 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 1, 2004, pp. 79-83 Three Dimentional Transvaginal ultrasound in the assessment of uterine lesions: when do we really need it? Alaa N. Ebrashy, M.D., Mohamed Momtaz, M.D., Osama A. Shawky, M.D., Ehab M. Soliman, M.D., Zakareya Aboul Maaty, M.D. Department of Obstetrics and gynecology, Kasr El Aini Hospital, Cairo University, Cairo, Egypt Correspondence: Alaa Ebrashy, No 2 - Cross 7/154 St Maadi, Tel: 5254477, Fax: +2025260168, E-mail: ebrashy@bigfoot.com Received
on June 26, 2003; Code Number: mf04012 ABSTRACT Objective: To evaluate the use of Transvaginal 3D
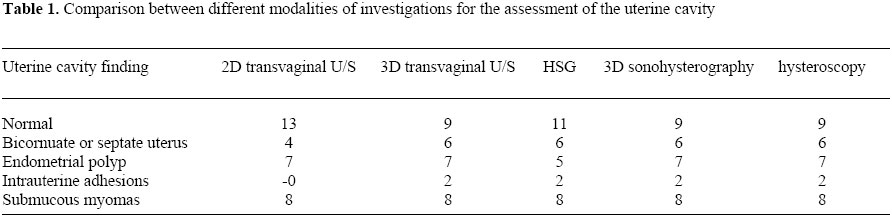
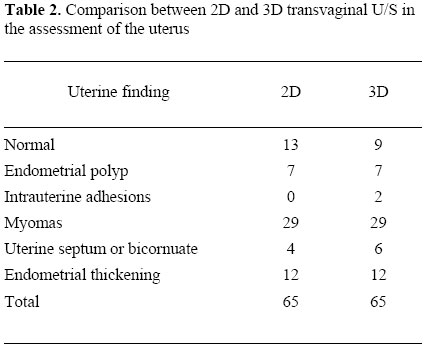
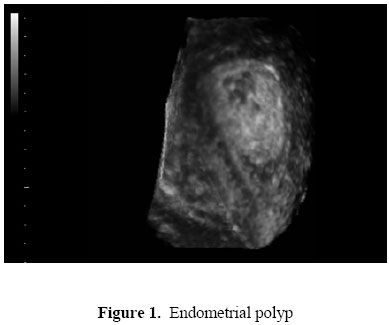
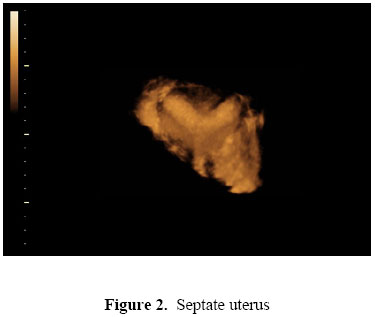
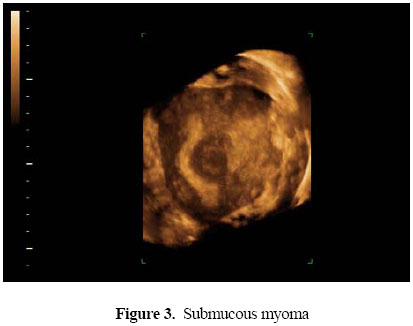
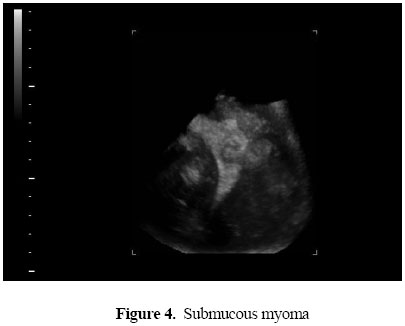
U/S in the assessment of uterine pathology and uterine cavity abnormalities. Key words: 3D transvaginal U/S -Uterine cavity - Hysteroscopy-uterine cavity anomalies The objective of an U/S examination is to get a spatial impression of the examined organ. With the conventional technique, the examiner has to imagine a 3D idea of the shape, size, and position of the organ being examined. By Transvaginal 2D U/S, the examination of the uterine lesions is limited to the transverse and sagital planes, which sometimes give an inadequate view of the uterus and its corresponding pathology (1). 3D U/S is a multiplaner simultaneous 3 axes sectional image displayed on the same screen. These 3 planes (frontal, sagittal, and coronal) can be displayed anatomically and topographically layer by layer. -3D allows volume examination on the monitor simultaneously in three perpendicular planes. All three planes are located in a separate window and each of them can be rotated at 90 degrees to each other in all three axes. After acquiring the required volume, the presence of the patient is no longer needed, so the examination last no more than 3 minutes. It has the ability to register all three imaging planes simultaneously as well as to visualize surfaces 3 Dimensionally (2). 3D U/S enables visualization of the uterus in the coronal plane which is rarely seen on conventional B-mode scans. Transvaginal 3D U/S thus provides a unique diagnostic tool for non invasive studies of the uterine morphology and diagnosis of congenital uterine anomalies (3). Sonohysterography is proposed for evaluation of endometrial abnormalities. It is indicated when endometrial lesions eg, submucous fibroid -endometrial or endocervical polyps -uterine septum are suspected -It involves the injection of U/S -ve contrast media (saline) or + ve (Echovist) into the uterine cavity during transvaginal scanning (4). MATERIALS AND METHODS The study was conducted in Kasr El Aini hospital. Cases were recruited from the outpatient gynecological clinic. 65 cases were included in the study in the period between Jan 2002 and Jan 2003. . They were recruited based on their complaint which were either vaginal bleeding, reproductive failure (recurrent abortion or infertility). Age range between 21-47. All cases were subjected following investigations by both 2D Transvaginal U/S, and 3D Transvaginal U/S. The following procedures were done for All the cases which showed uterine pathology:-Hysterosalpingraphy, hysterosonography, (injection of saline in the uterine cavity with simultaneous U/S examination ) and hysteroscopy. hysterosonography (injection of saline in the uterine cavity with simultaneous U/S examination ) was also done only in cases showing intrauterine pathology. All these procedures were done 2 to 3 days postmenstrual and in an episode of no vaginal bleeding. Laparoscopy was done in selected cases demonstrating uterine cavity anomalies. In these cases hysteroscopy and laparoscopy were considered the gold standard for diagnosis. For HSG we used aqueous contrast medium (Urograffin: Shering Germany). We used laparoscopy and rigid hysteroscopy (Karl storz Germany). We used 3D U/S machine (Medison Voluson 530D-MT Medison Co. Ltd) in which we did both 2D and 3D U/S. Sonohysterography procedure was done by introducing sterile vaginal speculum to visualize the cervix. the cervix was cleaned by povidone -iodine 10%. then a plastic Nelaton catheter number 8 Fr (Eastern Medikit limited) or an intrauterine insemination catheter (Gynetices medical products Belgium) was inserted through the cervix to inject around 10-20 cc of saline in the uterine cavity, the speculum is then with drawn and the endovaginal probe was reinserted posterior to the catheter to the posterior fornix of the vagina. Sterile saline was injected slowly through the catheter, usually 10-20 ml of fluid were needed. The patients tolerated the procedure with minimal discomfort. For evaluating the uterine anomalies we used the American Fertility Society classification 1988 (5). RESULTS We examined 65 cases by both transvaginal 2D and 3D U/S. 9 cases had normal uterine cavity and no uterine pathology. 29 cases had myomas either single or multiple, from which 8 cases had submucus myomas. Seven cases had endometrial polyps. 12 cases had thickened endometrium. 6 cases had uterine cavity anomalies. Two cases had intrauterine adhesions. Using hysteroscopy as the gold standard in diagnosing uterine cavity lesions, there was 2 cases with Mullerian anomalies both were septate uterus and 2 cases with intrauterine adhesions were diagnosed by Transvaginal 3D U/S, while being missed by 2D U/S (4 false negative cases -sensitivity = 93% compared with 100% for 3D U/S). There were 2 cases of endometrial polyps which were missed by HSG and diagnosed by 3D transvaginal U/S (-2 false negative cases -sensitivity 92% compared with 100% for Transvaginal 3D U/S. In all cases with Mullerian anomalies: 3D TVS correlated well with HSG and hysteroscopy however with an additional information concerning the visualization of the surrounding myometrium and the accurate differentiation between septate and Bicornuate uterus. Sensitivity of Transvaginal 2D U/S for uterine assessment was 93% and for transvaginal 3D U/S was 100%. 2D Saline sonohystrography was very helpful in diagnosing polypi, uterine cavity anomalies. However 3D saline Hysterosonogarphy offers advantages over that with 2D saline Hysterosonography in that the uterus is distended for a shorter time than that necessary for 2D examinations. It seems that the picture depicted by 3D Transvaginal U/S for the uterine cavity was beyond any doubt for diagnosing any abnormality to the extent no further enhancement by contrast media is needed except in cases with intrauterine adhesions which in this cases it might prove to be helpful ( Table 1, Table 2 & Figure 1, Figure 2, Figure 3, Figure 4). DISCUSSION Obstetrics and gynecology is likely to undergo revolutionary changes in diagnostic image with the arrival of 3-D US. Recent reports have focused on the diagnostic capabilities with this method to assess the uterine cavity abnormalities (6). The acceptance of Transvaginal 2D sonography as a screening tool for the presence of uterine pathology is beyond any doubt, however recently with the introduction of 3D U/S, this is obviously being challenged specially concerning the uterine cavity anomalies and the uterine cavity lesions (7). Being easy, non invasive office procedure it definitely surpass the HSG in evaluating the uterine cavity being a rather minimal invasive test requiring the use of iodinated contrast agents and exposure to minimal irradiation. Further more it visualize the frontal plane of the uterus which is not seen by HSG (8). Jurkovic et al pointed out that lateral fusion disorders of the uterus often require laparoscopy or laparotomy to make a definitive diagnosis (9). We agree with him that 3D U/S was able to easily differentiate septate and bicornuate uterus without the help of the laparoscopy as it visualize both the uterine cavity and the surrounding myometrium. Giving the chance to assess the fundus from outside and the cavity from inside simultaneously. Concerning the lesions within the substance of the uterus not involving the cavity it was revealed that 3D U/S did not offer better opportunity than 2D U/S concerning diagnosis except in more diagnostic perception of the size and site of the lesion. This concept was also supported by others (10). The same is applied for the endometrial thickness and the diagnosis of Hyperplasia however the volume of the endometrium measured by 3D may offer a better chance in proper evaluation of the management. We as well as other authors believe that it would be of great attribution in cases of postmenopausal bleeding evaluation (11). In cases of submucous myomas, in spite of the act that the diagnostic accuracy of both 2D and 3D U/S is almost the same, However the spatial and the reconstructed image produced by the 3D frontal view of the uterus is more informative specially when it comes for the decision of management either, myomectomy through open surgery, or hysteroscopic myomectomy (12). Considering sonohysterography Weinraub et al were among the first to evaluate the findings of different pathology of the uterine cavity abnormalities with 3D saline sonohysterography (13). They addressed that the simultaneous display of the zone of interest in three perpendicular planes enhances imaging capabilities, while surface rendering provides a comprehensive overview of the surface area of the findings and their topographical orientation Ayida et al 1996 emphasized that 3D scanning to assess the uterine cavity appeared to offer no advantages over conventional 2D contrast sonography (14). We had our experience with 2D Saline sonohystrography and we found that it was very helpful in diagnosing polypi, sub mucus myomas and uterine cavity anomalies (4). In this study we see that the 3D illustration of the uterine cavity was so impressive and precise that it alleviated the need for 3D contrast scanning and in turn the 2D contrast scanning, However it may be give more accurate information in cases with intrauterine adhesions concerning the location and the extent of adhesions which is a pivotal point for the preoperative assessment and the plane for management. Furthermore, the uterus is distended for a shorter time than that necessary for 2D contrast examinations. CONCLUSION 3D TVS is an exciting new technology that provides valuable information in investigating the uterine cavity abnormalities. 3D TVS allows surface and volume rendering that can produce photographic like images It is believed that, in the near future, 3D U/S equipment will be less expensive, which will allow its wide spread application. We recommend asking for 3D TVS in these cases: 1-In Mullerian anomalies involving the uterine cavity:septate and bicornuate uterus it has several advantages over HSG,2D and Hysteroscopy which is its ability to visualize the uterus in coronal plane visualizing both the endometrial cavity and the surrounding myometrium. we believe that the advantage of this technique along with capacity to create 3D spatial reconstructions of pelvic organs is certain to make it the procedure of choice for these cases 2- Submucous myoma and Endometrial polyps and intrauterine adhesions. 3D U/S alone or combined with 3D sonohysterography is valuable in delineating their location and position in relation to the cavity which is the essential in planning to manage them by surgery remove these either by surgery or endipivotal assists in surgical planning, REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04012t1.jpg] [mf04012f3.jpg] [mf04012f2.jpg] [mf04012f1.jpg] [mf04012t2.jpg] [mf04012f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}