 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 2, 2004, pp. 93-100 REVIEW Chlamydia testing in infertility management Jolande A. Land, MD Department of Obstetrics and Gynaecology, Research Institute Growth and Development (GROW), Academisch Ziekenhuis Maastricht, and MaastrichtUniversity, Maastricht, The Netherlands Correspondence: Jolande A. Land, Department of Obstetrics and Gynaecology, Academisch Ziekenhuis Maastricht, P.O. Box 5800, 6202 AZ Maastricht, The Netherlands, Tel: +31 43 387 6776, Fax: +31 387 4765, Email: jlan@sgyn.azm.nl Received on December 15, 2003; Code Number: mf04017 ABSTRACT In the majority of women, chlamydia infections occur during adolescence, and remain asymptomatic. These unrecognized and untreated infections may increase the risk for tubal factor subfertility at a later age. Since the association between chlamydia IgG antibodies in serum and tubal
pathology was noticed, chlamydia antibody testing (CAT) has been used in the
fertility work-up as an inexpensive and non-invasive screening test for tubal
factor subfertility. The predictive value of CAT is limited, however, and clinicians
should be aware of factors known to affect the diagnostic accuracy of CAT (such
as test and cut-off titre used, and definition of tubal factor subfertility).
Key words: Chlamydia trachomatis, Chlamydia antibody testing, tubal pathology, infertility, cervical screening, uterine instrumentation CHLAMYDIA The genus Chlamydiaceae consists of nine species, of which only C. trachomatis, C. pneumoniae and C. psittaci are human pathogens. C. trachomatis has been subdivided into two biovars: trachoma (causing ocular disease, genital infections and infant pneumonia) and lymphogranuloma venereum (LGV). The trachoma biovar is further subdivided into 15 serotypes, on the basis of antigenic differences in their cell walls. The antigenicity of the chlamydia cell wall is determined by the outer membrane, which consists of a lipopolysaccharide (LPS) and proteins, including the major outer membrane protein (MOMP). LPS is a common component of the outer membrane of all Chlamydiaceae. MOMP has epitopes which are not only species-specific, but can be used to identify different serotypes as well.
Today, C. trachomatis is the most common sexually transmitted disease (STD) in industrialized countries. The highest prevalence is found among adolescents, with two or more sexual partners in the past year (1). Lower genital tract sampling has revealed the presence of chlamydia in 12% of women attending STD clinics (2), but also in 5% of asymptomatic women (1,3). The major problem in the control of genital tract chlamydia infections is that as many as 70-80% of women and up to 50% of men who are infected do not experience symptoms (4,5). This results in a large reservoir of undiagnosed, infected individuals who can transmit the infection to sexual partners, in whom upper genital tract infections and late complications may develop. Evidence exists, however, that in about half of asymptomatic women with lower genital tract infections the micro-organism will be cleared spontaneously (6). In the remaining group, cervical infections maypersist over many years (7), and in about 10%cervical infections will ascend to the upper genitaltract and induce pelvic inflammatory disease (PID) (8,9).
C. trachomatis is an immunogen which stimulates both the humoral and cell-mediated arms of the immune system, leading to antibody formation and T cell activation (10). After primary chlamydia infection, immunity is considered to be only partially protective, however. Since the micro-organism is sequestered within intracellular sites it may remain unrecognized by the immune system. This may predispose to persistence of the micro-organism in the genital tract, and to recurrent infections (11). Recurrent infections may be caused by reinfections as well, with other chlamydia serovars, or with the same serovar after antigenic mutations in MOMP (7, 12). Clinical studies show that recurrent chlamydia infections are common, the recurrence rate being 30-50% in young adolescents (13). One current hypothesis is that only hosts repeatedly exposed to the micro-organism (either by persistent infection or reinfection) develop extensive tissue damage in the upper genital tract (14,15). This tissue injury appears to be induced by cell-mediated immunologic reactions, including a delayed hypersensitivity response (10,14), which leads to fibrosis and scarring, and ultimately to tubal factor subfertility. Tubal factor subfertility
Tubal pathology is the main cause of subfertility in 10-30% of couples in developed
countries (16,17,18), and in up to 85% in developing countries (19). The
main cause of tubal pathology is PID, which, in the majority of cases, is
due to C. trachomatis, Neisseria gonorrhoeae, or both. Studies on the prevalence of C. trachomatis in patients with proven PID have shown that more than half of PID cases are caused by C. trachomatis (10). In the last decades the incidence of gonococcal infections has declined in western countries (20), whereas the number of infections due to chlamydia is still rising. Only in countries in which screening programs have been introduced to prevent chlamydia infections, a gradual decline in the rate of chlamydia infections has been noted (3).
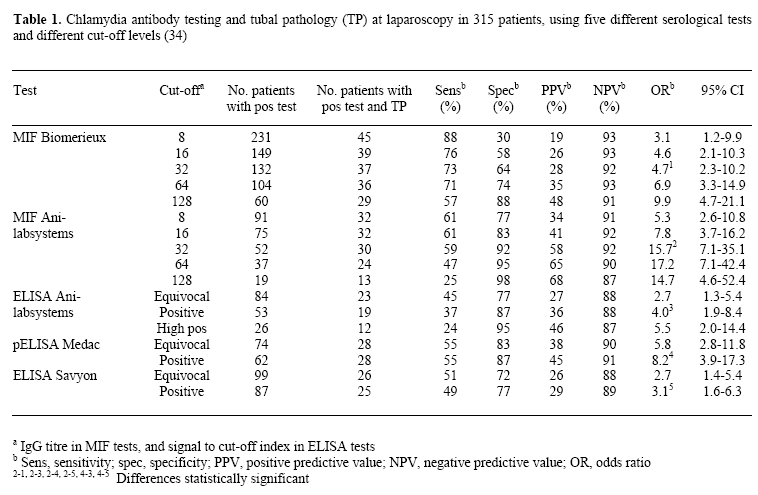
Weström's classical studies (21) indicated that the incidence of tubal factor subfertility is approximately 10% after one episode of PID, about 20% after two episodes, and over 40% after three episodes. All PIDs were laparoscopically confirmed, but only symptomatic patients had been included in the studies. Most women who have tubal factor subfertility, however, have never been diagnosed with PID, since their infections have been asymptomatic or subclinical. Seroepidemiological studies have indicated that chlamydia infections account for a large proportion of these asymptomatic infections, by demonstrating a strong link between the presence of serum antibodies to C. trachomatis and the presence of tubal pathology (22). Since C. trachomatis invades columnar epithelium in particular, the densely ciliated ampullary segment of the fallopian tube is most susceptible to chlamydia infection. In this way chlamydia PID can cause distal tubal occlusion and subsequent infertility, or partial distal occlusion with an increased risk for ectopic pregnancy. Tubal pathology can be diagnosed by hysterosalpingography (HSG) or laparoscopy, i.e. by invasive and expensive means only. Laparoscopy is considered the best available test for diagnosing tubal factor subfertility, and is the accepted reference test in the evaluation of diagnostic performances of other tests. But, as general anaesthesia is required, laparoscopy is unsuitable for screening purposes on a large scale. Today, HSG is the most widely used screening test for tubal factor subfertility. As compared to laparoscopy, specificity of HSG is 83%, and sensitivity is 65% in diagnosing tubal patency (23). For diagnosing adhesions, sensitivity of HSG is only 46% (23). Furthermore, clinical pelvic infection following HSG has been reported in up to 4% of cases, and in 10% of women with tubal disease (24). The poor predictive value for tubal pathology and the high prevalence of febrile morbidity question HSG as the best screening test in high risk patients for tubal factor subfertility. Chlamydia antibody testing (CAT) in serum As screening by HSG appeared to have low sensitivity, and laparoscopy to be unsuitable for screening on a large scale, clinicians have searched for other tests to estimate the risk of tubal pathology in subfertile women. The aim was to find an inexpensive and non-invasive test which could accurately discern high risk and low risk patients for tubal factor subfertility. Ideally, based on the results of this screening test one would subject high risk patients to diagnostic testing (i.e. laparoscopy), and delay additional invasive and expensive testing in low risk patients. Since it was noted that the majority of tubal pathology cases are due to chlamydia infections, and the development of late sequelae is associated with chlamydia IgG antibody formation (22), chlamydia antibody testing (CAT) in serum has been introduced as a screening method for tubal factor subfertility. A widely used test for CAT is the (micro) immunofluorescence test (MIF), which has been considered the gold standard in the serological diagnosis of chlamydia infection (25). Initially, antigens from elementary bodies of each of the serotypes of C. trachomatis were included in the MIF test, which provided serotype-specific antibody testing (26). Later, for practical reasons, the number of antigens has been reduced by pooling antigens of epidemiologically related serotypes, or by using one broadly reacting serotype (usually L2) (27). However, in modified MIF tests, cross-reactivity between C. trachomatis and C. pneumoniae occurs (28). To overcome this, species-specific MIF tests have been developed, in which LPS has been subtracted, a common component of the outer membrane of all Chlamydiaceae. Disadvantages of the MIF tests are that they are labour intensive, their reading is observer dependent, and interlaboratory variation is significant (29). To overcome these drawbacks, enzyme-linked immunosorbent assay (ELISA) tests with high specificity have been developed, using LPS-stripped elementary bodies as antigens (30). Recently assays have become commercially available in which specific synthetic peptides are used, based on MOMP of C. trachomatis, which contains species-specific and serotype specific epitopes (31). These ELISA tests are easy to perform and are well standardized (32). Although CAT has been incorporated in the fertility work-up on a large scale, no uniformity exists in assays and antigens used, and there is no agreement about cut-off titres for positive tests and definitions of tubal pathology. A critical reappraisal of the results reported in literature on screening for tubal factor subfertility by CAT, reveals heterogeneous results, and indicates that the predictive value of CAT for tubal pathology is limited: sensitivity of CAT varies between 30-88% and specificity between 45-100% (33). In order to shed more light on these inconsistent and generally poor results, various tests and methodological aspects of CAT have been investigated. The diagnostic accuracy of five commercially available CAT tests has been evaluated (34), using laparoscopy as a reference. The tests included in this study were a 'classic' MIF (Biomerieux, The Netherlands), a species-specific MIF (Anilabsystems, Finland) and three ELISA tests (Anilabsystems, Finland; Medac, Germany; Savyon, Israel). Since all tests were done in the same cohort of patients at the same time, the differences found are due to differences in antigenic composition of the tests. Although ELISA tests have been claimed to be highly sensitive and specific, they were not found to be superior in predicting tubal factor subfertility. Of the five tests evaluated, MIF by Anilabsystems had the best diagnostic performance (OR 15.7), and among the three ELISA tests, pELISA by Medac (OR 8.2) performed best (Table 1). Significant cross-reactivity with C. pneumoniae antibodies was found in all tests evaluated, except in pELISA by Medac. Economic analysis, taking into account diagnostic accuracy, cost of performing the test, and cost of consequences of false positive and false negative results, will show which test is to be preferred from a cost-effectiveness point of view. The impact of the definition of tubal factor subfertility on the diagnostic accuracy of CAT has been investigated (35). It has been shown that CAT is most accurate in predicting distal tubal pathology, instead of unspecified tuboperitoneal abnormalities or proximal tubal occlusion. Since the ampullary segment of the fallopian tube is most susceptible to chlamydia infection, the presence of chlamydia antibodies is associated with distal tubal disease. And, consequently, the predictive value of CAT will be poor for chlamydia-unrelated pathology, as proximal occlusion.
In studying the implications of different cut-off titres for a positive test
using MIF, it has been noted that increasing the cut-off titre will improve
specificity, at the expense of sensitivity. According to ROC curves, in which
the best combination of sensitivity and specificity is depicted, Land and
co-workers (35) found the most suitable statistical cut-off titre of CAT
to be 16. But in establishing a clinically relevant cut-off level for a positive
test, the aim of screening should be taken into consideration as well. For
instance, if there is limited access to laparoscopy, the number of patients
without tubal pathology subjected to laparoscopy has to be minimized. If
CAT is applied to select patients for laparoscopy, the number of false positive
tests should be low. Therefore, a high cut-off level for CAT (e.g. 64) may
be chosen because of its high specificity. However, in older patients, the
primary aim of screening may be prevention of delay in diagnosing tubal pathology,
and subsequent referral for IVF. In this situation, false negative results
have to be minimized. A low cut-off level for CAT (e.g. 16) may be chosen
because of its high sensitivity. Thus, the cut-off titre for a positive test
will influence the predictive value of CAT, but it has to be determined depending
on the aim of screening and the inception cohort.
Low sensitivity of CAT may be caused by false negative CAT results, i.e. negative CAT in patients with tubal pathology at laparoscopy. Some of these patients will have a chlamydia-unrelated cause for adhesions or tubal occlusion (e.g. endometriosis, cornual polyps or PID due to other micro-organisms). In others, however, no chlamydia antibodies may be found despite previous C. trachomatis infection. It has been hypothesized that false negative CAT results may be due to disappearance of IgG antibodies over time. Although it is assumed that chlamydia infections give rise to persistent IgG antibody formation, the exact course of titres over time is still poorly understood. Since most women have chlamydia infections during adolescence and present at fertility clinics 10-15 years later, IgG antibodies might become undetectable within this period. Several studies have reported on the course of IgG antibodies after antibiotic treatment of chlamydia infections (36,37,38,39). In 1-6 years a significant titre decline was noted in one third of women, but seroconversion from positive to negative was a rare event. Only one study has been done in asymptomatic, untreated, subfertile women (40). In patients with initial CAT titres >32, in 18% a decline of IgG antibody titres of two or more titre steps was found in 4-7 years, but in no patient IgG titres became undetectable by MIF (40). Therefore, it can be assumed that chlamydia IgG antibodies persist for a long time, even after antibiotic treatment, and decline in IgG antibody titre is not a significant cause of false negative CAT results. In discussing false positive CAT results, i.e. positive CAT in patients without tubal pathology at laparoscopy, unintended cross-reactivity between antibodies in CAT tests is a major issue. Cross-reactivity between C. trachomatis and C. pneumoniae antibodies may occur due to the many antigenic structures they have in common. The prevalence of C. pneumoniae antibodies in women in Western European countries is up to 70% (41). Reports in the literature concerning cross-reactivity between C. pneumoniae and C. trachomatis antibodies in CAT tests, are scarce and controversial. Two studies (42,43) concluded that no cross-reactivity occurs, since they found the same prevalence of C. pneumoniae antibodies in a group with a high prevalence of C. trachomatis antibodies, as compared to control groups with a low prevalence of C. trachomatis antibodies. Others (44) found that antibodies to C. pneumoniae may account for up to half of all chlamydia positive test results by MIF. In a study by Gijsen and co-workers (28) C. pneumoniae antibodies were found significantly more often in subfertile women without tubal pathology and a positive MIF test (in 84%), as compared to patients without tubal pathology and a negative MIF test (in 69%). The studies available indicate that antibodies against C. pneumoniae are common among women, and that cross-reactivity between C. trachomatis and C. pneumoniae antibodies cannot be excluded as a cause for decrease in specificity of the MIF test. To eliminate cross-reactivity, ELISA tests for C. trachomatis have been developed, based on synthetic peptides that are claimed not to share any sequence homology with C. pneumoniae MOMP (31). There is still very little data on cross-reactivity in these peptide-based ELISA tests, but, as discussed before, in most tests evaluated cross-reactivity could not be excluded (34). In conclusion, there is still no excellent screening test for tubal pathology in subfertile women. In order to develop more accurate tests for the prediction of chlamydia-associated tubal pathology, future research should focus on the immunopathology of chlamydia infections. Evidence exists that patients with chronic, persisting chlamydia infections are particularly at risk for developing late sequelae. Although IgG antibodies are markers of a previous infection, they do not reflect an ongoing chronic inflammation properly. Candidates to be introduced into screening for tubal factor subfertility, in addition to specific C. trachomatis IgG antibodies, are anti-heat shock protein 60 (HSP60) and anti-LPS antibodies. HSP60 has been shown to play a prominent role in chronic inflammation and scarring (45), and anti-LPS antibodies might be indicators of ongoing chlamydia infection (32). Endocervical chlamydia infections in subfertile women In women with asymptomatic endocervical chlamydia infections, ascending spread of micro-organisms from the cervix may cause upper genital tract infections. Women with endocervical chlamydia infections are considered particularly at risk for ascending infections during uterine instrumentation, e.g. HSG and laparoscopy with hydrotubation. Different strategies have been proposed for the prevention of ascending infections in women undergoing uterine instrumentation, including administration of prophylactic antibiotics and a screen-and-treat policy.
Studies published on endocervical chlamydia colonization in subfertile patients,
using DNA amplification tests as polymerase chain reaction (PCR) and ligase
chain reaction (LCR), have reported prevalences of 1.3-1.9% (46,47,48). This
low prevalence makes screening subfertile women for endocervical infections
(and selective treatment of women with positive test results only) not cost-effective
(49). Furthermore, evidence exists that C. trachomatis may persist in a viable and metabolically active state for a long period in the upper genital tract, despite negative PCR results from the cervix (50,51). Reactivation of the micro-organism may cause upper genital tract infection, but it is still speculative which stimuli (including uterine instrumentation) may induce reactivation. If reactivation of chlamydia upper genital tract infections can occur in women in whom no chlamydia DNA can be detected in the cervix, this questions screening by cervical swabs before uterine instrumentation, and also questions considering PCR-negative patients not at risk for upper genital tract infections (48).
Chlamydia IgG antibodies have been found in 30-60% of subfertile women (33), and are regarded as markers for past pelvic infections. Subfertile women with chlamydia antibodies should be considered at risk for reactivation of persistent chlamydia after uterine instrumentation, even after exclusion of chlamydia from the cervix. In subfertile women who have no chlamydia antibodies, the presence of chlamydia in the genital tract cannot be excluded, however. Since iatrogenic spread of chlamydia may have severe consequences for the preservation of fertility, prophylactic antibiotics before uterine instrumentation should be considered in subfertile women, irrespective of the presence of antibodies. Clinical studies which allow for the assessment of the effectiveness of antibiotic therapy in preventing pelvic infections after uterine instrumentation are impracticable, since the majority of chlamydia infections will go undiagnosed. Thus, clinical guidelines concerning precautions in subfertile women undergoing uterine instrumentation can be based on theoretical arguments only. Prophylactic antibiotics (e.g. azithromycin in a single oral 1 gram dose, 12 hours before the planned procedure) have been proposed to replace endocervical screening for C. trachomatis and treatment of positive cases only (48). Chlamydia and male fertility
In males C. trachomatis is a common cause of urethritis. Up to 50% of men who are infected do not experience symptoms (5). Complications of untreated urethritis are epididymitis and prostatitis, but the complication rate has been estimated to be <4% (52). There is no convincing evidence for a relationship between previous chlamydia infection and semen quality (53), and therefore CAT is not helpful in identifying patients at risk for male factor subfertility.
Active chlamydia infections in males are of concern, however, because of the risk of transmission of the micro-organism to female partners. By intercourse, infected males can cause lower genital tract colonization in women and subsequent ascending infections. Furthermore, since C. trachomatis has been shown to adhere to spermatozoa (54), the micro-organism can be introduced directly in the upper female genital tract as well. Therefore, partners of infected males are at increased risk for late sequelae of chlamydia infections. CONCLUSION C. trachomatis is the most common STD. In the majority of women, chlamydia infections occur during adolescence, and remain asymptomatic. These unrecognised and untreated infections increase the risk for tubal factor subfertility at a later age. Since it has shown that tubal pathology is found more often in women with chlamydia IgG antibodies in serum, Chlamydia antibody testing (CAT) has been introduced in the fertility work-up as an inexpensive and non-invasive screening test for tubal factor subfertility. The predictive value of CAT is limited, however. Its diagnostic accuracy is affected by the antibody test used, the cut-off titre chosen for a positive test, and the definition of tubal factor subfertility applied. Unintended cross-reactivity with C. pneumoniae antibodies is still a major cause for false positive CAT results (i.e. positive test results in patients without tubal pathology). Women who undergo uterine instrumentation (e.g. hysterosalpingography and laparoscopy with hydrotubation) are considered at risk for pelvic infections. In subfertile women, the incidence of active chlamydia infections in the cervix is low (1-2%). But despite negative PCR test results from the cervix, the presence of viable chlamydia micro-organisms in the upper genital tract cannot be excluded. Therefore, prophylactic antibiotics before uterine instrumentation should be considered in all subfertile women, instead of endocervical screening for C. trachomatis and treatment of positive cases only. In males, there is no convincing evidence for a relationship between previous chlamydia infection and subfertility. REFERENCES
© Copyright 2004 - Middle East Fertility Society The following images related to this document are available:Photo images[mf04017t1.jpg] |
| |||||||||

{kind=link}