 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 1, 2004, pp. 31-36 Assessment of the value of ultrasound monitoring and doubling of insemination in clomiphene citrate stimulated IUI cycles Hamdy Azab, M.D.*, Nahed Afify, M.D.† Saudi German Hospital, Aseer, Saudi Arabia* Consultant
of obstetrics and gynecology SGH-Aseer, Lecturer of obstetrics and gynecology,
Kasr El-Ini, Cairo University.† Received
on April 13, 2003; Code Number: mf04005 ABSTRACT Objective: To compare the results of controlled
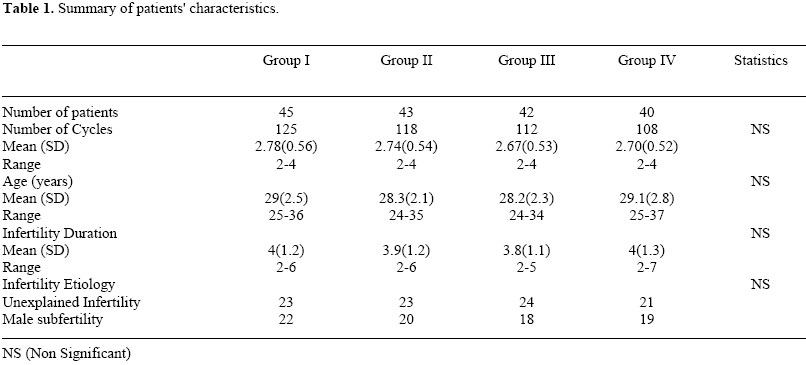
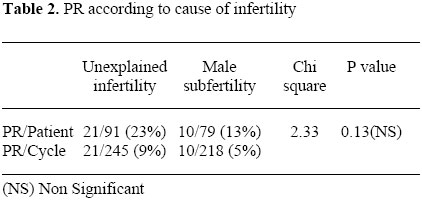
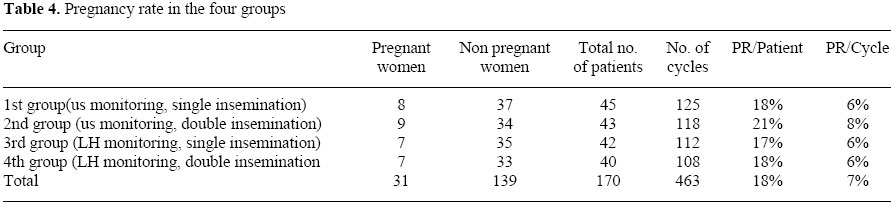
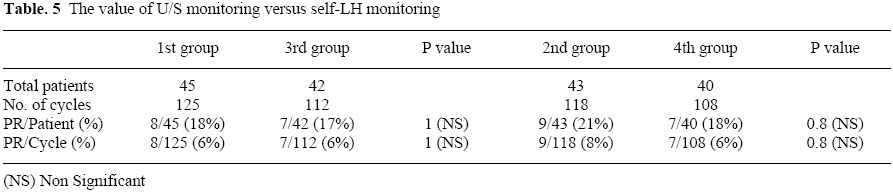
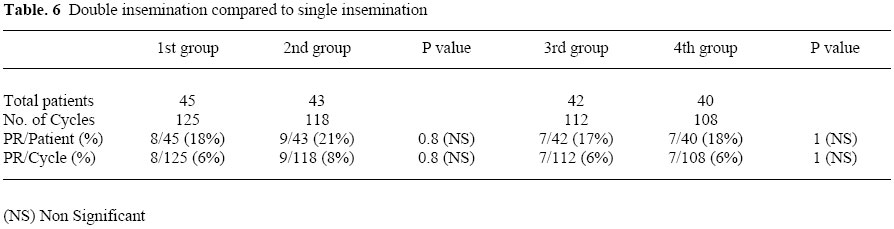
ovarian stimulation and intra-uterine insemination using 4 protocols. Controlled ovarian stimulation together with intrauterine insemination (COS/IUI) is a widely used practice for the management of infertility, particularly for couples with unexplained infertility, male factor infertility, or endometriosis (1-3). COS plus IUI has been found to be more effective for treatment of infertility than either treatment alone (2, 4). Several studies documented that COS/IUI treatment is cost effective for subfertile couples before proceeding to the more invasive and expensive IVF procedures (1, 5). COS using clomiphene citrate (CC) is relatively simple, inexpensive, and safe. The PR per cycle in CC/IUI cycles varies from 6-26% (2, 3, 6). CC has been found to be as effective as gonadotropins for COS in certain population of patients (7). In this study, we are trying to reach a simple and inexpensive protocol as an initial management of infertile couples. We are investigating the value of monitoring of ovulation using vaginal ultrasound versus self monitoring using urinary LH detection kits, at the same time we are checking the value of double insemination versus single insemination. MATERIALS AND METHODS Ninety one couples with unexplained infertility and 79 couples with male subfertility participated in this study during the period from April 2001 until December 2002. The hospital review board approved the protocol of the study. An informed consent was taken from the couples. The age of female partners ranged from 24-37 years with a mean of 28.5 years. All couples had at least 2 years duration of infertility. They had undergone the basic infertility evaluation including history, clinical examination, mid luteal phase progesterone, prolactin assay, and semen analysis. Tubal patency was confirmed by either hysterography or laparoscopy. Women with tubal abnormality were excluded from the study. Unexplained infertility was considered if the results of basic infertility evaluation were normal. Male factor infertility was defined as sperm count < 20 millions/ml, normal morphology < 30 %, or progressive motility < 50 % before sperm preparation. Subjects' characteristics are summarized in Table 1. All women received CC 50 mg tablets twice daily for 5 days starting from the 3rd day of cycle. Women were classified into 4 groups. There was no significant difference among the 4 groups regarding, the age, the duration of infertility, the number of cycles per patient, or the distribution of patients with unexplained infertility and male infertility. In the 1st group monitoring of ovulation was done using transvaginal sonography (TVS) starting from the 10th day of cycle. HCG 10,000 IU was given when the mean diameter of at least one follicle is ≥ 17 mm. Single insemination was then done 36 hours after the HCG shot. The 2nd group was also monitored by TVS and HCG was given as before. Two inseminations were done 20 and 40 hours after the HCG shot. In the 3rd group monitoring of ovulation was done using urinary LH detection kits (Clear Plan) starting from the 10th day of cycle, single insemination was done 24 hours after detection of LH surge. The 4th group was monitored by LH detection kit and double insemination was done 12 and 24 hours after detection of LH surge. The choice of treatment for each couple was based on their preference. The same method was used if the couple had more than one cycle of treatment. Male partners were instructed to collect semen by masturbation after 2-4 days of sexual abstinence. After liquefaction and initial semen analysis, suitable samples were prepared using the density gradient method. SupraSperm system from Medi-Cult (Copenhagen, Denmark) was used. 2 ml of the 55% SupraSperm were dispensed in a centrifuge tube, and then 2 ml of the 80% supraSperm were dispensed beneath the 1st solution. 1 ml of semen sample was added to the prepared gradient. The tube was then centrifuged for 20 minutes at 300g. The supernatant was carefully removed leaving the sperm pellet. The pellet is suspended in 2 ml sperm preparation medium (Medi-Cult) and Centrifuged for 10 minutes at 200g The supernatant was removed and the wash process was repeated. The pellet is then suspended in 0.5 ml of sperm preparation medium. If the count of motile sperms after preparation was less than 5 millions, these couples were excluded from the study and referred to either IVF or ICSI. IUI was done using Wallace (Wallace, Kent, U.K.) IUI catheters, with 1 or 2 ml syringe. With the patient in lithotomy position a speculum was inserted in the vagina. The cervix was cleaned by cotton swab. The IUI catheter was gently passed through the cervical canal. 0.5-2 ml of sperm suspension was slowly injected into the uterine cavity. The patients remained in a supine position for 15 minutes after the procedure. Clinical pregnancy was considered upon the visualization of an intrauterine pregnancy sac using TVS Data were presented in terms of mean, range, standard deviation, and percentage. Comparison between any two groups was done using the Chi-square test with or without Yates correction and Fisher exact test. One way ANOVA test and Chi-square test were used to check for any difference among the 4 groups. P values of less than 0.05 were considered significant. The SPSS (Chicago, IL, USA) and Microsoft Excel computer programs were used for statistical analysis. RESULTS A total of 170 patients underwent 463 cycles with an average of 2.72 cycles per patient. There were a total of 31 pregnancies with an average PR of 18% per patient and 7% per cycle. Of the 31 pregnancies; 27(87.1%), continued pregnancy beyond 16 weeks and 4 (12.9%) resulted in spontaneous abortion. There was only one set of twins (3.2%). There were no ectopic pregnancies. Couples with unexplained infertility had a higher PR (9%) compared to couples with male subfertility (5%). However, this was not statistically significant. Couples with infertility of less than 4 years duration had a significantly higher PR (9%) than couples with infertility of more than 4 years (3%). These data are summarized in Tables 2 and 3. The overall pregnancies for groups I, II, III, and IV were 8 (18% per patient, 6% per cycle), 9 (21% per patient, 8% per cycle), 7 (17% per patient, 6% per cycle), and 7 (18% per patient, 6% per cycle), respectively. These data are summarized in Table 4. The value of U/S monitoring versus self-LH monitoring was assessed by comparing the PR of the 1st and 3rd groups and the 2nd and the 4th groups. Although the women underwent U/S monitoring had a higher PR, yet the difference was not statistically significant. Similarly, double insemination did not yield a significanthigher PR compared to single insemination, as evident by comparing the 1st and 2nd groups and the 3rd and 4th groups. These data are summarized in Tables 5 and 6. DISCUSSION COS and IUI is a widely used practice for management of infertility being simple and relatively inexpensive approach. In this study we are trying to reach a simple approach for the management of unexplained infertility and male factor subfertility. Patients with unexplained infertility have undergone basic infertility evaluation; however, not all of them had laparoscopy or analysis of the possibility of immunological factors. Based on this, the cause of unexplained infertility in some patients can be related to early stage endometriosis. We analyzed the value of U/S monitoring of ovulation versus self urinary LH monitoring and the value of increasing the frequency of insemination. Although the PR was higher with U/S monitoring, yet the difference was not statistically significant. Zreik et al, (8) have found that U/S monitoring and induction of ovulation using HCG did not yield a higher PR when compared to urinary LH monitoring, which is matching with our conclusion. In a retrospective study by Deaton et al, (9) they found that the success of IUI with CC is not dependent on the method used to establish the timing for the IUI. They concluded that U/S monitoring of ovulation has no advantage over urinary LH monitoring. Moreover, Martinez et al, (10) found that waiting for endogenous LH surge may have an advantage over triggering ovulation by HCG. They suggested that this allows full natural maturation to occur. However, Awonuga et al, (11) found no value for waiting spontaneous LH surge. Our results and the mentioned studies are in common suggesting that urinary LH monitoring is as effective as U/S monitoring in this population of IUI patients. There is controversy in the literature about the value of double insemination compared to single insemination. Silverberg et al, (12) were the first to address a significant value of double insemination in a prospective randomized study. Ransom et al, (13) in another prospective randomized study found that increasing the frequency of insemination does not provide a significant increase in cycle PR. Ragni et al, (14) found that two IUIs performed 12 hours and 34 hours after HCG administration is the most cost-effective regimen for women undergoing COH cycles with clomiphene citrate and gonadotropins. The authors suggesting value of double insemination refer this to optimizing the window of ovulation taking full advantage of sequential ovulation. In our study we used CC only for induction of ovulation so the value of sequential ovulation of multiple follicles is denied. We have found no significant value of double insemination which seems to be logic among this population of patients stimulated by CC. Our results demonstrated a significant increase in PR in women with infertility duration of less than 4 years (9%) compared to women with infertility of 4 years or more (3%). This is in accordance with the results of Nulsen et al, and Tomlinson et al (15-16). However, other studies found no relation between the duration of infertility and the likelihood of pregnancy (3, 17). Regardless of the variability in the literature, CC stimulated IUI cycles can not be recommended for women with long standing infertility. We found a higher PR in couples with unexplained infertility (9%) compared to couples with male factor subfertility (5%); however, the difference was not statistically significant. Previous studies showed a PR ranging from 6-26% in women with unexplained infertility (2, 3, 6) and a PR of 3-5% in couples with male subfertility (2, 18, 19). Several studies (20-23) achieved a higher PR in male subfertility. We applied post preparatory threshold value of 5 million motile sperms to be included in the study. The higher PR in these studies could be due to the use of a higher threshold total motile sperm count and/or the use of gonadotropins for stimulation.Finally, this study shows that women with unexplained infertility or mild male factor abnormality and of infertility duration less than 4 years will have a good chance with CC stimulated IUI cycles monitored by self urinary LH and employing single insemination. Couples with long standing infertility or severe male defect need a more aggressive approach. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04005t6.jpg] [mf04005t1.jpg] [mf04005t2.jpg] [mf04005t5.jpg] [mf04005t4.jpg] [mf04005t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}