=0.17) and median value of 0.63μg/L. The social classes of the mothers were low 66, middle 23 and high 17 with mean neonatal serum zinc of 0.62μg/L, 0.68μg/L and 0.72μg/L. The mean serum Zinc in 17/86 neonates of mothers with inadequate tetanus vaccination was 0.53μg/L, (below the median value) compared to 0.66μg/L in 89/106 neonates of mothers with complete vaccination. The serum zinc in the neonates of mothers <25 years of age was 0.68μg/L compared to 0.61μg/L in the neonates of mothers >25years. Fever in pregnancy was seen in 31/106; with mean neonatal serum Zinc of 0.63μg/L compared with those without fever 0.65μg/L. There were 94 neonates with normal weight (>2.5kg) and 12 low birth weight (<2.5kg) with mean serum Zinc of 0.69μg/L and 0.66μg/L respectively. Antenatal care was complete in 81 and incomplete in 25 with mean neonatal serum Zinc of 0.66μg/L and 0.56μg/L respectively. Univariate analysis revealed significant correlation between the mean serum Zinc and the socioeconomic class (P = 0.022), but there was no correlation with maternal age (P=0.327), sex (P=0.566), gestational age (P=0.100), birth weight (P=0.365), vaccination (P=0.954), malaria fever (P=0.875) and antenatal care (P=0.97), We concluded that low social status of the mothers and inadequate vaccination in pregnancy were major factors associated with low neonatal serum zinc. The control of these factors may impact on optimal neonatal nutrition. Key word: neonates, serum zinc, maternal social classes, antenatal care, association INTRODUCTION There is increasing recognition that micronutrients deficiencies are important determinants of infection and infant mortality rate which is high in most developing countries despite advances in child health care (Lind et al, 2003; Jeswani and Vani, 1991). Zinc is a crucial micronutrient as it influences various aspects of the immune system starting with its effects on the barrier, modulation of the host resistance to several pathogens and various components of innate and acquired immunity (Prasad, 2000; Brown et al, 2002). In addition, severe bacterial illnesses also lead to zinc redistribution (Mahalanabis and Bhan, 2001; Cousins and Lienart, 1988). Supplementation with zinc has been documented to provide protection against common childhood infections like diarrhea and pneumonia in older children (Zlotkin et al, 2003; Dijkhuizen et al, 2001). However, there is limited data on therapeutic effect of zinc supplementation on severe infections in young infants less than 4 months of age (Herman et al, 2002; Froozani and Parsam, 1983). This is an initial report of the serum zinc level in full - term neonates. The objective is to document how the cord serum zinc level of these neonates is affected by the social status of the mothers and other antenatal events. MATERIALS AND METHOD Participants Recruitment Inclusion Criteria: Consecutive mothers with normal pregnancy as judged by the obstetrician. Exclusion Criteria: Pregnant women with history of sepsis, chorioamnionitis and other chronic medical illneses such as asthma, allergy, diabetes, and hypertension. Subjects: Participants were recruited into the study following ethical approval by the University of Ibadan/University College Hospital, Ibadan Ethical Committee (UI/IRC/07/023). Consecutive eligible and consented pregnant mothers in the last trimester of pregnancy were counselled. The participants were pregnant women who had antenatal care, labour and delivery at the University College Hospital and the Bilal Mission Hospital Ibadan. Using oral interview and confirmation in the hospital record chart, the detail of the tetanus vaccination, fever, and antenatal care in pregnancy were documented. At delivery, the duration of labour, fetal weight and gestational age were noted and the cord blood of the neonate was taken from the umbilical vein using a 21G needle and 5 ml syringe, and introduced into a non – heparinized bottle. This was centrifuged at 1500 x g for 10 minutes. After clot extraction, the serum was separated and stored at -80◦C. The sample were analysed for Zinc. Determination of Plasma Zinc: Serum was deproteinised 1 ml to 9 mL of 10% trichloroacetic acid in 0.1% lanthanum solution. Zinc levels were determined in the resultant supernatant using flame atomic absorption spectrophotometry (Model 205 Buck Scientfic, East Norwalk CT, USA 06855). All reagents and materials used for the analysis were free of zinc contamination and the plastics used for the analysis were previously washed with Hydrochloric acid. Statistics: The main outcome variables were the serum levels of retinol in the neonates. Tetanus vaccination was judged adequate if there were 2 doses within 4 weeks to delivery, inadequate if less or none. We depended on self report of fever by the mother, this was assessed as malaria fever if confirmed by the doctor or self - treatment with antimalaria was followed by resolution. Antenatal care was judged adequate if there was no default by the pregnant mother. The socioeconomic class was defined as high (I and II), middle (III) and low (IV and V) based on occupation, income earning and education of the parents11, 12. The data was initially explored using the stata software, variables were analysed by unpaired t-test both for equal and unequal variance using the variance ratio function of the Stata software to determine the appropriate use of the Satterthwaite’s correction for the degrees of freedom. Level of statistical significance was set at p< 0.05 for all the analyses. RESULTS The study included 106 neonates and mothers. The neonates were made up of 57 females and 49 males. The ages of the mother at pregnancy ranged between 21 years to 39 years, with a mean of 26 years; while the gestational age of the neonates ranged between 30 weeks and 45 weeks with a mean of 37.3. The range of the serum Zinc was 0.14μg/L – 0.92μg/L, with a mean of 0.64μg/L (SD=0.17) and median value of 0.63μg/L. The distribution of the social class of the mothers was as follows: Low social class 66, middle 23 and high 17 with mean serum zinc of the neonates in each social class of 0.62μg/L, 0.68μg/L and 0.72μg/L respectively, figure 1. The serum zinc in the neonates of mothers <25 years of age was 0.68μg/L compared to 0.61μg/L in the neonates of mothers >25years. Tetanus vaccination was complete in 89/106 mothers with a mean neonatal serum zinc of 0.66μg/L while it was incomplete in 17/86, with mean of 0.53μg/L. There were 31/106 mothers who had fever in pregnancy, with mean neonatal serum Zinc of 0.63μg/L compared with those without fever 0.65μg/L. There were 94 neonates with normal weight (>2.5kg) and 12 low birth weight (<2.5kg) with mean serum Zinc of 0.69μg/L and 0.66μg/L respectively. The mothers who had incomplete tetanus vaccination were 25/106, with mean serum Zinc of the neonates of 0.56μg/L while 81/106 mothers had complete tetanus vaccination with mean neonatal serum Zinc of 0.66μg/L, figure 2. Univariate analysis revealed significant correlation between the mean serum Zinc and the socioeconomic class (P = 0.022), but there was no correlation with maternal age (P=0.327), sex (P=0.566), gestational age (P=0.100), birth weight (P=0.365), vaccination (P=0.954), malaria fever (P=0.875) and antenatal care (P=0.97), tables 1. TABLE 1: Univariate analysis showing the association between serum zinc and the variables (n = 106)
DISCUSSION The main finding in this study was that maternal social status had a significant inverse association with neonatal serum retinol. In addition, the neonatal serum zinc was below the median value in the neonates of mothers with fever and inadequate vaccination in pregnancy, although this did not show statistical significance. There were no previous reports on maternal social status and neonatal zinc. However, the work of Froozani and Parsam (1983) appeared similar to our finding. They compared the serum level of zinc in cord blood of neonates of 194 women at a public and private Hospitals. Their findings showed that the serum zinc levels in cord blood in the case of the private group were significantly higher (p < 0.01) compared to the public group. In addition, a weak association was observed between umbilical cord blood Zn levels and anthropometric measurements of newborns, like birth weight and head circumference, parity, residence and smoking habits of mothers (Frkovi et al, 1996; Soltan and Jenkins, 1982; Marriott et al, 2007). Szyszko and Czarnowski (2006) studied the effect of social habits of mothers comparing smoking and non-smoking mothers. They found that the ratio of Zinc/Cadmium and Selenium/ lead is higher in all tissues of non-smoking than smoking women, showing tobacco smoke exposure had negative influence on the distribution of the micro-elements in the feto-placental unit. Inadequate vaccination and fever in pregnancy may be features of poor access to optimal health care which are features of low social class. In addition, poor immune status may result in recurrent infection in pregnancy which may lead to neonatal malnutrition. Finding from this study also showed that the serum zinc of neonates of younger mothers (< 25 years) was higher than those whose age are >25 years. Frkovic et al (1996) reported that younger mothers (aged ≤ 25 years) also had higher levels of Zinc in neonatal umbilical cord compared to those whose age was >25 years. It is difficult to postulate which led to the other between intrauterine infection and low neonatal serum Zinc. A vicious cycle of infection and zinc deficiency exists. There was sufficient data from animal and human studies of increased host susceptibility to infections with zinc deficiency (Marriott et al, 2007; Nasrat et al, 1992; Shah et al, 2001). In addition, infection reduces the plasma zinc concentration, which reflects the severity of the infection and inflammation. This might be observed early during the illness in organs such as the skin, thymus, bones and the epithelium which also become depleted during this process. The implication of this report is to study the association of the fetal serum of zinc and other elements and the risk of development of early childhood upper respiratory infections. Soltan and Jenkins (1982) found that cord blood zinc concentrations in congenitally abnormal babies were lower than in the control babies. Hence they concluded that low plasma zinc may be an associated factor in the aetiology of fetal abnormality. Nasrat et al (1992) reported low level of plasma zinc concentration in 10 fetuses with symmetrical growth retardation, but the level was not significantly different from that in the normal control fetuses. However, they concluded that in fetuses with symmetrical intrauterine growth retardation, a low plasma zinc was probably a parallel phenomenon and not necessarily an aetiological factor. Zinc deficiency during fetal development was documented to cause intra-uterine growth retardation and also impaired postnatal immune functions making these babies more susceptible to severe infections (Mukherjee et al, 1984; Shankhar and Prasad, 1998; Bhutta et al, 2000). Studies have shown good correlation between cord blood zinc, maternal zinc concentration and birth weights (Bhutta et al, 1999; Murray and Lopez, 1997). This is critical to demonstrate because nearly 80% of infant mortality occurs in first 2 months of life (Schultink et al, 1997; Abdulla and Suck, 1998; Brooks et al, 2005). Any health programme that aims at reducing infant mortality rate needs to address mortality in the first two months of life. The predisposition of young infants in developing countries to zinc deficiency and infections suggest the need for the addition of zinc to standard treatment of serious bacterial infections may lead to significant improvements in the outcomes. The infant mortality rates in India continued to be in excess of 60 per 1000 live births. Neonatal mortality contributed to over 64% of the infant deaths particularly in those who were born low birth weight. Serious systemic infections like sepsis and pneumonia constituted 30 - 40% of the causes of mortality Abdulla and Suck, 1998). This high prevalence of sepsis is likely to suggest an increased requirement for zinc in the young infants living in the developing countries. This will be needed in order to help in sustaining immunity against the recurrent infections and high microbial load in the environment. In conclusion, our findings suggested that the low social status of the mothers, and inadequate vaccination in pregnancy were major factors associated with low serum zinc in newborns. Further studies are needed to correlate the maternal and neonatal serum zinc status. However, control of these epidemiological risk factors will help in achieving optimal neonatal nutrition. REFERENCES
Copyright 2008 - Ibadan Biomedical Communications Group The following images related to this document are available:Photo images[md08042f1.jpg] [md08042f2.jpg] |
| |||||||||

{kind=link}
{kind=link}