 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 2, 2004, pp. 136-139 Acanthosis nigricans as skin manifestation of polycystic ovaries syndrome in primary infertile females Khalifa E. Sharquie, M.B.Ch.B., Ph.D.*,Ansma Al-Bayatti, M.B.Ch.B., Ph.D., D.D.V.†,Awatif J. Al-Bahar, M.B.Ch.B., F.A.H.K.A.R.T.‡,Qais M. A. Al-Zaidi, M.B.Ch.B.* Departments of Dermatology and Venereology, and Biochemistry, College of Medicine, University of Baghdad, Baghdad, Iraq * Department of Dermatologyh and Venereology, College of Medicine,
University of Baghdad. Correspondence: Ansam A. Al-Bayatti, M.B.Ch.B., Ph.D., D.D.V. Assist. Professor and chairman of Biochemistry Department, College of Medicine, University of Baghdad, postal code number 12114, Medical collection post office, Baghdad, Iraq. Tel: 00 964 1 5560036, Fax: 0047 24136110. E-mail: ansimalaad@yahoo.com Received on December 15, 2003; Code Number: mf04024 ABSTRACT Objective: The present work is to record the frequency of Acanthosis
Nigricans (AN) among patients with Polycystic Ovaries Syndrome (PCOS), and
to observe the frequency of PCOS among patients with AN. and to study the association
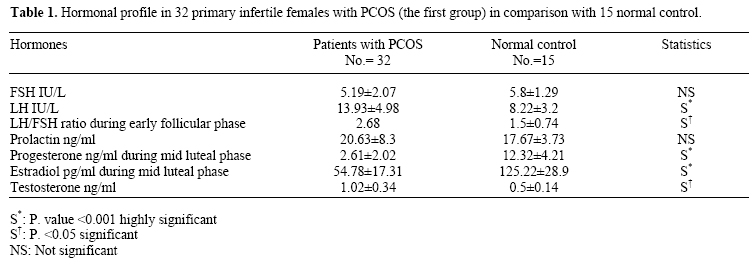
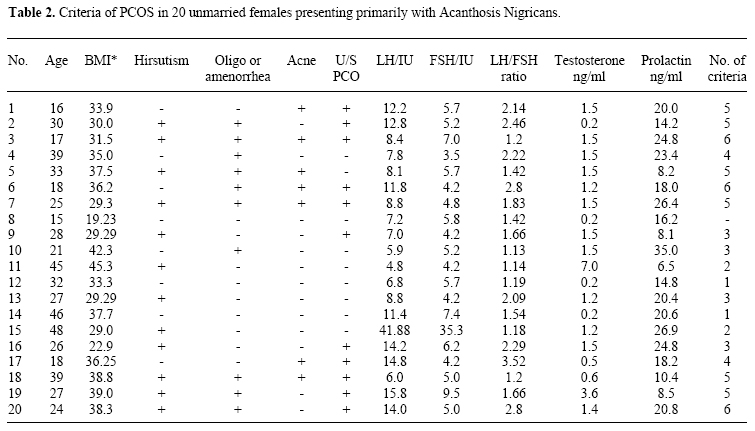
between AN & PCOS Key word: Acanthosis Nigricans, Polycytic Ovaries Syndrome, Primary Infertility Acanthosis Nigrcians (AN) is not an uncommon dermatological problem. Its etiology is still unknown, so called idiopathic but there are many associated abnormalities that could be seen like hormonal changes and malignancies (1-3). The diagnosis of this problem is mainly clinical by observation of hyperpigmented verrucous plagues with a velvety texture symmetrically distributed in the intertriginous areas including the neck, axilla, groin and umbilicus, and occasionally it may involve the oral and anogenital mucosa (1). Polycystic ovaries syndrome (PCOS) characterized by obesity, infertility, acne, hirsutism, amenorrhea or oligomenorrhoea, raised LH/FSH ratio of more than 2:1 and PCO by ultrasonography (2,5,6). The aim of the present work was to record the frequency of AN among patients with Polycystic Ovaries Syndrome (PCOS) and to observe the frequency of PCOS among patients with AN. MATERIALS AND METHODS This study included two groups of patients in addition to apparently 15 fertile healthy females as a control. The first group consisted of thirty-two females with primary infertility and PCOS. Full history was done for all patients concentrating on the following criteria: obesity (Body Mass Index (BMI) equal to or more than 30 were considered to be obese) (7), infertility, acne, hirsutism, and oligo or amenorrhea. A thorough physical examination was done for all patients. Also, hormonal profile including Follicular Stimulating Hormone(FSH), Leutinizing Hormone(LH), LH/FSH (ratio during early follicular phase), testosterone, progesterone (during mid luteal phase), estradiol (during mid luteal phase), and prolactin. Abdominal and pelvic ultrasonography was done for all patients. The diagnosis of PCOS was done by demonstration of 3 or more of the following criteria: (obesity, infertility, acne, hirsutism, oligomenorrhea or amenorrhea, LH/FSH ratio of more than 2:1, elevated or normal testosterone level, normal or mildly elevated prolactin level, and consistent ultrasonographic changes of PCO). The necks and axillae of these patients were screened for AN. The second group consisted of twenty unmarried females presented with AN. The diagnosis of AN was done clinically and confirmed by histopathological examination. These patients were screened for clinical features of PCOS. Furthermore, hormonal profile (LH, FSH, LH/FSH ratio, prolactin and testosterone levels) and ultrasonography were done for these patients. RESULTS The first group: this group included 32 primary infertile females with PCOS. Their ages ranged from 18-33 years with a mean ± SD of 25.8 ±7.2. Hormonal profile showed that the ratio of LH/FSH was greater than 2:1 with low progesterone level (Table 1). Ultrasonography showed changes of PCOS. AN of the necks and axillae was noticed in 22(68.75%) of patients. The second group: this group included 20 unmarried females with benign AN. Their ages ranged from 16-48 years with a mean ± SD of 18.55 ± 3.73. Fifteen patients (75%) had more than 3 criteria of PCOS. Obesity (as measured by BMI) was seen in 13 (65%) of patients, hirsutism was recorded in 12 (60%) of patients, menstrual irregularities (oligomenorrhea or amenorrhea) were reported in 10(50%) of patients, and acne was noticed in 7 (35%) of patients. Ultrasonography with features of PCO was reported in 11 (55%) of patients. Regarding the hormonal profile; thirteen patients (65%) sowed high testosterone level, 8(40%) of patients showed LH/FSH ratio of more than 2:1, and 9 (45%) of patient had high prolactin level (Table 2). DISCUSSION The incidence and prevalence of AN in the general population is not yet known (6, 7). Also, its actual incidence among Iraqi people is not studied but AN seems to be not uncommon problem. AN is classified into hereditary benign AN, syndromic AN (associated with insulin resistance), pseudo-AN (obesity- related), drug-induced AN (nicotinic acid, estrogen and steroids), and malignant AN (Adencarcinoma of the stomach and Lymphoma) (4, 8-11). PCOS is a very common problem among Iraqi females but unfortunately the association with AN was not recognized before. In the present work, AN was observed in 68.75% of patients with PCOS and this is a very surprising figure and may confirm a close association between the two conditions. The association of PCOS with AN is well recognized in many countries (12). Similarly this association was shown in this study as it was noticed in 75% of patients with AN, but this figure is very high when compared to other countries (11). AN might precede the other features of PCOS and could be an alarming sign of this condition. So, in conclusion, the present work had shown a significant association of AN with PCOS and AN should be considered as an important skin marker and a major feature of PCOS. REFERENCES
© Copyright 2004 - Middle East Fertility Society The following images related to this document are available:Photo images[mf04024t2.jpg] [mf04024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}