 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 2, 2004, pp. 128-135 Testicular sperm extraction and cryopreservation in patients with non-obstructive azoospermia prior to ovarian stimulation for ICSI Taha Abd Elnaser, M.D. ,Hamsa Rashwan, M.D. Andrology Department and Gynecology and Obstetric Department, Faculty of Medicine, Cairo University and Adam international clinic, Mohandeseen, CairoEgypt. Correspondence: Dr. Taha Abdel Elnaser, 20 Aden Street, Mohandessin, Giza, Egypt. Received on March 21, 2004; Code Number: mf04023 ABSTRACT Objective: To compare between freshly retrieved and
cryopreserved testicular sperm obtained from patients with non-obstructive
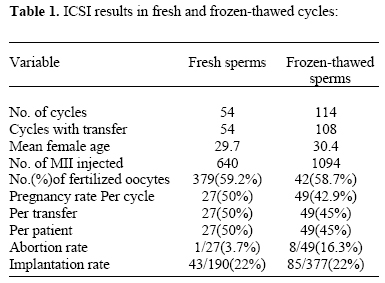
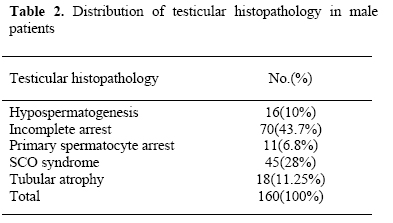
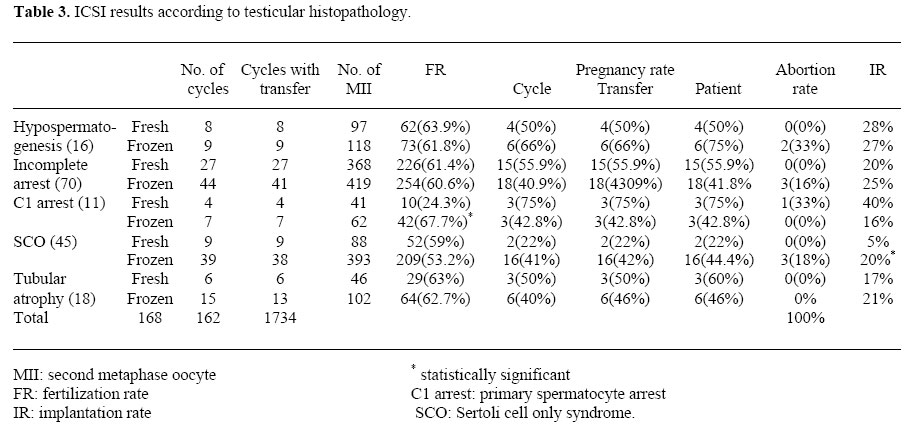
azoospermia (NOA) undergoing intracytoplasmic sperm injection. Key words: Cryopresevation, ICSI, non-obstructive azoospermia, TESE, testicular biopsy. Since its introduction in 1993, the use of testicular sperm for intracytoplasmic sperm injection (ICSI) has become a routine procedure for patients with azoospermia, either suffering from obstructive azoospermia (OA) with normal spermatogenesis, or from non-obstructive azoospermia with testicular failure (NOA) (1,2). In patients with OA, sperm retrieval is always successful and easy either for the first or repeated times, while in patients with NOA, sperm retrieval is variable and is successful in only about 50% of patients. Thus scheduling TESE in the day of ICSI carries the risk of cancellation of the cycle and pointless ovarian stimulation with its financial and psychological complications (3,4). Moreover, TESE in patients with NOA is not completely safe, as it may results in serious complications as hematoma, fibrosis, devasculari-zation and destruction of the marginal sperm production in those patients, with failure of sperm retrieval in repeated attempts for further treatment cycles (5,6,13). Thus, cryopreservation of testicular sperms in patients with NOA before ovarian stimulation of the wife has many clear advantages over planning TESE in the day of ICSI. However, it is anticipated that the quantity and quality of the retrievable sperm will be poor, especially with more severe testicular pathology, that may carry the risk of complete loss of the sperm in the cryo-thawing process (7,8). In addition, the data concerning the outcomes of ICSI using frozen/ thawed testicular sperm are still controversial. While some investigators claim that fertilization and pregnancy rates are lower with frozen/thawed sperms as compared with fresh sperm, others have demonstrated that in obstructive and non-obstructive azoospermic men, cryopreserved sperm function as well as the fresh sperm (4,9-12). The aim of this study is to compare results of ICSI/TESE using fresh and cryopreserved testicular sperm in NOA patients with different testicular histopathology. MATERIALS AND METHODS The study is a retrospective one involving 160 non obstructive azoospermia patients with retrievable sperm during microdissection TESE recruited from Adam international clinic from Jan. 2002 to Jan. 2004, underwent 168 ICSI cycles. According to the patients preference, 54 cycles were done using freshly retrieved sperm and 114 cycles were done with frozen / thawed sperms. The patients were diagnosed as NOA on clinical basis: small sized testes (< 15ml volume), repeated spermograms showing azoospermia, elevated serum FSH level and /or previous histopathology with abnormal spermatogenesis. The patients were counseled either to prepare the wife with ovarian stimulation and perform TESE in the day of ICSI, with the risk of cancellation if no sperm could be retrieved, or to do TESE/cryopreservation if sperms found and prepare the wife 3-6 months later with risk of loss of the cryopreserved sperm and the need to repeat TESE procedure. Accordingly, 53 patients preferred the former option and 107 preferred the later one, routine written consent was taken. Technique of TESE The procedure of TESE was done under general anesthesia using surgical microscope according to the protocol of Amer et al., 2000 (13). After scrotal sterilization, one testis was delivered through vertical skin incision in the median scrotal raphe, the epididymis was inspected to prove non obstruction, stay sutures were placed and small tunical incision was done under optical magnification to avoid large subtunical vessels, the tubules were inspected for homogenousity and presence of dilated tubules, if no dilated tubules were found the incision was enlarged with copious irrigation of the field with Ringer's solution. A piece of testicular tissue was excised from the best looking tubules and put in a petri dish containing ham F10 solution and transferred immediately to the adjacent IVF laboratory for immediate examination. If no sperms found after examination of the whole dish, another piece was taken with maximum of 4 pieces, if still no sperms found, the procedure was repeated on the contralateral testis. A piece of testicular tissue was taken in Bouin's solution for ordinary histopathology. The wound was closed in layers using 4/0 vicryl sutures, skin and dartos was closed using 4/0 chromic catgut sutures. Technique of sperm retrieval The testicular tissue in the petri dish (Falcon cat no 3004, Becton Dickinson, USA) containing one ml HEPES buffered Ham's F10 (Gibco BRL, Scotland) medium was taken directly into the lab, where the tissue was minced using sterile glass slides and shredded with two jeweler forceps's (14) under Olympus stereo microscope (SZ-PT, Tokyo, Japan) aiming at cutting and separating the individual tubules and then examined under an inverted microscope (Olympus IMT2, Tokyo, Japan) with Hoffman optics using 400X magnification for the presence of testicular sperm. The entire petri dish was checked. If no spermatozoa were seen, the squeezed tissues were removed from the petri dish and the remaining medium containing the different tissue cells was collected in 15ml falcon tube (Cat no 2095, Becton Dickinson, USA). The testicular pellet for each biopsy was then resuspended in 2ml of erythrocyte lysing buffer (ELB) for 10 minutes at room temperature (15) after which, 10ml of HEPES buffered Ham's F10 was added to the specimen and centrifuged for 10 minutes at 500g. The pellet was resuspended in 50µl of HEPES buffered ham's F10 and second search for spermatozoa was done by three observers under 3 inverted microscopes in 2µl microdrops covered by sigma oil (M-8410, USA) in falcon petri dishes. The sperm found were either cryopreserved or used for ICSI and the extra sperm were cryopreserved. Technique of cryo-thawing The procedure was performed according to the protocol adopted by Yavetz et al., 1991 (16) using a computer controlled biological freezer (Nicool LM10, France). The freezing medium (Sperm freeze-Fertipro NV, Beernem, Belgium) and the sperm washing medium (HEPES buffered Ham's F10) were removed from the refrigerator and placed in an incubator set at 37° C for 30 min, and the nitrogen dewar of the nicool LM apparatus was filled before each run with controlled run freezing. Testicular sperm sample was diluted (Volume/volume) with the sperm freeze, which was added drop by drop in the side of a falcon tube (Over 10 minutes) to minimize hyperosmotic stress, while continuously shaking the tube. The sperm-medium mixture is transferred in a plastic bubbler dish provided with a comb (IMV, Cat. No. GC000 and GC001). The diluted semen was loaded into straws using an automatic pipette-straws, sealed at one end by a cotton plug, they are provided in 20 colors and have a 250µL volume. After aspiration, each straw was placed on the comb to create an air bubble to avoid explosion of the straw after thawing. Then straws were removed from the comb and sealed by dipping in polyvinyl alcohol powder, which is available in 8 colors (IMV, cat. No A 501-508), the powder sealed ends of the straws are immersed in water, which polymerizes the powder, excess powder and water were wiped off using paper tissue, finally the air bubble is moved to the center of the straw. Straws were labeled individually with the name of the patient, file number, date of cryopreservation and placed in the chamber of the Nicool apparatus and cooled with the freezing program described by Yavetz et al., 1991 (16). The freezing rate was as follow: from room temperature to 10°C at a rate of 1.6°C/m for 6minutes; from 10°C to -120°C at a rate of -5.5°C/min for 20 minutes. The sample was then removed from the controlled rate freezer and plunged directly in the liquid nitrogen storage tank at -196oC. Sperm thawing technique The straw was removed from the liquid nitrogen tank according to the patient’s data, and thawed at 37oC for 1 minute. One end of the straw was cut (sealed with powder) and was placed near the tip of a conical falcon tube and then the other end was cut to let the sample fall into the tube. Three ml of HEPES-buffered Hams F10 medium containing 0.5% Human serum albumin was added slowly drop by drop to the sample, left for 10m at 37oC and then centrifuged at 1800rpm for 10m. the supernatant was removed and the pellet was resuspended in a fixed volume of 200 µL Hams F10 medium. Female preparation and ICSI procedure The female patients were all under the age of 37 years, they underwent ovarian stimulation using a long protocol. Ovarian stimulation was started by pituitary desensitization by GnRH agonist (Decapeptyl or Zoladex) in the midluteal phase (day 21 of the cycle). Hormone determination was carried out after 10 days to confirm baseline concentration of estradiol < 50 pg/ml. Thereafter, stimulation with HMG in a dose of 150- 375 IU/ day was started and continued for 7 days, the doses were subsequently adjusted to individual response and the follicular response was monitored by transvaginal ultrasound. When at least 3 follicles were > 18 mm in diameter, ovulation was induced by administration of 10000 IU of HCG (Choriomon 5000, IBSA, Switzerland). Transvaginal ultrasound guided follicle aspiration was carried out 35 hours after HCG injection. Oocyte preparation The cumulus and corona radiata cells were removed by incubation for 30 seconds in BMI medium ( Eurobio, Italy ), containing 80 IU hyaluronidase/ ml ( Type VIII, specific activity, 320 IU / mg, Sigma chemical co., St. Louis, MO, USA) and by aspiration of the complexes in and out of a FLEXI-PET denuding pipette 130 micron (ID, Cook IVF, Australia). ICSI procedure and assessment ICSI was carried out on the stage of an inverted microscope ( Olympus IX 70, Tokyo, Japan) at 400X magnification using the Hoffman modulation contrast system by the same operator. The procedure of ICSI was performed only on an intact oocyte at second metaphase MII. A single spermatozoon , which was first immobilized by being hit on the tail, was injected into the ooplasm. After 16-18 hours, oocyte was checked under the inverted microscope for the presence of the two pronuclei. At 48 hours after ICSI , embryos were scored for quality according to the percentage of a nucleate fragments and the size of blastomeres into excellent, good, moderate and poor quality embryos (17). Embryo transfer for 3-5 embryos was carried out on either day two or day three post injection using cook embryo transfer catheter ( Cook IVF, Australia), the best embryos were selected for transfer according to embryo morphology and female age considering that implantation rate is significantly decreased in patients with NOA. Luteal phase support was carried out by administration of Progesterone 800 mg / day ( Cyclogest 400mg) from the day of ovum pick up. Pregnancy was diagnosed by measuring serum ? subunit of HCG 16 days after embryo replacement. Clinical pregnancy was determined by observation of gestational sac with fetal heart beats on transvaginal ultrasound at 6-7 weeks of pregnancy. Statistical analysis Statistical analysis was done using an IBM computer and SPSS for MS windows statistical program. Descriptive statistics were presented as means ± standard deviation, as well as frequencies and percentages. Chi- square test for contingency table analysis. P value < 0.05 was considered to be statistically significant. RESULTS A total of 160 patients with NOA underwent 168 cycles of ICSI, 54 cycles were done using freshly retrieved testicular sperms and 114 cycles with frozen-thawed testicular sperms. The mean female age was 29.7 years in fresh cycles vs. 30.49 in cycles with frozen- thawed sperms. The number of mature oocytes (MII) injected were 640 in fresh cycles vs. 1094 in frozen-thawed cycles. The number of fertilized oocytes (FR) were 379 (59.2%) vs. 642 (58.7%) in the two groups respectively with no significant difference (p=0.724). The pregnancy rate per cycle was 50% vs. 42.9% in the two groups respective with no significant difference (p=0.509). The abortion rate was 3.7% vs. 16.3% with P value 0.146, and the implantation rate was 22% in both groups (Table 1). Testicular histopathology was done to all patients and the findings were as follows: 16 patients (10%) had hypospermatogenesis, 70 patients (43.7%) had incomplete spermatogenic arrest, 11 patients (6.8%) had primary spermatocyte arrest, 45 patients (28%) had SCO syndrome and 18 patients (11.25%) had tubular atrophy and hyalinization (Table 2). In the cycles performed with fresh sperms, enough motile sperm were available to inject all oocytes and all cycles ended with embryo transfer, while in cycles performed with frozen- thawed sperms, no motile sperms could be obtained after thawing to inject the available oocytes, and no fertilization or embryo transfer was done in 6 cycles (5.2%), 3 cases with incomplete spermatogenic arrest, one case with SCO syndrome and 2 cases with tubular hyalinization in histopathology. No statistically significant difference in fertilization, implantation and pregnancy rates between cycles with fresh sperm and cycles with frozen-thawed sperm in patients with hypospermatogenesis, incomplete arrest and tubular atrophy was noticed. In patients with primary spermatocyte arrest, significantly higher fertilization rate was found in frozen-thawed group, and also significantly higher implantation rate was found in frozen-thawed cycles in patients with SCO syndrome (Table 3). DISCUSSION Testicular sperm extraction procedure can be used to retrieve spermatozoa from men with NOA in up to 60% of attempts. The use of a combination of TESE and ICSI with testicular spermatozoa from azoospermic men has been reported with a fertilization rate of 43%-47% and pregnancy rate of 20% to 50% of sperm retrieval attempts (18,19). Also, the use of cryopreserved testicular spermatozoa in ICSI has been reported to give rise to clinical pregnancies and an average fertilization rate of 52% which is comparable for that obtained with fresh sperms (10, 20). A prerequisite for the routine cryopreservation of TESE sperm is the demonstration of the post-thaw results and the clinical outcomes comparable to fresh TESE. It has been reported that, although sperm count and morphology were lower in testicular biopsies of men with NOA versus OA, the pre-freeze and post-thaw viability was similar and no difference in ICSI outcome between the 2 groups (21) suggesting that cryopreservation does not adversely affect this procedure. In this study we directly compared ICSI outcome in 2 groups of NOA patients, one group underwent the procedure using freshly retrieved testicular sperms (54 cycles for 53 patients), and the second group underwent the procedure using cryopreserved testicular sperms obtained during previous diagnostic TESE (114 cycles for 107 patients). There was no statistically significant difference in fertilization rate (59.2% VS 58.7% P = 0.724), implantation rate (22% in both groups), clinical pregnancy rate (50% VS 42.9% / cycle, P =0.509) and spontaneous abortion rate (3.7% VS 16.3%, P = 0.146) between both groups. Also testicular pathology and the degree of impairment of spermatogenesis did not affect ICSI outcomes, as there was no statistically significant difference in ICSI parameters in all histopathological groups, except significantly higher fertilization rate with cryopreserved sperms from primary spermatocyte arrest group & significantly higher implantation rate with cryopreserved sperm from cases with SCO group, which we attributed to possibility of better sperm quality that survived the cryo-thawing process. These results are in agreement and has been supported by many authors who suggested to do diagnostic TESE and freezing routinely before ovarian stimulation particularly in absence of clinical or laboratory criteria that are highly predictive for TESE outcome in patients with NOA (21-27). But these results are in disagreement with reports of poor results of ICSI outcome in all patients with NOA (28) and particularly those with cryo thawed testicular sperm (8,29). To account for these discrepancies is that the cryopreservation methods and techniques are variable between different centers and that freeze/thaw techniques for TESE sperm can significantly be detrimental for ICSI outcome. Moreover, the post-thawing laboratory work at the day of oocyte pick up may be extremely difficult and time consuming that may delay the Intracytoplasmic injection procedure and this may result in flattening and fragmentation of the first polar body of the oocytes with a higher incidence of abnormal fertilization and poor embryo quality (30). Another important concern is the post-thaw loss of all cryopreserved sperm, which has been reported to range from 9%-68% and may lead to cycle cancellation (8,23). In our study, this was found in 5.2% of cycles performed with cryopreserved sperm, this is most probably related to the pre-freeze sperm parameters. In a previous study we have reported that the minimal sperm parameters for effective freezing is total sperm count of 144, and total motile sperm count of 41 sperm, to ensure post-thaw motile sperm enough to inject all the available oocytes the day of ICSI (31). Freezing of testicular spermatozoa provides several advantages. First, in 26%-64% of patients with NOA, no sperm can be obtained from testicular biopsy (4,19). Since there are no definite clinical parameters to predict availability of sperm in NOA, the couple can be saved emotional and financial complications (by freezing of TESE sperm) if no sperm are retrieved during concurrent fresh TESE. Second, repeated testicular biopsies may cause damage to the testis and failure of sperm retrieval with repeated attempts (6). Since cryopreservation of TESE specimens allows storage of multiple straws, multiple attempts of ICSI cycles can be achieved from single diagnostic biopsy procedure. Third, no co-ordination of two surgical procedures, TESE and oocyte retrieval, for concomitant ICSI procedure is necessary when frozen- thawed sperm are used. Finally, in patients with solitary testis scheduled for surgical radical orchiectomy because of cancer and have azoospermia or severely impaired semen parameters, freezing of TESE sperms can save their fertility potential (32).
In conclusion, the present study found no significant difference between fresh and frozen-thawed TESE sperm from patients with NOA with regards to fertilization, embryo cleavage, pregnancy and spontaneous abortion rates. Thus, with consideration of the advantages of sperm freezing, routine cryopreservation of testicular sperm at the time of diagnostic testis biopsy seems to be a convenient, cost effective and more advantageous for patients with non-obstructive azoospermia. ACKNOWLEDGMENT The authors are greatly indebted to Dr. Giergis Abdelmalak and Dr. Emad Fakhry from the IVF laboratory of Adam international clinic and their colleagues for their generous effort in conducting the practical part of this work. Also, thanks to Dr. Medhat Amer and Dr. Wael Zohdy from the Andrology team for their kind help and support in revising this work. REFERENCES
© Copyright 2004 - Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}