 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 1, 2004, pp. 47-57 Ovulation prediction in spontaneous and induced cycles: the role of ovarian reserve markers Amgad O. Gohar, M.D., A.R. El-Edwi, M.D., Hossam ELDin S.H. Abdallah, M.D. Department of Obstetrics and Gynaecology, Faculty of Medicine, El Minia University, El Minia , Egypt . Correspondence and reprint request: Dr. AmgadOsmanGohar, Dept. of Ob Gyn. El Minia University Hospital, El Minia , Egypt , E-Mail: Amgad_gohar2003@yahoo.com Received on September 17, 2003; Code Number: mf04008 ABSTRACT Objective (s): To evaluate the role of day 3 serum; FSH,
inhibin-B and estradiol, (biochemical markers),
ultrasound measured antral follicle count AFC and
ovarian volume OV (biophysical markers) in ovulation prediction in induced
cycles in infertile patients with different induction protocols. Also, the
secondary aim was to analyze the correlations between these markers and
prediction of ovulation success in induced cycles with different induction
protocols. Key words: Ovulation prediction, FSH, Inhibin-B, estradiol, transvaginal ultrasound, antral follicle count AFC, ovarian volume OV, Infertility “Ovarian reserve” describes the native oocyte endowment and is closely associated with reproductive potential. As a diagnostic entity, ovarian reserve screening developed from clinical experience with the advanced reproductive technologies. Diminished ovarian reserve generally presages a poor response to any fertility treatment, and sharply limits the possibility of successful pregnancy. Screening for the ovarian reserve is a fundamental component of the initial infertility evaluation, since it is a key determinant of what, if any, treatment should be offered. A number of tests have been described that attempt to best assess ovarian reserve (1). The concentration of circulating FSH on the third day has been recognized as a marker of ovarian reserve and important predictor of the ovarian response to hormonal stimulation and IVF outcome than age (2). However, some clinicians have questioned the usefulness of widespread FSH screening because of the difficulty in establishing absolute FSH breakpoints compatible with achieving pregnancy (3). It has been suggested that the serum measurement of Inhibin B concentration in the early follicular phase may be of value in the assessment of "poor responders" to IVF treatment (4).However, it has been concluded that, so far as for clinical usefulness, it remains a horizon topic because of the lack of a satisfactory assay to quantify it (4-9). Early follicular estradiol levels may reflect cycle dynamics and the likelihood of conception (2).A number of studies have examined the estradiol levels on day 3 of the cycle as an independent risk factor in IVF cycles, with the general findings that cycles are more likely to be cancelled because of poor stimulation, oocytes retrieved are fewer, and pregnancy rate are lower when estradiol values exceed 60 pg/ml, in one study and 80 pg/ml in the other two (10-12). Since the loss of ovarian reserve is functionally related to fewer primordial follicles available for gonadotropine recruitment, ovarian imaging via transvaginal ultrasound has been used to gain a direct assessment of gonadal status and activity both before and during fertility treatment (1). There is currently much interest in determing the size of the growing follicular pool (13).Antral follicle count AFC assessment as a tool for predicting outcome in IVF has been suggested. Day 3 FSH, maternal age and antral follicle assessment were found to be strongly related to IVF outcome. Pregnancy rate was significantly higher in the group with antral follicle >6 compared to that in the group with the antral follicle < 6. It has been concluded that antral follicle assessment was a better predictor of IVF outcome than age or FSH. Antral follicle assessment may provide a marker for the ovarian age that is distinct from chronological age or hormonal markers (14). Also, ultrasonic measurement of the ovarian volume OV as an indictor of reproductive success had been suggested (15, 16).A significant correlation between pretreatment ovarian volume and gonadotropin dosage required to detect ovulation induction, follicular yield, and oocyte recovery has been found (17).Yet, it has been concluded that, a confirmation is needed in order to determine if this is a reliable index of ovarian function (18). The aim of the work was to evaluate the role of day 3 serum; FSH, inhibin-B and estradiol (biochemical markers), ultrasound measured antral follicle count AFC and ovarian volume (biophysical markers) in ovulation prediction in induced cycles in infertile patients with different induction protocols. Also, the secondary aim was to analyze the correlations between these markers and prediction of ovulation success in induced cycles with different induction protocols MATERIALS AND METHODS Eighty patients attending the Infertility clinic of El Minia University Hospital with primary or secondary infertility and with otherwise normal complete infertility work-up (study group) together with 20 fertile subjects matched for age, weight and body mass index (BMI) and using local methods of non-hormonal contraception recruited from The Family Planning Clinic (control group) were included in the study which was done from September 2002 to August 2003. The ages of the subjects were between 35-38 years with a duration of infertility of at least two years and normal menstrual cycle (range 24-35 days).Exclusion criteria were, smoking, endometriosis, the presence of only one ovary or previous ovarian surgery, polycystic ovary syndrome, positive Chlamydia infection, or other endocrine or medical disorders, exposure to study drugs or other ovulation induction drugs within 3 months of participation in the study. Those women with male partners having a total sperm concentration < 20 million/ml, with sperm motility and normal morphology < 40 % (19), were excluded from the study. The study group was further subdivided into four groups according to the method of ovulation induction. Group I: (Clomiphene Citrate; CC group) including 20 patients receiving clomiphene citrate (Clomid, Epico, Egypt) oral tablets (50- 200 mg /day for 5 days) starting on the third day of the menstrual cycle. Group II: (Human urinary FSH, u-FSH group): including 20 patients
receiving human urinary FSH (Meterodin HP,
Group III: (Low dose recombinant Follicle stimulating hormone; rFSH group): including 20 patients receiving recombinant
FSH (Puregon,
Group IV: (IVF group) including 20 patients receiving the long protocol of IVF. IVF protocol was performed as described by Harrison et al., (20, 21) and Gordon et al., (22) in IVF center. An informed consent was taken from each participant after careful explanation of the purpose and the procedures of the study. Methods Complete history and examination were done to all participants.In day 3 of the normal menstrual cycle, all participants were subjected to blood sampling for measurements of serum inhibin-B, FSH, estradiol and ultrasound measurement of the antral follicle count AFC and ovarian volume OV. Blood sampling and Hormonal assays Blood samples for screening markers (FSH, Inhibin- B and Estradiol) were withdrawn from the ante-cubital vein at
Blood samples were allowed to clot; serum was separated, labeled and stored in -40 C° for subsequent assays. B- Inhibin was measured in duplicate using two-site enzyme linked immunosorbents assays ELISA (Serotech Limited, Kindlington, Oxford, UK) using plates coated with specific monoclonal antibodies.Theinhibin-B assay cross-reacts approximately 1% with inhibin-A. Assay sensitivity for inhibin-B was 16 pg/ml. Inter- and intraplate coefficient of variations were both <7 %. Estradiol and progesterone were analyzed using solid phase
radio-immunoassay technique RIA technique (Diagnostic Products,
Serum concentrations of FSH and LH were measured using Immulite chemiluminescent assay kits ( DPC, Glyn Rhonwy, Llanberis, Gwynedd, UK).The detection ranges of FSH and LH were 0.1 -170 and 0.7-400 mIU /ml, respectively. All hormone analyses were done under the supervision of an investigator unaware of the diagnosis. The cut off limit for FSH was 10 m IU/ml (normal <10 m IU/ml;
abnormal ≥10 m IU/ml) (cycle day # 3 criteria of
Georgia Reproductive Specialists,
Ultrasound Transvaginal ultrasound was done by 6.5 MHz sector transducer,
(model 415 EUB, Hitachi Med. Corp,
Follow up All patients were followed up by follicular monitoring with vaginal ultrasonography and serial measurement of E2 and LH starting on the 8th day of the cycle and then every other day until HCG (10,000 IU, Pregnyl; NV Organon, OSS, the Netherlands) was administered as a single I.M injection to trigger ovulation when at least one follicle ≥ 18 mm. Cycles were cancelled if the ovarian response was poor with < 3 follicles at day 8 of the cycles. Endometrial thickness was measured at the greatest diameter perpendicular to the mid-sagittal plane in the fundal region, including both layers of the endometrial cavity. The image was oriented so that, the endometrial canal and the cervical canal were visualized in the same plane to ensure measurement through the center of the endometrium as recommended by Gonen andLuteal phase was supported in documented ovulatory patients in the
study group by progesterone suppository 50 mg daily or minimally three
injections of 1500 IU hCG for at least two weeks. Biochemical pregnancy was
defined as a positive urinary pregnancy test (Clearview,
hCG II, Unipath Ltd, Bedford,
Statistical Analysis Results were expressed as means ± SD for quantitative characteristics and number and percentages for qualitative characteristics. Statistical comparisons were made using Chi-square χ2 test or Fisher exact test for qualitative characteristics when appropriate. Unpaired data were compared using the non-parametric Mann-Whitney U test. One way analysis of variance ANOVA was used to compare the numerical results among different groups. Pearson's correlation analysis was carried out to study the relationship between biochemical markers (FSH, inhibin-B and E2) and biophysical markers (Antral follicle count AFC and ovarian volume OV). Multivariate regression analysis was used in a stepwise fashion to test the relative significance of different biochemical markers (FSH, inhibin-B and estradiol) or biophysical markers (AFC and OV) in relation to ovulation. Statistical analysis was performed on an IBM personal computer
using SPSS statistical package for windows (SPSS, Inc,
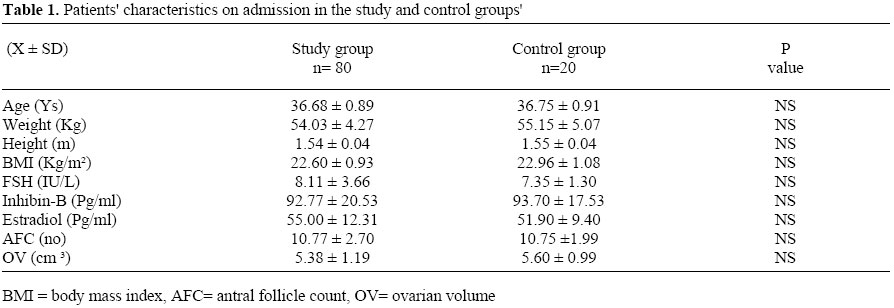
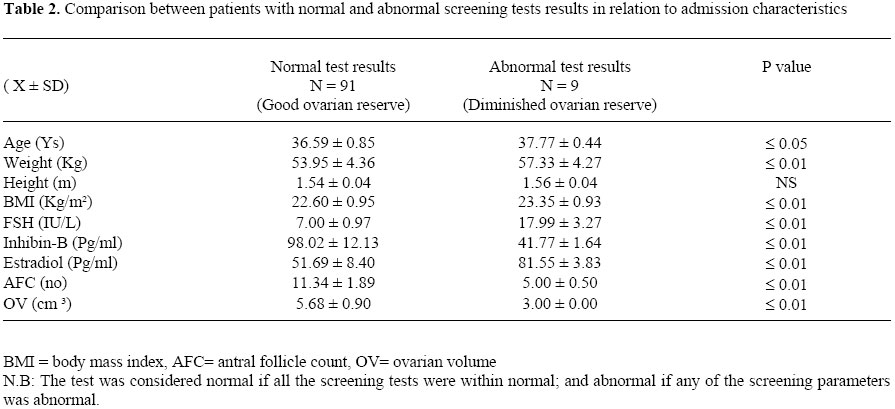
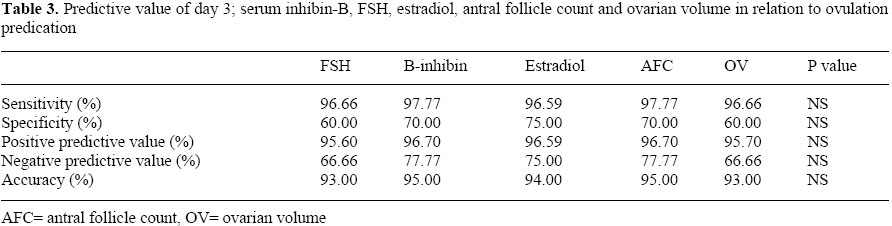
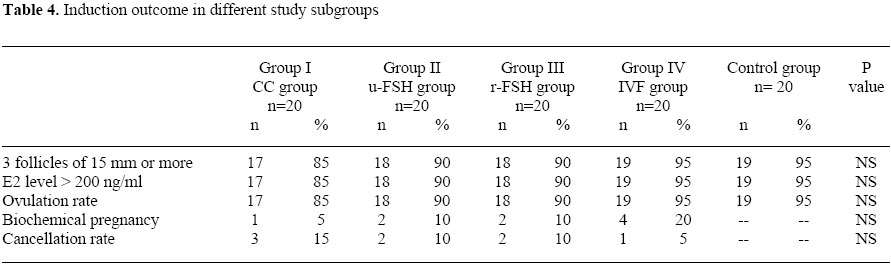
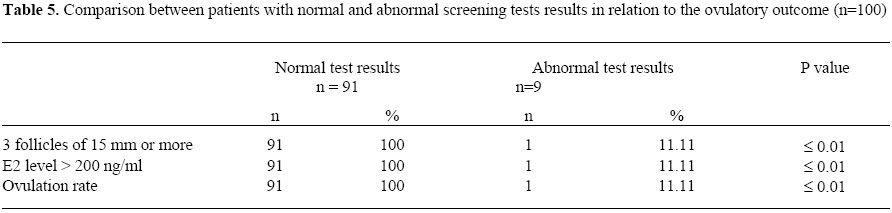
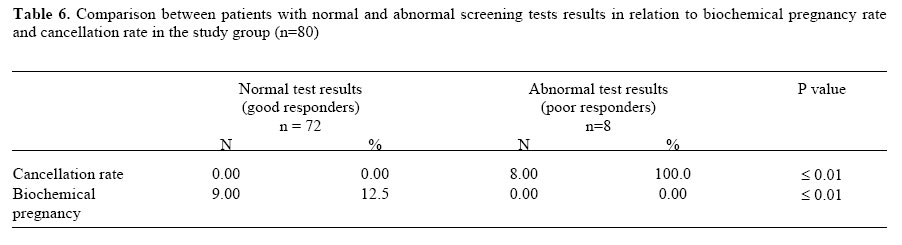
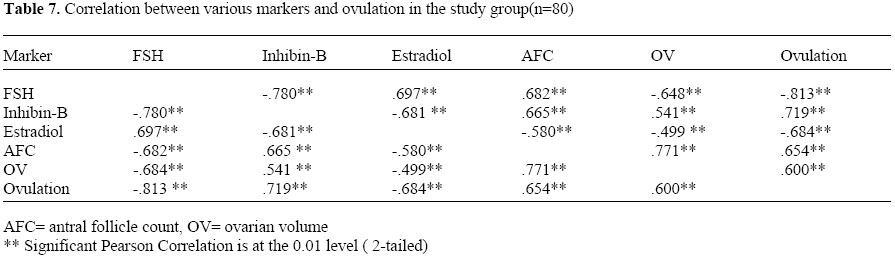
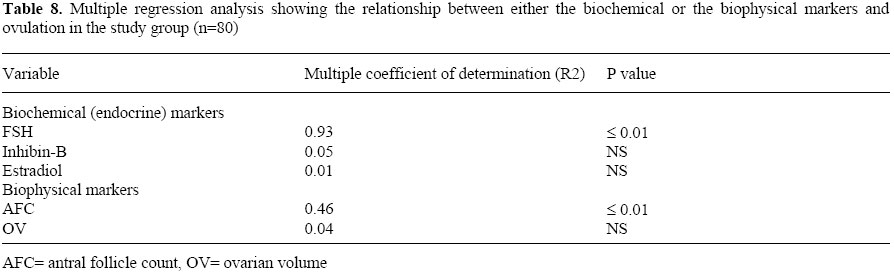
RESULTS Patients' characteristics on admission in the study and control groups are summarized in Table 1. There was no statistically significant difference between the study group and control group regarding age or weight or height or BMI. Biochemical (FSH, inhibin-B and estradiol) and biophysical markers (AFC and OV) were comparable in both groups (8.11± 3.66, 92.77 ± 20.53 and 55.00 ± 12.31) & (10.77 ± 2.70 and 5.38 ±1.19) Vs (7.35 ± 1.30, 93.70 ± 17.53 and 51.90 ± 9.40) & (10.75 ± 1.99 and 5.60 ± 0.99), respectively (P > 0.05) (for each). Table 2 shows comparison between patients with normal and abnormal screening tests results in relation to admission characteristics. Age was significantly higher in patients with abnormal test results (poor ovarian reserve) compared with those with normal test results (good ovarian reserve) (37.77± 0.55, # 36.59 ± 0.85, P ≤ 0.05). Weight, BMI, FSH and estradiol were significantly lower in patients with normal test results compared with patients with normal test results (P≤ 0.01) (for each). Inhibin-B, AFC and OV were statistically higher in patients with normal test results compared with those with abnormal test results (P ≤ 0.01) (for each). The predictive values (sensitivity, specificity, positive predictive value, negative predictive value and accuracy ) in relation to ovulation prediction of FSH (<10 IU/L), serum inhibin-B ( > 45 pg/ml), estradiol (< 75 pg/ml) antral follicle count (> 6) and ovarian volume (> 3 cm≥ ) were statistically comparable (P > 0.05) (Table 3) Ovulation rate, number of follicles (> 3) greater or 15 mm in diameter on the day of hCG administration, peak estradiol level of > 200 ng/ml in response to different induction drugs were comparable among different study subgroups and compared with the control group (P > 0.05) (for each)(Table 4). Ovulation rate, number of follicles (> 3) greater or 15 mm in diameter on the day of hCG administration, peak estradiol level of > 200 ng/ml were significantly higher in patients with normal test results (good ovarian reserve) compared to those with abnormal tests (diminished ovarian reserve) (P ≤ 0.01) (for each, respectively, n=100) (Table 5). Eight poor responders (10%) were found in the study group (n=80) (Three in group I, two in group II, two in group III and one in group IV).All of them were with abnormal screening test results. In each study subgroup, all responders received the same average drug dosage. The dosage was found to be increased only in poor responders. Cancellation rate was significantly higher in patients with abnormal test results compared to those with normal test results in the study group (P ≤ 0.01, n=80). Biochemical pregnancy rate was significantly higher in patients with normal test results compared to those with abnormal test results in the study group (n=80) (P≤0.01) (Table 6). Ovulation was significantly correlated to the levels of FSH (r =-, 813, P ≤ 0.01) inhibin-B (r =.719, P ≤ 0.01) estradiol ( r = -,684, P ≤ 0.01), AFC (r =.654,P ≤ 0.01) and ovarian volume ( r =.600, P ≤ 0.01) in the study group (n= 80) (Table 7). Multivariate analysis of the variables that predict ovulation in induced cycles demonstrated that ;of the biochemical variables FSH was the most significant contributor to ovulation ( R2 = 0.93 P ≤ 0.01),while of the biophysical variables AFC is the most significant one ( R 2= 0.46, P ≤ 0.01). (Table 8) DISCUSSION Screening for the ovarian reserve is needed. Resisting the temptation to obtain all possible tests for the ovarian reserve should be done by clinicians for better interpretation of their results (18). In this study the predictive values ( sensitivity, specificity, positive predictive value, negative predictive value and accuracy) of day 3 serum inhibin-B ( > 45 pg/ml) were in agreement with Seifer et al., (4), who observed that when the day 3 serum inhibin-B titer was < 45 pg/ml, the response to gonadotropine stimulation was blunted, the cancellation rate was higher, the number of retrieved oocyte was lower, and the pregnancy rate was significantly reduced in a comparison with subjects whose day 3 inhibin-B values were ≥ 45 pg/ml. Also, this is in agreement with Smith et al., (24) who found that day 3 serum inhibin-B and estradiol are the best predictors of success in assisted reproductive technologies. It was noticed that the rise in early follicular FSH with reproductive aging correlates with the fall in inhibin-B levels (25). Hofmann et al., (7) confirmed that women with diminished ovarian reserve had lower inhibin-B levels and they postulated that this may be due to reduced granulose cell inhibin-B production. Furthermore, it was postulated that the earliest demonstration of diminished ovarian reserve may be reflected by a decrease in day 3 inhibin-B levels before a significant rise in day 3 serum FSH (26). Unfortunately, determination of inhibin-B had been criticized by the lack of a satisfactory assay to quantify it (4-9). Also, several recent studies failed to find clinical value in measuring basal inhibin-B levels with regard to IVF outcome (8, 27, 28).Perloe et al., (1), in their review of the current inhibin-B status in evaluation of the ovarian reserve concluded that although these early reports confirm that inhibin-B can extend the sensitivity of ovarian reserve screening, more data are needed before meaningful normal ranges of inhibin -B can be applied routinely in clinical practice (27-30). The predictive values of FSH in this study (<10 IU/L) were in agreement with the findings of Scott et al., (31), who found that that women undergoing IVF with a day 3 FSH < 15 m IU/ml were twice as likely to conceive as women with FSH between 15 and 24.9 m IU/ml. Also, Toner et al., (32) found that the predictive value of FSH for reproductive outcome in IVF as superior to female age alone. Another study found that when day 3 FSH level exceeded 20 IU/L conception rates fell precipitously (33). On the other hand, a single measurement of day 3 FSH may not be representative of actual ovarian reserve and confirmation of a very high result should be sought in a subsequent cycle (1). Also, clinical interpretation of such inter-cycle day 3 FSH fluctuations is controversial (34,35).There is a debate whether elevated FSH levels seen with reproductive aging may represent a primary neuroendocrine change rather than ovarian one (36). Finally, some clinicians, because of the possibility of confusing results in women with low risk for poor ovarian response, have questioned the value of widespread FSH screening (3). The predictive values of serum estradiol in this study (< 75 pg/ml) were in agreement with the findings of Licciardi et al., (11) who studied the correlation of reproductive outcome with systematic measurement of both serum E2 and FSH on cycle day 3. They observed that even when FSH values were <20 mIU/ml, no pregnancy occurred when day 3 serum E2 was > 75 pg/ml. This was supported by Buyalos et al.,(37) who found that day 3 serum E2 < 80 pg/ml with normal FSH was associated with better outcome in women who are undergoing fertility treatment. Smotrich et al., (12) and Evers et al., (10) also found that low day 3 E2 levels were associated with improved stimulation response and pregnancy rates, as well as lower cancellation rates (10,12). The predictive values of the antral follicle count (> 6) were in concordance with the findings of other studies. Bansci et al.,(38) studied the predictors of poor ovarian response in IVF and found that AFC provides better prognostic information on the occurrence of poor response during hormonal stimulation for IVF than does chronological age and the currently used endocrine markers. However, they concluded that endocrine tests remain informative. Also, Sylvestre et al., (39) studied the role of baseline ultrasound and serum hormonal levels in prediction of follicular response to gonadotropine stimulation during IVF. They found that antral follicle count is the best pre-treatment predictor of the follicular response to gonadotropine stimulation during IVF. Furthermore, Morris et al., (40) studied the role of TVS in determination of the number of primordial follicles as a measure of the ovarian reserve. They concluded that the number of antral follicles detected by TVS has been shown to be a predictor of fertility treatment outcome. The predictive values of the ovarian volume (> 3 cm3) were similar to the findings of Lass et al.,(20) and Syrop et al., (15,16). They found that measurement of the ovarian volume by transvaginal ultrasound before treatment with gonadotropins can predict the ovarian responsiveness in IVF. Also, the role of ovarian volume in evaluation of the ovarian reserve in assisted reproduction has been emphasized by Frattarelli et al., (41) who suggested a prospective novel method of determination of the ovarian size during IVF cycles. In contrary, Tomas et al., (42) and Dumesic et al., (30), fail to find a significant relationship between ovarian volume and ovarian response. The findings in this study are supported by the findings of several studies which investigated the incidence, clinical characteristics, biochemical (FSH, inhibin-B and estradiol), and biophysical markers (AFC and OV) and reproductive performance in the general infertility patients including those receiving different ovulation induction drugs and particularly those with poor or diminished ovarian reserve (4-6,10-17,24,31, 32,37-40,43). Scott et al., (44) found that approximately 10% of the patients in the general infertility population had an abnormal test and the incidence increases with age. Failure of ovulation with different ovulation induction drugs is known to occur in the general infertility patients particularly with those with poor or diminished ovarian reserve i.e. "poor responders". (43,45, 46). Using Univariate analysis, in this study, ovulation was significantly correlated to the levels of FSH, inhibin-B, estradiol, AFC and ovarian volume in the study group (n= 80). These findings are in accordance with the findings of other studies which evaluated the role of different screening parameters in prediction of the ovulation induction success with different end points of evaluation i.e. no of mature oocytes, ovulation rate, estradiol level, no of oocytes retrieved, fertilization rate, biochemical or ultrasound confirmed pregnancy rate...etc. For example, Chuang et al., (47) found that serum concentration of FSH in early follicular phase show an inverse relationship to the size of follicular cohort. Inhibin-B can serve as the earliest index of FSH dependent growth of the antral follicles (13). Also, the serum concentration of FSH during the cycle was found to be regulated by the negative feedback of ovarian hormones i.e. estradiol and inhibin-B (48,49). Muttukrishna et al.,(50) observed a negative correlation between FSH, inhibin-A and inhibin-B in women undergoing surgical menopause. They concluded that this relation may contribute to the observed early rise of FSH after surgical menopause. On Multivariate analysis of the variables that predict ovulation in induced cycles -in this study- it was demonstrated that of the biochemical variables FSH was the most significant contributor to ovulation, while of the biophysical variables AFC is the most significant one. These findings are in agreement with different studies which investigated the role of different markers in prediction of IVF success. Fawzy et al., (51) stated that day 3 basal FSH levels has proved the most useful, in that a poor IVF outcome was associated with higher levels of the hormone even within the normal range(52), and these results are in broad agreement with those reported by previous investigators (4,53,54). Yong et al.,(13) found that early follicular phase FSH supplemented by AFC remain of greater value in determination of the number of growing oocytes. AFC was found to provide better prognostic information on the occurrence of poor response during hormonal stimulation for IVF than does chronological age and the currently used endocrine markers (38). Nahum et al.,(11) found that antral follicle count was a better predictor of IVF outcome than were age or FSH. They concluded that AFC assessment may provide a marker for the ovarian age that is distinct from chronological age or hormonal markers. Child et al., (55) using multiple linear regression, found that the AFC was shown to be the most important independent predictor of the numbers of oocytes retrieved. AFC, OV and maximum ovarian stromal blood flow velocity can predict the number of oocytes retrieved in unstimulated cycles. However, there is a great debate among different studies about the best predictor of IVF success. Some studies suggested that age is a strong predictor of pregnancy rate (27,56-58), although other studies contradict this finding (59,60). Chuang et al., (47) found that both age and basal FSH levels contributed to the prediction of the quantitative ovarian reserve as reflected by the number of oocyte collected. However, they concluded that age is better predictor of pregnancy potential than FSH levels in women undergoing IVF. In conclusion, Day 3; serum FSH, inhibin-B, estradiol, AFC and ovarian volume are comparable screening markers of the ovarian reserve in the general infertility patients. Of the biochemical factors the main predictor for ovulation in induced cycles is FSH while AFC is the main biophysical one. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04008t8.jpg] [mf04008t6.jpg] [mf04008t5.jpg] [mf04008t7.jpg] [mf04008t2.jpg] [mf04008t4.jpg] [mf04008t3.jpg] [mf04008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}