 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 1, 2004, pp. 3-9 REVIEW Pregnancy failure after spontaneous conception or ovulation induction: endocrine causes and treatment Adolf E. Schindler, M.D. Institute of Medical Research and Education, Essen, Germany Correspondence: Prof. Dr. A.E. Schindler, Institute of Medical Research and Education, Essen, Germany, Hufelandstr. 55, D-45147 Essen, Tel.:+49-021-7991833, Fax: +49-021-7499533, Email: schindler@uni-essen Code Number: mf04002 ABSTRACT The spontaneous abortion rate in the general population is about 10%. In some women treated with drug regimens for ovulation induction with or without modern assisted reproductive technology (IVF/ICSI etc.) the rate of pregnancy failure is high. Special attention should be directed towards women with recurrent abortion after spontaneous or stimulated cycles without or combined with methods of ART. Besides the known organic defects of the reproductive system the endocrine abnormalities need to be considered (i.e. corpus luteum insufficiency, disturbances of the luteo-placental shift, trophoblast disturbance). In case of abnormal progesterone and estradiol at the beginning of pregnancy, at the time of the luteo-placental shift or delayed placental endocrine function later in time treatment with progesterone or progestins or estrogen/progestin combinations should be done and the therapeutic effect controlled by repeated progesterone and estradiol measurements. Keywords: Pregnancy, pregnancy failure, habitual abortion, progesterone, estradiol, hCG INTRODUCTION Pregnancy failure; spontaneous and recurrent, is a heavy burden to the parties (wife, husband, doctor) directly involved. These problems are even accentuated when for the achievement of conception ovulation induction with or without various procedures of reproduction have been applied. Procedures to overcome sterility or infertility such as ovulation induction with different regimens with or without modern ART are known to be associated with a higher rate of pregnancy failure than in normal cycling women. Compared with the expected abortion rate of the general population of about 10%(1), the data from 10931 women treated with Clomiphen citrate showed an average miscarriage rate of 24.2% (range 11.4-41.0%) and the data from 2368 women treated with gonadotropins were 23.4% (range 9.4-40.0%)(2). Data from the German IVF register 2001, for example, showed for IVF, dependent on the number of transferred embryos that the average miscarriage rate was 25.7% with one embryo transferred, 18.3% when two embryos transferred and 22.5% with 3 embryos transferred. The data also indicate that there is an increased rate of abortion with increasing age of the women showing for the highest age group between 40-44 years an abortion rate between 32.3 to 66.6%. This increase of spontaneous abortion with ART was also shown recently in 62228 clinical pregnancies between 1996 and 1998 in the USA, where in women over the age of 43 years the abortion rate was 39.3% (3). Furthermore, in women with PCOS miscarriages during the first trimester are reported to be between 30-50% (4,5). Also for recurrent pregnancy loss women with PCOS have a high incidence between 36-82% (4,6) which points towards possible endocrine factors. This is a very likely possibility since correction of the endocrine milieu by metformin and other insulin sensitising drugs, not only improves ovarian function and conception rate but also lowers the abortion rate to 8.8% (4). Such improvements are also found in women with pregnancy loss treated with metformin (change of the abortion rate from 58.3% to 11.8%) (4). Therefore, the endocrine events in the first trimester of pregnancy will be reviewed in order to look for possible critical areas, where endocrine abnormalities could occur and contribute or lead to pregnancy failure and also to obtain indications for endocrine treatment. Rationale for endocrine evaluation and treatment In most animal species and in men progesterone is essential for maintenance of pregnancy (7). Recently, it was reported that estradiol is also crucial for normal pregnancy development (8). It was also shown that women at high risk for subsequent miscarriage had oligomenorrhea and an isolated deficiency of estradiol in the luteal phase of the menstrual cycle (9). In addition, the dominant role of progesterone in pregnancy is due to the fact that progesterone protects the allogenic conceptus from immunological rejection by the mother (7,10). Endocrine events during the first trimester of pregnancy The sources of
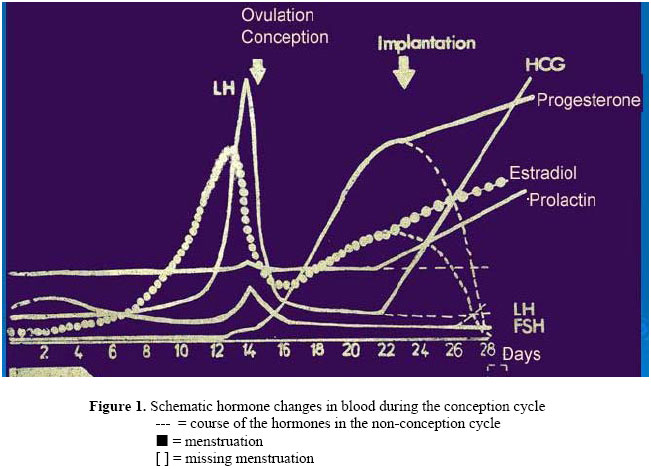
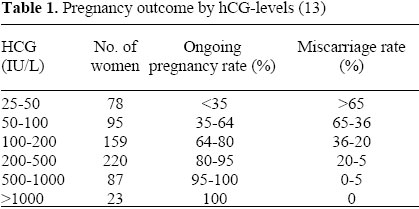
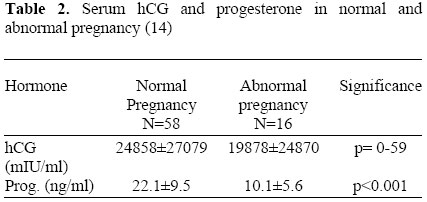
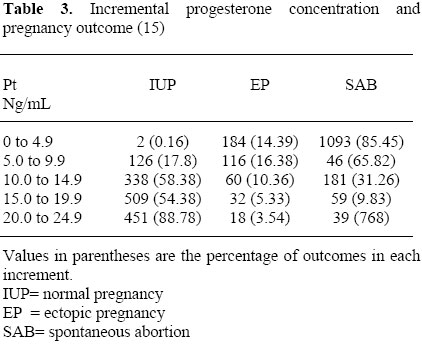
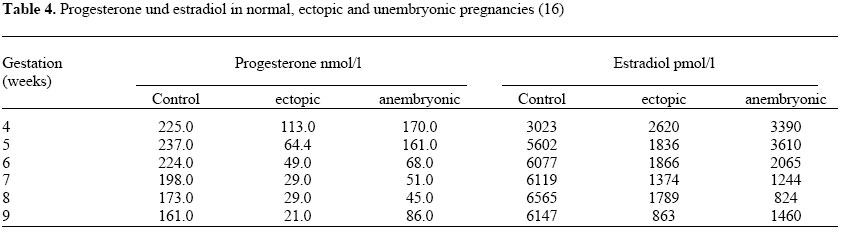
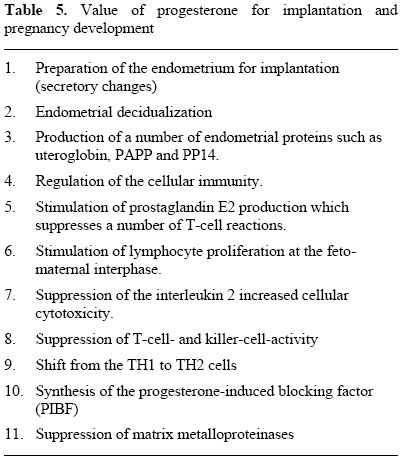
progesterone and estradiol in the first trimester of pregnancy are: Production and secretion of progesterone and estradiol are determined by placental human chorionic gonadotrophin (hCG). hCG can be measured in blood as early as 48 hours after implantation. This is in contrast to HPL, which comes from the same trophoblast tissue and starts to rise in the 7th to 8th week of gestation (11). The early and steep rise of hCG causes the change of the regular corpus luteum to a corpus luteum graviditate with an increase of progesterone and estradiol as well. Parallel to this there is also an increase of prolactin, which most likely is due to the rising steroid concentrations (Fig. 1). It could be demonstrated that at the beginning there is a hCG doubling time of 48 hours. With rising hCG levels the doubling time changes to 72 hours and later to 92 hours as pregnancy progresses (12). Lack of a normal doubling time indicates the following possibilities: 1. Ectopic location of the gestation Indeed, the outcome can be judged early in pregnancy by the concentration of hCG as shown by Homan et al (13) (Table1). The study shows that a single serum hCG measurement 16 days after ovulation is a useful predictor of pregnancy outcome. Later on, the outcome of pregnancies can be better predicted by serum progesterone than hCG as shown in Table 2 (14). Also the incremental increase of progesterone reflects the quality of gestation as shown in Table 3 (15). Abnormalities are also found for estradiol as shown by Johnson et al (16). This is summarized in Table 4. In 1973 Mishell and coworkers (11) showed through continuous measurements of progesterone throughout the first trimester that at first there is an increase of progesterone after implantation. Later on between the 6th and the 10th week of gestation there is not only a plateau but even a decrease which can be farely steep and longlasting in the individual case. The turnaround thereafter is followed by a continuous rise till term in uncomplicated pregnancies. For estradiol there is a more continuous rise with an additional increase around the 6th to 7th week of gestation (11, 17). An explanation for this is the limited life span of the corpus luteum in pregnancy which is reflected at first in a rise of 17α-hydroxyprogesterone following implantation than there is a gradual decrease towards the 7th to 8th week of gestation. This can be explained by the fact that 17α-hydroxyprogesterone is synthesized and secreted by the corpus luteum but not by the placenta. At first, most of the progesterone in early pregnancy is produced by the corpus luteum and placental progesterone comes in later. Therefore, first trimester pregnancy is endocrinologically determined by the luteo-placental shift (18). The importance of the corpus luteum in early pregnancy has been clinically demonstrated by the fact that the removal of the corpus luteum in early pregnancy (before the 8th week of gestation) is followed by abortion (19). In 1972 Csapo and coworkers (20) have shown that luteoectomy causes a steep decrease of plasma progesterone. If the decrease persists at low levels abortion follows; if there is a recovery of the progesterone concentration for instance by treatment pregnancy continuous. According to these findings there is a shift of progesterone production and also estradiol production from the corpus luteum to the placenta. This occurs around the 8th and the 9th week of gestation. Therefore, there exists a functional transition called luteo-placental shift (18,21). Major endocrine events related to spontaneous and recurrent abortions The importance of progesterone for example, for successful implantation and uneventful pregnancy outcome can be understood looking at the multifold action of progesterone in pregnancy as shown in Table 5. According to the data so
far discussed, three endocrine disorders related to spontaneous and recurrent
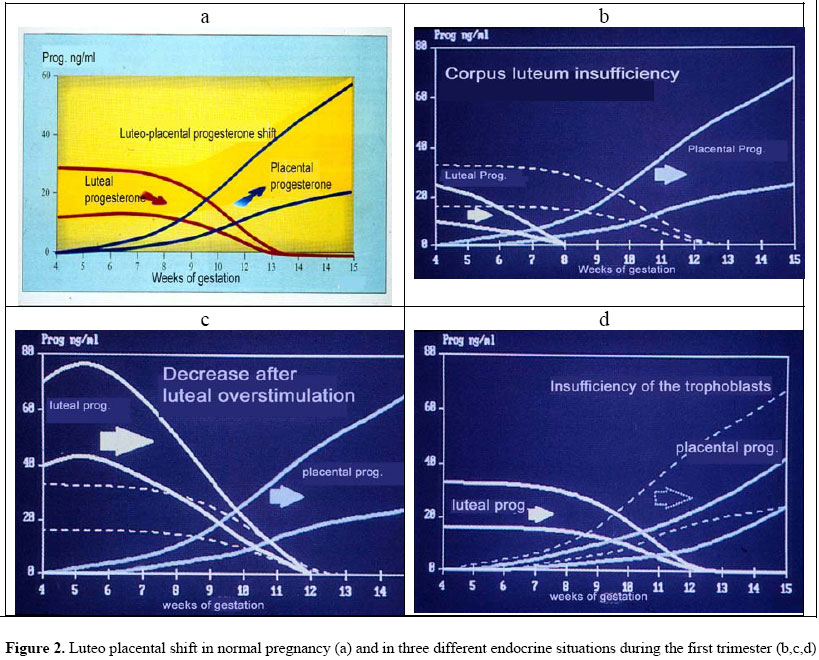
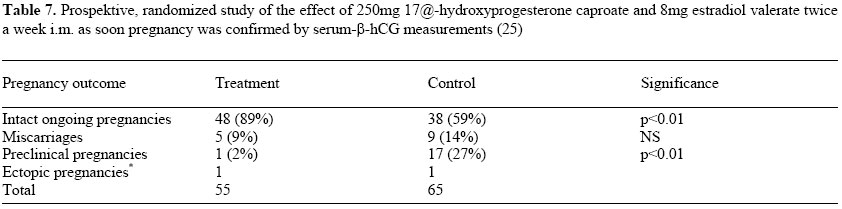
abortions can be differentiated: An overlooked but important point is that in cases with a clomiphene citrate treatment for follicle stimulation the levels of progesterone are even higher than normal to decerne normal from abnormal gestation (30 ng/ml in treated cycles compared with 10 ng/ml in untreated cycles) (22). Therefore, apart from normal pregnancy, three different endocrine conditions in first trimester pregnancy can be postulated as shown in Figure 2 a,b,c,d. In Fig. 2a the normal relationship of progesterone secretion by the corpus luteum and placenta is shown. The transition period lasts from the 7th to the 11th week of gestation. If there is primary corpus luteum insufficiency (Fig 2b) the transition zone last from the 5th to the 8th week of gestation. The values for progesterone are below the normal values and increase later when placental progesterone secretion takes over, if pregnancy continuous. In case of follicular stimulation and ovulation induction there are particular high progesterone and estradiol values, which also decrease as in normal pregnancy, but the decrease is much steeper and even there might be higher values in the normal transition period between the 7th and 11th week of gestation the hormone decrease could lead to a hormone withdrawal and bleeding could be the consequence (Fig. 2c). Recently, the high abortion rate in cases with over-stimulation syndrome, where progesterone as well as estradiol fall from a very high level support this concept (23). The third abnormal endocrine condition could be generated by the delayed and lower progesterone and estradiol biosynthesis by the placenta (Fig. 2d). This delay is sometimes very extensive (23) and could perhaps be the reason of some of the late abortions, since progesterone treatment can prevent premature labour as recently demonstrated (24). The outcome of pregnancy as normal, anembryonic and ectopic gestation is not only related to the course of progesterone but also estradiol as shown in Table 4 (16). This should be taken into consideration when endocrine therapy is done. Hormone treatment of pregnant women with risk of spontaneous and recurrent abortion Treatment possibilities based upon the described endocrine changes in first trimester pregnancy are summarized in Table 6. Various treatment schedules have been reported. One prospective randomized study showed the effect of early start of treatment with a depot preparation containing 250mg 17α-hydroxyprogesterone caproate and 8 mg estradiol valerate twice a week (Gravibinon ®) as soon as pregnancy was confirmed (25). The data are shown in Table 7. One of the clinical indications for estrogen/ progesterone treatment is early low progesterone and estradiol values. This is particular important in women, who had already experienced one or more spontaneous abortions before and one can assume that previous pregnancies ending in abortion were also associated with low hormone values. Defects in hemostasis have to be ruled out (Factor Leyden V, ATIII, Protein C, Protein S)(26). Also antiphospholipid antibodies have to be looked for (27). There are further treatment studies in women with high risk pregnancy conditions which have shown good clinical results with the same hormone preparation (28, 29). Already 1978 Philips and coworkers stated that for a favorable therapeutic effect it is necessary to start the prophylactic progesterone substitution as early as possible (30). Also positive results were reported recently using oral progestin treatment with two times 10 mg dydrogesterone (duphaston®) daily (31). In view of the recent statement (July 2002) by the Royal College of Obstetricians and Gynecologists that the use of immunotherapy should no longer be offered to women with unexplained recurrent miscarriage, one should consider hormone therapy as indicated in pregnancies with early low progesterone and estradiol concentration in women with recurrent/habitual abortion, or women who conceived after follicle stimulation and ovulation induction with or without ART who have rapidly falling progesterone and estradiol levels particularly with the history of abortion in the past. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04002t2.jpg] [mf04002t1.jpg] [mf04002t6.jpg] [mf04002t3.jpg] [mf04002t7.jpg] [mf04002t4.jpg] [mf04002t5.jpg] [mf04002f2.jpg] [mf04002f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}