 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
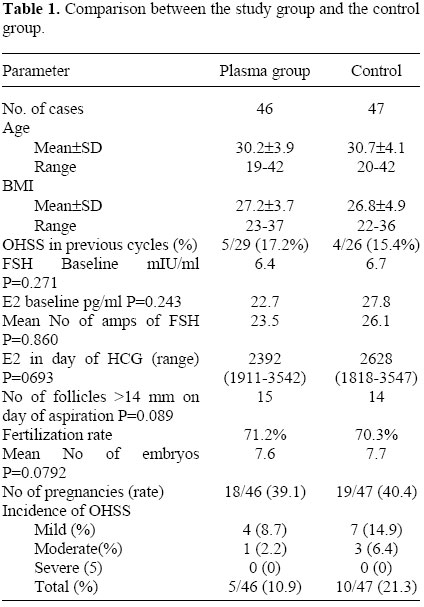
Plasma transfusion on the day of oocyte aspiration may reduce ovarian hyperstimulation syndrome in patients with polycystic ovary Yousef M. Alhelou, M.Sc.,Tharwat Y., Alhelou, M.D., Ghada S. Alkerenawi, B.Sc., Sandra N. Akela, B.Sc. The ART center, AlhelouInternationalHospital, 177-50 Nasser Street, Gaza city, Palestine. Correspondence: Yousef Alhelou, Alhelou International Hospital, 177-50 Nasser street, Gaza city, Palestine. Fax: 970 8 2840 663, Email: alhelou@yahoo.com Received
on January 20, 2003; Code Number: mf04006 ABSTRACT Objective: To determine the efficiency of plasma
transfusion on the day of oocyte aspiration in preventing ovarian
hyperstimulation syndrome (OHSS) in polycystic ovary (PCO) patients undergoing
ART cycles. Key Words: OHSS, PCOS, Plasma, ART, ICSI The polycystic ovary syndrome (PCOS) was first presented by Stein and Leventhal in 1935 (1). PCOS is characterized by infertility, hyper-androgenism, anovulation, acne, hirsutism (2), and insulin resistance (3). It affects about 6% of premenopausal women (4,5). The exact etiology of PCO remains to be clarified, but genetic factors have been proposed (6-8). Ovarian hyperstimulation syndrome (OHSS) is the most serious complication in PCO patients who are treated with exogenous gonadotrophins, it occurs in about 1%-10% of all ART cycles (9). OHSS has many complications such as cerebrovascular problems (10,11), liver dysfunction (12,13), renal complications (14), respiratory complications (15), gastrointestinal complication (10,16), ectopic pregnancy (17), peritonitis and perforated appendicitis (18). Many strategies have been proposed to reduce the incidence of OHSS in high-risk patients, non of them are completely effective, such strategies try to modify the overstimulated cycle, they include reduction in ovulation dose of HCG (9), prophylactic administration of albumin (19,20), ascitic fluid aspiration (21), cryopreservation of embryos and withholding gonadotrophins to allow E2 levels to decrease before HCG administration, coasting (22-24), administration of methylprednisolone (25) and administration of GnRH agonist to induce ovulation instead of HCG after GnRH antagonist ovarian stimulation (26). In our study, we present the results of plasma administration as a technique for reducing the incidence and degree of OHSS. MATERIALS AND METHODS Patients From February 2000 to November 2001, a total of 93 patients undergo ICSI with the female partner has PCOS and are at risk of OHSS. The cases with high risk were diagnosed by the presence of enlarged polycystic ovaries with more than 10 cysts, 2-8 mm in diameter scattered either around or throughout an echodense thickened central stroma and high levels of E2 (> 2500 pg/ml) on the day of HCG administration (27,28). Stimulation protocol and ICSI procedure Ovarian stimulation was carried out as described elsewhere (29). Briefly, pituitary desensitization was initiated with Triptorelin (Dipherelin 3.75 mg, Beaufour Ispen International, France), which was administrated intramuscular (I.M) in the midluteal phase of the previous cycle. Human urinary follicle stimulating hormone (FSH) 150-225 IU (Follitrin, Massonie, Argentina) was injected from day 2-3 of menstrual cycle, injection of FSH continued till day of human chorionic gonadotrophin (HCG) administration. The patients received 7500 IU of HCG (Gonacor, Massonie, Argentina) when 2 or more of the leading follicles had reached the diameter of 18 mm and after one day of coasting. Transvaginal oocyte retrieval and preparation was carried out as descried elsewhere (30), the partners' semen analysis was collected in a sterile container after masturbation. Sperm parameters were assessed by established procedure (31,32). The ICSI procedure was performed on MII oocytes as described elsewhere (33). Fertilization was examined 16-22 hours after injection, embryo quality and cleavage were assessed 24 hours later (30). The luteal phase was supported with progesterone (Cyclogest, Cox pharmaceuticals, UK) 400 mg twice daily, vaginally for 14 days. 1-3 units of plasma with the same blood group of the patient were transfused in patients who are at risk of OHSS. Written consent was obtained from all participants. All patients underwent the same controlled ovarian stimulation protocol. After oocyte recovery, randomization took place on an alternative basis. The patients either received 1-3 units of plasma intravenous (i.v.) or did not receive plasma (control). The patients were followed for the signs of OHSS, the symptoms of OHSS were classified as early or late and graded mild, moderate or severe according to the standard OHSS criteria. Ninety-three cases were randomized in total, 46 cases received plasma, 47 cases were used as control and did not received plasma. There was no significant difference in the demography of the two groups. One unit of plasma was given for cases with E2 level less than 2000 pg/ml on day of HCG, two units were given for case with E2 level between 2000 pg/ml and 3000 pg/ml on day of HCG, and three units were given for patients with E3 level higher than 3000 pg/ml on day of HCG The plasma group is presented first (Table 1). Mean age 30.2 (range 19-42) SD 3.9 versus 30.7 (20-42) SD 4.1, mean body mass index (BMI) 27.4 (range 23-37) SD 3.7 versus 26.8 (22-36) SD 4.9, and past history of OHSS in a previous cycle (5/29) 17.2% versus (4/26) 15.4%. The baseline for FSH 6.4 mIU/ml versus 6.7 mIU/ml, P=0.271, baseline E2 22.7 pg/ml versus 27.8 pg/ml, P=0.243. The mean total number of ampoules of FSH received 23.5 versus 26.1, P=0.860. There was no difference in the number of days coasted. E2 level on HCG day 2392 pg/ml (range 1911-3542) versus 2628 pg/ml (1818-3547), P=0.693, the number of follicles before aspiration >14mm is 15 versus 14, P=0.089. RESULTS Fertilization rate was 71.2% versus 70.3%, P=0.0871. The mean number of embryos formed was 7.6 versus 7.7, P=0.0792. There was no significant difference in pregnancy rate (18/46) 39.1% versus (19/46) 40.4%. There was a noticeable difference in the two groups related to the occurrence of OHSS, the plasma group had 4 mild 8.7% and 1 moderate 2.2%, total % 10.9, where as 7 mild 14.9% and 3 moderate 6.4%, total % 21.3 in the no plasma group, all were early onset of OHSS. None of the plasma group showed early or delayed transfusion reaction. DISCUSSION The polycystic ovary appearance occurs in 20% of normal women and in 40% of patients undergoing ART irrespective of the indication for treatment (34). The underlying mechanism responsible for the clinical manifestation of OHSS appears to be an increase in capillary permeability of the mesothelial surface with acute fluid shift out of the intravascular spaces (35), which results in the development of massive extravascular exudates (34,36) in the peritoneal and plural cavities causing a protein-rich ascites (34). It is believed that this fluid shift begins one day before the oocyte aspiration (37). High circulating concentrations of E2 are immediate predictor of OHSS, but they are not the cause of vascular permeability. Many compound have been proposed to mediate the capillary permeability such as estrogens, the ovarian renin angiotensin system, prostaglandins, vascular endothelial growth factor (VEGF), interleukins, angiognin (38,39) and kallikareins (34). The two main candidates that are thought to have strong influence on capillary permeability are the activation of the ovarian renin angiotensin system and the release of VEGF from the ovary. The follicle contains renin in an inactive form which is activated upon exposure to HCG and which then cause the conversion of angiotensinogen to angiotensin I (34). Loss of fluid into the extravascular space cause a profound fall in intravascular volume, hemoconcentration and suppression of urine formation, loss of protein from intravascular spaces cause a fall in plasma oncotic pressure which results in a further loss of intravascular fluid. Secondary hyperaldosteronism occurs and cause salt retention, and eventually peripheral edema develops (34). It was mentioned previously that prophylactic administration of albumin might reduce OHSS (19,20). The human plasma contain 6.0-8.2 g/dL of total protein and 3.5-5.2 g/dL of albumin (40), Albumin is the plasma protein that contribute most to oncotic pressure because of its high plasma concentration and relatively low molecular weight (41) and it is established that protein affect the distribution of extracellular fluid between vascular bed and interstitial fluid by means of oncotic pressure they generate (40). As a result, plasma administration to patients at risk of OHSS enhances protein and albumin concentration which may reduce fluid shift from intravascular space to extravascular space, in addition, plasma may compensate some of fluid loss, if occurs, due to its high content of water and electrolytes. Furthermore, plasma is not expensive. CONCLUSION Our study proposes that plasma administration may reduce the percent and degree of OHSS in PCO patients undergoing ART, Plasma administration has no effect on the pregnancy rate. REFERENCE
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04006t1.jpg] |
| |||||||||

{kind=link}