 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 1, 2004, pp. 71-78 Laparoscopic ovarian re-electro cautery versus ovulation induction with FSH for persistant anovulation after laparoscopic PCOS treatment Momen A. Kamel, M.D., Alaa El-Din M. Abdel Hamid, M.D., Mahmoud Abdel-Rahim, M.Sc.,Sayed A. Mostafa, M.D. Department of Obstetrics and Gynaecology, Assiut University Hospital, Assiut, Egypt Reprint request: Dr. Momen A. Kamel, M.D. Dprt. of Ob. Gyn, Assiut University Hospital, 71111 Assiut, Egypt, Fax: 002088362204, E mail: momen_k2000@yahoo.com Received
on January 26, 2003; Code Number: mf04011 ABSTRACT Objectives: To determine the effectiveness and
safety of either another laparoscopic ovarian drilling or purified urinary FSH
for induction of ovulation in PCOS patients who were treated previously by
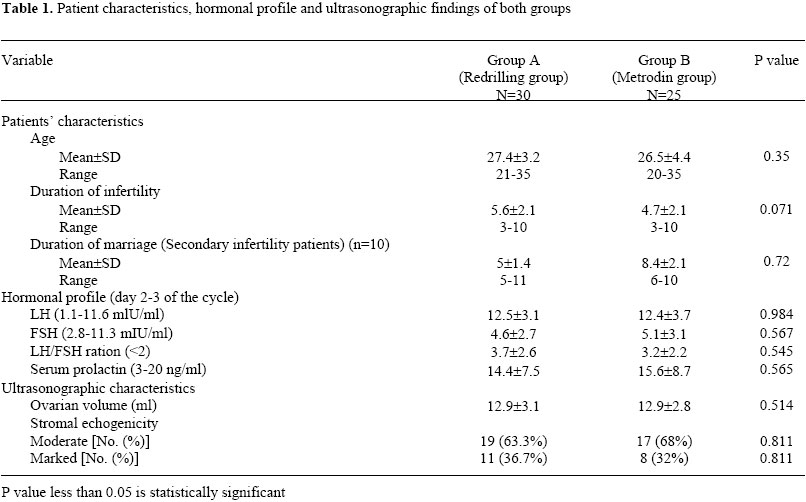
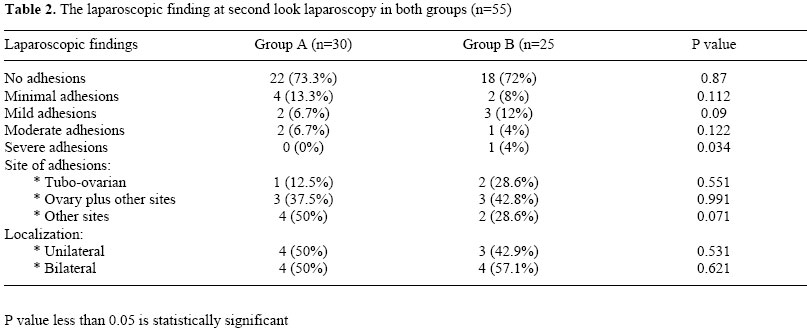
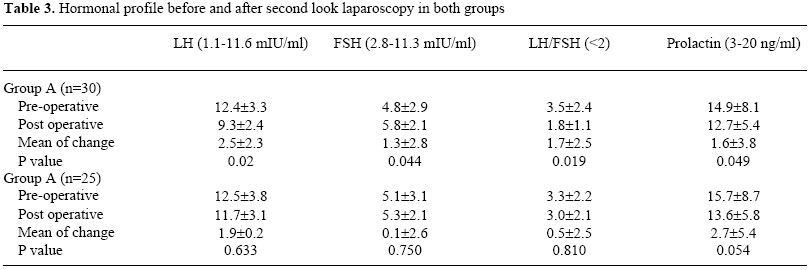
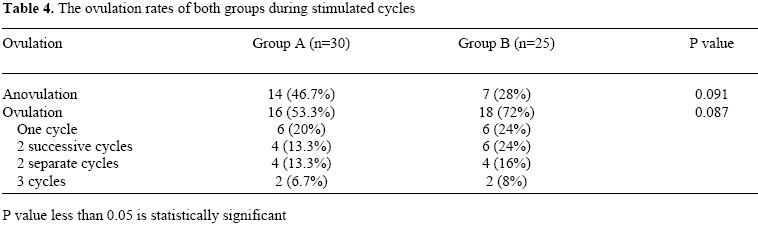
laparoscopic electrocautary but still anovulatory. Key words: polycystic ovary, infertility, induction of ovulation, second look laparoscopy, clomiphene citrate failure, laparoscopic re-electrocautary. Anovulatory infertility is a common problem in women with polycystic ovary syndrome (1,2). Polycystic ovarian syndrome accounts for 73% of cases of anovulatory infertility (3,4). Induction of ovulation by clomiphene citrate is the first line of treatment with ovulation rate reaching 80% (5). Although of this high rate of ovulation, pregnancy rate is low (1,6,7). Treatment with human menopausal gonadotrophins may be successful but it is extremely demanding for the women and for the clinician and there is a significant risk of hyperstimulation and multiple pregnancy even with intensive monitoring (1,8). Farquhar et al., 2002 in a randomized controlled trial of gonadotropin therapy for women with clomiphene citrate resistant polycystic ovary syndrome versus laparoscopic ovarian diathermy found no statistically significant difference in pregnancy or miscarriage rate during the 6-month follow up period or three cycles of gonadotrophin stimulation (9). Pulsatile leutinizing hormone releasing hormone (LHRH) therapy (with or without clomiphene) has been used but the results have been disappointing and the misscarriage rate is high (10). Wedge resection of the ovaries was used successfully in the management of the women with PCOS prior to the availability of antioestrogens in the 1960s; ovulatory cycles were diagnosed in approximately 80% of women treated. Disadvantages of wedge resection are that laparotomy is required and post-operative adhesions are high and occurring in up to 100% of treated women (11). More recently laparoscopic ovarian diathermy has been introduced as an alternative to wedge resection (12,13). The advantages of this form of treatment are that it entails laparoscopy rather than laparotomy and as the scars are small and there is no or minimal ovarian bleeding, it is probable that adhesion formation is less likely (14-16). Results from recent basic and clinical research investigations have greatly showed the importance of insulin resistance (IR) associated with PCOS in particular. Postulated relationships among PCOS, hyperandrogenism and insulin resistance do not completely solve the endocrinologic mystery of the patient with PCOS. For example, how does partial destruction of the ovary (e.g wedge resection or ovary drilling by laser or cautery), which does not affect insulin resistance, result in ovulatory cycles? (17). It also remains to be determined whether PCOS and type 2 diabetes mellitus represent no more than different clinical manifestations of the same IR syndrome, with their phenotypic differences due to the presence or abscence of a coincidental genetic defect at the level of the ovary or pancreas, respectively or representing the result of etiologically different subtypes of IR syndrome (18). Ovulation has been found to occur postoperatively in more than 80% of women treated with laparoscopic ovarian diathermy (12,13,16,19,20), yet 20% or more remain with anovulatory infertility. These patients were tried to be stimulated with clomiphene citrate or by HMG where it was shown that electrocautary improves ovarian response to gonadotrophins in clomiphene citrate resistant patients with polycystic ovary syndrome (21). Another laparoscopic re-electrocautary was tried by some gynecologists with no sufficient published data to support this maneover scientifically. We had done an extensive computer search to collect data about studies done to compare the results of any further treatment modalities for patients remained with anovulatory infertility after laparoscopic PCOS electrocautary, yet no single study was found in this aspect to give information about the effect of redrilling of the ovaries. Ovarian redrilling theoretically will inflect more adhesions. There is a risk of more ovarian tissue destruction and ovarian follicular depletion leading to premature menopause as well as the risk of surgery. The aim of the work is to determine the effectiveness and safety of either another laparoscopic ovarian drilling or ovulation induction by purified urinary FSH in the treatment of anovulatory PCOS patients after previous laparoscopic ovarian drilling. MATERIALS AND METHODS Fifty five patients were included in this study. All of them were previously treated by laparoscopic drilling for management of anovulatory infertility of PCOS. All patients were attending the Outpatient Infertility Clinic of the Department of Obstetrics and Gynecology, Assiut, Egypt from April 2000 to November 2001 and still anovulatory at least six months after the first laparoscopy. Inclusion criteria 1. Age less than 35 years. All patients were subjected to induction of ovulation by clomiphene citrate (starting from 50 mg twice daily from the third day of the cycle for 5 days for 2cycles and if anovalation persisted in the third cycle 250 mg every day for five days starting from third day of the cycle was given) with ovulation monitoring by serial transvaginal ultrasonic evaluation. If anovulation was persistent after these 3 induced cycles, patients were randomly allocated into two main groups before performing the second look laparoscopy. Randomization was done with a simple random table this explained why the two groups are unequal because the data of patients attending the second look laparoscopy with bilateral tubal patency were included in the study. In both groups second look laparoscopy was done to evaluate the condition of the ovaries, to assess the presence of adhesions, to localize their sites and to determine their degree according to the American Fertility Society Classification of adhesions (AFS) now (ASRM). Adhesolysis was performed if adhesion was present. In group A which included 30 patients another laparoscopic electrocautery was performed. The technique used was standerized to all patients as follows: Grasping the ovarian ligament by atraumatic forceps 5 mm introduced through the contralateral port of the ovary then moved to the front of the uterus or towards the anterior abdominal wall to prevent injury of other plevic organs. An insulated puncture needle introduced through the epsilateral port and six to ten puncture points were made through the ovarian capsule in the antimesenteric surface using electrocautery. The same procedure was applied to the other ovary. A monoplar electrocautery current at a 30-W power is used for 4 seconds. Each punctare is about 4 mm in diameter and 6-8 mm in depth. No coagnlation was done within 10 m m of the hilum to avoid bleeding or permanent reduction of the ovarian supply. In group B which included 25 patients no electrocautery was performed. Before second look laparoscopy, all the following data were collected. 1. Menstrual pattern (Rhythm, duration). 2. Hormonal profile (LH, FSH, LH:FSH ratio and prolactin) day 2-3 of the cycle before laparoscopy. 3. Base line transvaginal ultrasonography to: All patients were followed up for 6 months. The first 3 months were unstimulated (no induction of ovulation was done). The next 3 cycles were stimulated where patients in: Group A: were given clomiphene citrate (CC) 50mg twice daily for 5 days starting from the third day of the cycle. Group B: Purified urinary FSH (Metrodin®, Serono, Italy) was given as one ampoule (75 IU) 1.M daily from the third day of the cycle. In both groups follow up of ovulation by serial transvaginal ultrasonography was performed and when one or more of the follicles reached 17 mm or more, 2 ampoules of HCG (profassi® 5000 IU serono, Italy) were given 1.M with timed intercourse 36-48 hours latter. During the follow up period the following data were recorded: 1. Menstrual pattern. 2. Hormonal profile (LH, FSH, LH : FSH ratio and prolactin) at day 2-3 of the cycle following the second look laparoscopy. Progesterone level as one predictor of ovulation was estimated at day 21-22 of first cycle in ovulatory patients but in anovulatory patients it was estimated at day 21-22 of the last follow up cycle. 3. Ovulation monitoring. 4. Pregnancy. In the present study the age of the patients ranged from 20-35 years with a mean of 27.1±3.8 years. The number of patients with primary infertility was 45 patients and that with secondary infertility was 10 patients. In group A: The number of patients with primary infertility was 24 (80%) patients and that of secondary infertility was 6 patients (20%). In group B: The number of patients with secondary infertility was 4 patients (16%). There was no statistically significant difference between both groups, (Table 1). The protocol of the study was approved by the Ethical Review committee in both the Faculty of Medicine and in the University. The data were normally distributed and the Statistical analysis of the data was performed using X 2, Fisher's exact or student's t-test considering P value of < 0.05 as statistically significant value. Sample size calculation was done using Epi Info Version 6. RESULTS Base line hormonal profile There was elevated levels of mean LH and LH/FSH ratio of both groups although the difference was statistically insignificant. The mean levels of FSH and prolactin were normal in both groups (Table 1). Ultrasonographic characteristics All patients in both groups had increased ovarian volume (>9 cm3) and all patients had increased stromal echogenicity (Table 1). Laparoscopic findings at second look laparoscopy Over all, the number of patients who were free from adhesions was 40 patients (72.7%). There were adhesions in 15 patients (27.3 %). Minimal adhesions were present in 6 patients (40%), mild adhesions were present in 5 patients (33.3 %), moderate adhesions were present in 3 patients (20.0%) and severe adhesions were present in only one patient (6.7%). Tubo-ovarian adhesions were present in 3 patients (20%), adhesions between the ovary and other sites other than the tube were present in 6 patients (40%) and adhesions away from the ovaries and tubes were present in 6 patients (40%). There were unilateral adhesions in 7 patients (46.7%) and bilateral adhesions in 8 patients (53.3%). Comparison of laparoscopic findings at second look laparoscopy in both groups is shown in table 2. There was no statistically significant difference except in case of severe adhesions which was statistically significant but this could be due to small number. Hormonal profile after second look laparoscopy Comparison of hormonal profile before and after second look laparoscopy in the included patients showed significant statistical difference in group A while in group B the difference was statistically insignificant (Table 3). Serum prolactin decreased due to medical treatment and not due to the procedure. Ovulation In the 55 studied patients, ovulation in the first 3 unstimulated cycles occurred in 17cycles out of the 165 observed cycle (10.3%). It occurred in 11 cycles in group A (redrilling group) and in 6 cycles in group B (Metrodin group), but all these occurred in one cycle only. No repeated ovulation was recorded in any patient. This represents 12.2 % and 8% ovulation rate per cycle in group A and B, respectively. During the 3 stimulated cycles where clomiphene citrate was given to group A and metrodin was given to group B ovulation occurred in 34 patients (61.8 %). It occurred in 16 patients of group A (53.3%) and in 18 patients of group B (72 %). Out of the 34 ovulated patients, the number of cases who showed ovulation in all the stimulated cycles was 4 patients (11.8%), the number of cases who showed ovulation in 2 successive cycles was 10 patients (29.4 %), the number of cases who showed ovulation in 2 separate cycles (1st and 3rd cycles) was 8 patients (23.5%) and the number of cases who showed ovulation in one cycle was 12 patients (35.3%). (Table 4) shows the distribution of ovulatory cycles in both groups. Although the ovulation rate was higher in group B (72%) in comparison to group A (53.3%); the difference was statistically insignificant. Pregnancy rate Six cases got pregnant during the period of follow up; 2 cases from group A and 4 cases from group B. In group A, the 2 pregnancies occurred in the second stimulated cycle. In group B, one pregnancy occurred in the first stimulated cycle, 2 pregnancies occurred in the second stimulated cycle and one case occurred in the third stimulated cycle. There is no single case of pregnancy occurred during unstimulated cycles. The pregnancy rate per cycle was 3.8% in all included patients. The pregnancy rate per patient was 10.9%. In group A (redrilling group) the pregnancy rate per cycle was 2.2% and pregnancy rate per patient was 6.6%. In group B (metrodin group), the pregnancy rate per cycle was 5.7% and pregnancy rate per patient was 16%. There was no statistically significant difference between the pregnancy rate per patient of both groups (P value 0.083). The pregnancy rate per cycle showed statistically significant difference (P value 0.042). DISCUSSION Laparoscopic management of PCOS anovulatory infertility became a common practice for the treatment of clomiphene citrate resistant cases because of high percentage of ovulation and conception occurring following its performance. Also postoperative adhesions are low compared to bilateral wedge resection by laparotomy (25). After laparoscopic ovarian electrocautary there is a significant reduction in the serum LH (13,26,21). The ovarian response to gonadotrophins showed a marked improvement. There is a significant increase in the number of ovulatory cycles, together with a significant reduction in the number of ampoules of gonadotropins used for stimulation, with improved pregnancy rate (21,27) Laparoscopic management is not out of disadvantages. One of them is its temporary effect. It may inflict adhesions, it also causes ovarian tissue destruction and ovarian follicular depletion which may lead to premature menopause (28). Also, some patients failed to respond and because of increased use of laparoscopic treatment we expect to have an increasing number of patients who are still infertile after laparoscopic procedures to treat PCOS infertility. The management of these patients "infertile PCOS patients after laparoscopic treatment" now is a real dilemma, and a clear protocol to manage these patients is not discussed at least to our knowledge before. In the present study we tried two different treatment modalities namely another laparoscopic drilling or induction of ovulation by purified urinary FSH. In the present study the incidence of adhesions at second look laparoscopy was 27.3% which is in agreement with the results of previous studies "Armar et al., 1990 who reported adhesions in 24% of cases (19)", Naether et al., 1994 reported 33% postoperative adhesions (28), and Zakhera (1999) reported post operative adhesions in 22.7% of patients (16). According to American Fertility Society (AFS) classification of adhesions (ASRM now) 74% of the adhesions were minimal and mild and only 20% were tuboovarian adhesions. After second look laparoscopy, regular cycles were recorded in 27 patients (49.1%) during the first 3 unstimulated cycles increased to 43 patients (78.2%) during the next 3 stimulated cycles compared to 17 patients (30.9%) before second look laparscopy without significant statistical difference between both groups, this reflects the marked improvement in the underlying hormonal profile. The study of hormonal changes following the second look laparoscopy revealed significant reduction in post operative mean levels of LH, LH: FSH in group A. These figures are in agreement with previous studies (13,26,21), but in group B there were slight insignificant changes in the hormonal levels which is expected as there was no ovarian intervention. Ovulation (documented by ovulation monitoring by US and progesterone level at day 21-22 of the cycle) occurred in 61.8% of patients during stimulated cycles. It occurred in 53% of patients stimulated with clomiphene citrate in group A (who were treated by redrilling) and 72% of group B patients (who were treated by metrodin). The difference was statistically insignificant. These results are lower than that of laparoscopic surgery performed for the first time for treatment of resistant cases of PCOS anovulation after maximum doses of clomiphene citrate. Ovulation in the stimulated cycles did not occur in all the follow up cycles of the ovulatory women except in 11.8%. It may occur in one cycle or in 2 successive or separate cycles. About 35.3% of the ovulation occurred only in one cycle (12 of 34 patients). Ovulation in the all follow up cycles occurred in only 11.8 % of ovulatory patients (4 out of 34 patients ) and it occurred in one patient of group A (i.e. following redrilling) and 3 patients of group B (i.e following induction of ovulation by metrodin). Although our end point was ovulation detection, the pregnancy rate was calculated. Six out of the 55 included patients in the study conceived during the follow up period (3.8 % per stimulated cycle and no patient got pregnant in unstimulated cycles). This low pregnancy rate may be attributed to the nature of patients included in this study who are resistant infertile anovulatory patients after the laparoscopy and multiple courses of ovulation induction. It can be also to some extent attributed to the short follow up period and longer follow up may add a new number of pregnancies. But this can not be accepted as the only cause of this low pregnancy rate. Zakhera (1999) reported that mean operation pregnancy interval was 2.4®1.3 months and about 80% of pregnancies occurred within the first 3 months postoperatively (16). Amin (1994) reported that 70% of pregnancies occurred within the first 3 post-operative cycles (29). These two studies were performed in the same unit of our study. Periadnexal adhesions may take a part in the explanation of this phenomenon preventing the pick up of the ovum by the fimbria of the tube. In previous studies hyperprolactinamia may play a role but cases of hyperprolactinuemia were treated before 2nd look laparoscopy. Using an insulated needle cautary for laparoscopic ovarian drilling for clomiphene resistant anovulatory women with PCOS is associated with minimal amount of adhesion formation as mentioned by Felemban et al., 2000 (30). All these factors may act with each other to cause infertility in ovulated patients or there may be hidden cause for infertility (male factor and tubal obstruction were excluded from the study). During the final revision of the paper one article described the effect of repeated ovarian diathermy in PCOS patients. This retrospective study was performed on twenty anovulatory infertile women with PCOS. An overall ovulation rate of 60% and pregnancy rate of 53% were achieved (31). CONCLUSION The different treatment modalities and the merits and disadvantages of each option for management of infertile anovulatory PCOS patients after first laparoscopy should be explained to the patients during counseling. Another laparoscopic electrocautery after failure of the first trial is a treatment option of lower pregnancy rate than FSH stimulation with possible hazards so it is better to be avoided. Induction of ovulation with purified FSH for PCOS anovulation should be encouraged because of its high ovulation rate, yet its cost benefit status should be explained to the patients. Possible hazards and low pregnancy rate of ovarian re-drilling than FSH stimulation should be taken in consideration if similar studies with larger numbers of patients will be tried, which is not recommended by the authors REFERENCES
The following images related to this document are available:Photo images[mf04011t1.jpg] [mf04011t2.jpg] [mf04011t4.jpg] [mf04011t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}