 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 2, 2004, pp. 140-149 Transvaginal ultrasound appearance of the ovary in infertile women with oligomenorrhea: association with clinical and endocrine profiles Ahmed Aboul Nasr, M.D.,Hesham Hamzah, M.D.,Zakaria Abou El Maaty, M.D.,Hesham Gaber, M.D.,Omniah Azzam, M.D. Department of Obstetrics & Gynecology, CairoUniversity, Cairo, Egypt Contact address: Hesham Al-Inany, 8 Moustapha Hassanin st, Manial, Cairo11451, Egypt E-mail: Kaainih@link.net Received on October 23, 2002; Code Number: mf04025 ABSTRACT Objective: to assess the morphological findings of the ovary based
on transvaginal ultrasound in infertile oligomenorrheic women and their predictivity
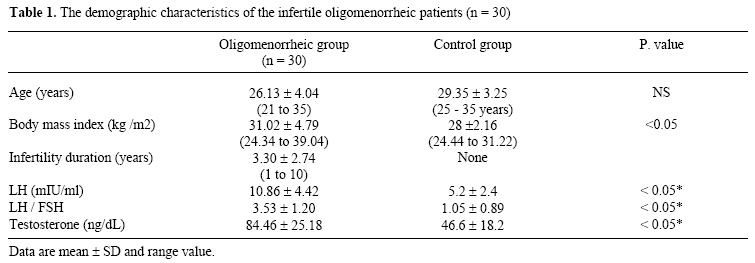
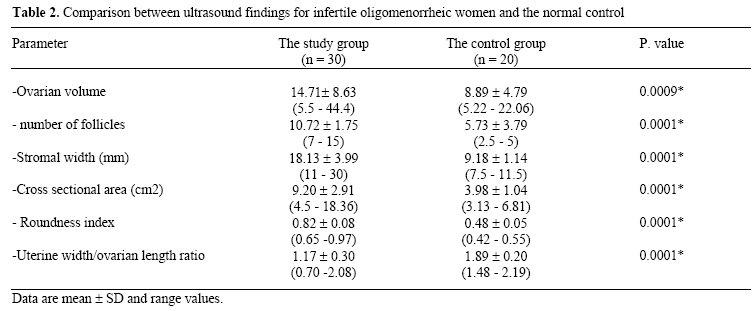
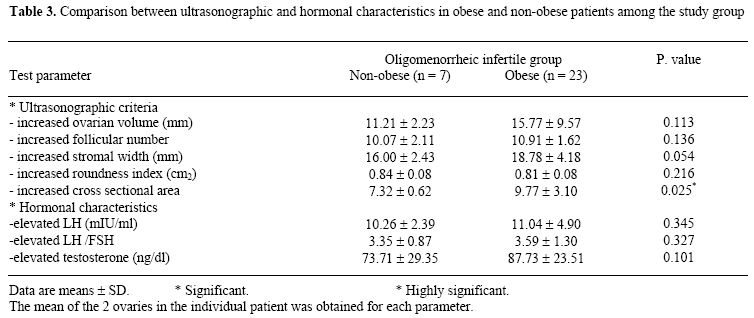
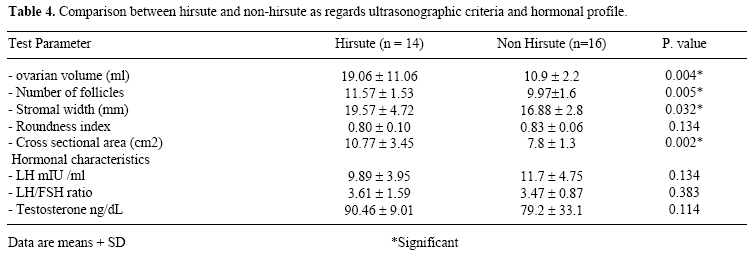
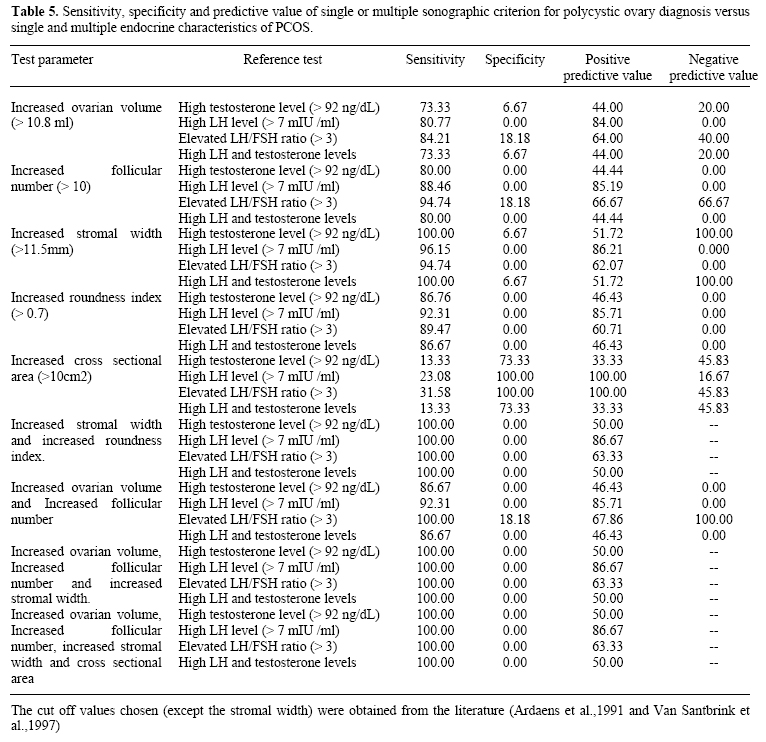
for endocrine signs of polycystic ovary syndrome Keywords: Oligomenorrhea, PCOS, infertility, transvaginal ultrasound. Hyperandrogenaemia. Oligomenorrhea is usually defined by menstrual intervals between 6 weeks and 6 months. This definition is, however, arbitrary and does not necessarily reflect important distinctions, indeed, they can be misleading (1). Therefore, oligomenorrhea includes a spectrum of conditions ranging from virtual normality at one end to the same causes as amenorrhea at the other. The main difference appears to be in the frequency of polycystic ovaries, which ultrasound and endocrine studies show account for about 90% of cases of oligomenorrhea and 33% of amenorrhea, although often without the classical syndrome, including hirsutism and obesity (1). It is also recognized, however that, many women with polycystic ovaries are endocrinologically normal. In one population-based study of 190 women, no differences in menstrual cycle pattern or prior fertility were found between women with polycystic ovaries and those with normal appearing ovaries (2). Oligomenorrhea may alternatively be used as a functional marker for PCOS. Biochemical evidence of androgen excess was reported in 40% of non-hirsute oligo-ovulatory women in one study Allen et al. (3), whereas in another report, 90% of women with oligomenorrhea were considered to have PCOS on the basis of concomitant hirsutism, estrogen status and luteinizing hormone (LH) to follicle-stimulating hormone (FSH) ratio (1). Because of the broad spectrum of clinical presentation of PCOS, including eumenorrhoeic non-hirsute women troubled only by recurrent miscarriage, and because of the lack of any reliable simple tests, assessment of ovarian morphology has assumed critical importance for the categorization of women with ovarian disorder (4). The aim of this study is to determine the range of appearances of the ovary in infertile oligomenorrheic patients and apparently normal women using high-resolution transvaginal ultrasonography and to investigate the predictive value of polycystic ovaries for endocrine signs of polycystic ovary syndrome (PCOS). MATERIALS AND METHODS Two consecutive series of young women (21-35 years) were recruited for study prospectively; one group with oligomenorrhea and elevated serum concentration of LH and a control group of apparently normal women (non-hirsute, non-obese, normal menstrual rhythm and normal serum concentrations of LH). Normal menstrual rhythm was defined as cycle length of 21-35 days and intercycle variability of less than 5 days. Hair growth was assessed clinically using scoring system described by Ferriman and Gallway. Nonhirsutism was defined by a score of 5 or less and unequivocal hirsutism by a score of 12 or more to avoid any overlap with normal variation in hair ngrowth. Obesity was defined as body-mass index greater than 25 kg/m2. None of the women had been pregnant in the previous year or received hormonal therapy in the preceding 6 month. Each patient was scanned with a transvaginal endoprobe (Siemens, 5 MHz). The scans were undertaken within the first 5 days of the menstrual cycle of those with normal menstrual rhythm and at random in those with oligomenorrhea. The maximum longitudinal and transverse diameters of each ovary were measured and volume was calculated according to the formula: Volume= 0.5xd1xd2xd3 (d1,2,3= diameters of the ovary in 3 perpendicular planes).. When possible, the maximum transverse diameter of brightly echogenic stromal tissue was measured. Follicular diameter was calculated as the mean of the maximum measurement in 3 perpendicular planes. The number and distribution in each ovary of follicles up to 10 mm were recorded. Cross sectional area of the ovary was calculated from the formula= length x width x #/4. Roundness index = ovarian width/ovarian length. The mean measurements of both ovaries were used for comparison. Also the uterine width/ovarian length was recorded. Hormonal assessment: Blood was analyzed for follicle-stimulating hormone (FSH), luterinizing hormone (LH) and total testosterone (T) concentrations. The samples were taken in the early follicular phase in the women with normal menstrual rhythm, and at random in the women with oligomenorrhea. In those with oligomenorrhea the venous sampling was ultimately timed retrospectively from any ensuring period to ensure that the blood had not been taken during the preovulatory phase. Serum LH and FSH concentrations were determined by specific radioimmunoassays (RIA) using polyclonal rabbit antisera (WRB/F87 for LH and M93/6873 for FSH; Pharmacia Diagnostic), standardized against international reference preparations. Following ether extraction, (T) was measured by specific RIA using polycolonal anti-sera (HP/5/55/1A sheep anti serum, University of Surrey, Guildford). Statistical analysis Data were statistically represented in terms of range, mean, standard deviation (SD), median and percentages. Comparison between different groups in the present study was done using Student t test for comparing parametric data. For comparing non-parametric data, Chi square (2) test was performed. Yates correction was used instead when the frequency is less than 10. Accuracy was represented using the terms sensitivity, specificity, positive predictive value, and negative predictive value . A probability values (p value) less than 0.05 was considered significant. All statistical calculations were done using computer programs Microsoft Excel version 7 and SPSS (Statistical Package for the Social Science) statistical program. The study was approved by the local Ethics Committee of Obstetrics and Gynecology Department of Kasr El-Aini Hospital. RESULTS The background characteristics of our participants are presented in Table I. There was a statistically significant difference between different transvaginal criteria in the 2 groups (Table 2). There was no statistically significant difference between obese and non-obese in the study group as regards all ultrasonography parameters except for increased cross sectional area (P= 0.025) (Table 3). There were 14 patients (46.7%) in the study group with hirsutism. There was statistically significant difference between hirsute and non-hirsute women as regards all ultrasonographic parameters except roundness index. There was no statistically significant difference between the two groups as regards all hormonal profile (Table 4). Twenty-five (83%) patients of the study group had ovarian volume > 10.8 ml ; 27 (90%) had follicle number > 10. Twenty-nine (96%) had stromal width > 11.5 ml; six (2%) patients had cross sectional area > 10 cm2 and twenty eight (93%) patients had roundness index > 0.7. Interestingly four patients (20%) in the control group had number of follicles > 10, however there was no patient in the study group having follicle number less than 7. Two patients (6.7%) in the control group had number of follicles and ovarian volume below the PCO limit but had increased amount of stroma and increased roundness index. Interestingly these 2 patients had high LH and testosterone levels but normal LH/FSH ratio. Increased stromal width showed the highest sensitivity amongst all the ultrasonographic morphological criteria with highest negative predictive value for elevated testosterone and elevated both testosterone and LH. Increased cross sectional area was the least sensitive but with the highest specificity. (Table 5), when one or more of the ultrasonographic criteria were combined sensitivity increased especially when the combination included increased stromal width. However, this came on the expense of the specificity (Table 5). DISCUSSION The polycystic ovary (PCO) is one manifestation of a functional disorder of the hypothalamo-pituitary- ovarian axis characterized by hypersecretion of luteinizing hormone (LH), ovarian and adrenal androgens (5). Because of the broad spectrum of clinical presentation, including eumenorrheic non-hirsute women troubled only by recurrent miscarriage, and because of the lack of any reliable simple endocrine test (4), assessment of ovarian morphology has assumed critical importance for the categorization of women with ovarian disorder. Ultrasonography has enabled detailed noninvasive assessment of ovarian morphology. The vaginal route improves the ultrasound study of internal ovarian PCOS criteria (polycystic appearance, abnormal ovarian stroma). On the other hand, the external ovarian PCOS features (increased ovarian area, uterine width/ovarian length and, excessive roundness index) are equally evaluated by abdominal route, more especially the uterine width / ovarian length ratio because one can visualize the uterus and the ovaries on the same section by this route. Conversely, the narrow-ness of the sectional field with vaginal probe does not always allow to see enlarged ovaries in their totality, impairing a reliable measurement of the larger ovarian axis. Furthermore, it may happen that ovaries are located at the upper part of the pelvis and thus not visible with the vaginal probe. Fortunately, the detection rate of ovaries in the present study was 100%. However, it is reasonable to consider the recommendation of Ardaens et al. (6), that abdominal ultrasound is needed before scanning patients vaginally. In the present study the polycystic ovaries could be observed in 20% of the control population. This was in agreement with several other studies (7-9) that showed prevalence rate of approximately 22%. Several groups have described ultrasound criteria for the diagnosis of PCOS (10-12) but no consensus has been reached. Scanning transabdominally Treasure et al.,1985 and Yeh et al., 1987 (11,12) suggested that as few as 5 follicles in each ovary was sufficient for the diagnosis to be made. Fox (1999) (13), using transvaginal ultrasound stated that if there were 15 or more small follicles per ovary, the diagnosis of PCOS could be made with confidence but below that number there was no clear demarcation in follicularity between normal women and those with clinical and laboratory evidence of PCOS, with some oligomenorrheic hirsute women having ovaries with normal follicularity. In the present study only 4 patients (13.3%) among the study group[ had follicular number equal to or more than 15. Like Ardaens (6) and Van Santbrink et al. (14), follicular number >10 was adopted in this study. Ninety percent were found to have follicular number >10, unlike (14) who found 58% of 330 normogonadotrophic oligomenorrheic or amenorrheic women with infertility having follicle number > 10. This difference could be explained by small number of the present study (30 patients versus 330 ) in there study. Eighty-three percent of our study group showed increased ovarian volume compared to 41% in the study of Van Santbrink et al. (14). Likewise, increased stroma was observed in 96% in the present study compared to 45% in their study. Most researchers had concentrated on measurement of ovarian follicularity and volume because these are relatively easy to quantify. The ovarian stroma may prove to be a more useful morphological test of ovarian dysfunction (15). In the present study it was possible to take measurement of the stromal width of all patients in the study group unlike 60% in the study of Fox (13). This difference was because of the inability to take measurement in the presence of follicles interspersed within the stromal tissue. In this study all patients showed the picture of central stromal hypertrophy that push the microcysts toward the tunica albuginea. This enabled easier measurement of the stromal width. One may argue that the evaluation of the stroma is purely visual and, therefore, rather subjective. This is avoided, however, by the very typical appearance of the stroma in PCOS by means of vaginal ultrasound. This was observed in the 4 patients in the control group who showed increased follicularity but lack the echo-dense central stroma. Unlike the 2 patients in the study group who showed follicularity and ovarian volume below the limit of PCO but had increased amount of echo-dense stroma. Interestingly these 2 patients had high LH and testosterone levels. With advances in computer-assisted interpretation of the images obtained from TVS, it will become possible to calculate the surface area of a single plane of the ovary occupied by stroma (15). In the present study we used a cut off value of 11.5 cm for stromal width obtained as the 95th centile of the control population aiming to get an objective way to evaluate this sign. The advantage of having an objective measurement of the stroma would be that it would be possible to define hyperandrogenetic ovaries with normal follicularity. In the present study it was observed that stromal width overlapped with increased ovarian volume, follicularity, roundness index and cross sectional area in 100%, 96.3%, 96,43% and 100% respectively. This means that you will never found increased ovarian volume or increased cross sectional area without increased stroma. Dewailly et al. (15), suggested that the ovarian hypertrophy results primarily from excessive ovarian stroma resulting from increased rate of atresia and mush less from thee abundance of microcysts. Unlike the data of others (16-18), the uterine width /ovarian length ratio <1 was present in only a minority of patients in the present study. This was in accordance with (6). They also found ratio <1 in some patients with hypothalamic anovulation in whom the uterine section was small because of their hypoestrogenic state. Although there was a statistically significant difference between study and control groups as regard the cross sectional area of the ovary, it was increased only (>10cm2) in 20% of patients in the study group. This was in accordance with Ardaens et al. (6), but in disagreement with Orsini et al. (18) and El-Tabbakh et al. (19), who used lower threshold. Twenty-three patient (76.7%) in the study group were overweight (BMI>25 kg/m2).There was no statistically significant difference between obese and non-obese patients in the study group as regards hormonal and ultrasonographic characteristics except for increased stromal width (P = 0.054). This was in accordance with Pache et al. (20), who could not find relationship between BMI and follicle number, ovarian volume and stroma echogenicity or between BMI and testosterone. Unlike the results of Balen et al. (21), who found higher BMI was associated with a rise in serum testosterone concentration and was significantly correlated with ovarian volume. Also higher BMI was associated with prevalence of hirsutism. Although 12 patients (52.17%) were hirsute among obese patients compared to 2 (28.57%) among non-obese patients in the present study. This was statistically non-significant, i.e. there was no statistically significant difference between obese and non-obese in all ultrasound criteria and all hormonal profile. In the present study hirsutism was present in 14 patients (46.7%) of the infertile oligomenorrheic group (study group). There was statistically significant difference between hirsute and non-hirsute patients as regards number of follicles (P = 0.005), ovarian volume (P = 0.004), stromal width (P= 0.032), and cross sectional area (P=0.002), but not with roundness index (P = 0.134). This was in accordance with Pache et al. (20), who found hirsutism positively correlated with all ultrasonogaraphic features of PCO (number of follicle, ovarian volume and increased stromal echogenicity). However, there was no statistically significant difference between hirsute and non-hirsute subgroups as regards LH and T levels, and LH/FSH ratio. Excessive androgen production is the most constant feature of PCOS, the ovaries being the main source (22). Not all patients are androgenized, however, expression of hyperandrogenemia such as virilization depends, in part, on the rate of peripheral conversion of testosterone to dihydrotestosterone in androgen dependant end organs (23). Fox et al. (4), stated that measurement of serum androgens is more useful than assessment of hair growth, particularly if the free component is calculated. In term of diagnostic accuracy, the free androgen index (FAI) alone or in combination with LH is the most useful biochemical test. This requires measurement of both testosterone and SHBG. However, the application of this test is hided by the limited availability of the SHBG assay. It this study total testosterone was assayed. In their comprehensive study Conway et al. (24), reported that, only 50% of patients with ultrasonographically diagnosed PCO had the most classical endocrine features of PCOS, namely elevated serum T and/or LH levels. Similar findings were emphasized in an earlier report by Swanson et al. (25). In the present study there were comparable results. Considering one or more of the usually used ultrasound criteria (number of follicles, ovarian volume and increased stroma ) to diagnose PCO, high testosterone (> 92ng/dl), high LH (> 7mIU/ml), high LH/FSH ratio and high both LH and testosterone levels were found in 50%, 86.7%, 63.3%, 50% respectively. Addition of cross sectional area and/or roundness index does not change these results. Robinson et al. (26), described the endocrine profiles of 63 women with clinical and ultrasound features of PCOS and found that, serum testosterone, androstenedione or LH concentration were elevated either alone, or in combination, in 86% of women and the LH/FSH ratio was of little value. Androgens are synthesized in theca and stroma cells. An increased rate of atresia, with consecutive augmentation of ovarian volume, is presumably part of the mechanisms leading to polycystic transformation of ovaries (27). Balen et al. (28), found that serum concentrations of LH and testosterone did correlate significantly with ovarian volume. There were many studies some are in agreement with Berger et al. (29), and others not in agreement with Givens et al. (30); Franks (5), an association between ovarian size and serum LH concentration. In the present study high testosterone was observed in 44% of patients with increased ovarian volume while high LH was observed in 88%. Elevated LH concentration and slightly decreased FSH concentration are well-established criteria for PCOS diagnosis. This also can be expressed as LH/FSH ratio. Different cutoff levels for LH/FSH ratio have been used by different authors. Gadir et al. (31), used >2 as cutoff level. Fox et al. (4), used >2.5 as cutoff level, however, they claimed that the best critical level for LH/FSH ratio was just 1. In their study nearly half the patients with PCO had ratios below 2.5 for which criterion the overall diagnostic accuracy was only 66% using their newly set criterion (>1.5) they expected that the diagnostic accuracy would appear to be 89%. Ardaens et al. (6), used LH/FSH ratio >3 after gonadotropin releasing hormone stimulation. In the present study LH/FSH ratio >3 was present in 63.33% of patients in the study group. Although this ratio has been used as an important diagnostic criterion in some studies (4), other studies showed reduced emphasis on measurements of serum gonadotropin concentrations for PCOS diagnosis (23). Pulstile release of LH, as well as, timing of blood withdrawal and assay variability (RIA versus IRMA) makes it questionable to use this parameter as the sole diagnostic criterion (26, 32). Van Santbrink et al. (14), found 85% of patients presenting with elevated serum LH levels suffered from polycystic ovaries and/or elevated serum androgens. In the present study approximately 80.8% of patients presenting with elevated LH had PCO if the same criteria were used as VanSantbrink (ovarian volume and/or number follicles). This figure increases if stromal width and/or roundness index is added to the diagnostic criteria. Only 57.7% of patients with elevated LH level had elevated serum testosterone. This was in accordance with approximately 50% of patients with elevated LH level having high androgen level in the study of (14). Fauser et al. (32), noted that up to 40% of women with clinical and endocrine signs of PCOS exhibit immunoreactive LH levels within normal limits. These observations may indirectly favor the concept of intraovarian dysregulation as a major cause of polycystic transformation of the ovaries (27,33).In the present study there were approximately 13.3% of patients who have PCO on ultrasound with normal LH level. Because a good screening test must have high sensitivity (i.e., percentage the test indicates presence of the disease of the total disease group) rather than specificity, Van Santbrink et al. (14), found mean follicle number as a single test and mean follicle number and/or ovarian volume as combined test appear the most favorable screening test to predict endocrine abnormalities characteristic for PCOS. In the present study all ultrasonographic criteria for PCO as a single test except for increased cross sectional area showed high sensitivity even more than that of Van Santbrink et al. (14). However, this came on the expense of specificity. This was marked when combinations were used where sensitivity reached 100% while specificity declined 0%. This was evident when increased stromal width was included in the combination test. As a conclusion a wide spectrum of ultrasonographic ovarian findings can be demonstrated in PCOS, extending from apparently normal to markedly enlarged cystic ovaries. In addition some women show sonographic signs of PCO without hyperandrogenemia, others are hyperandrogenemic without clinical symptoms and without typical sonographic PCOS signs. Thus, PCOS does not seem to be a single homogenous entity of disease. Although this study tried to demonstrate the importance of a vaginal sonography as screening method to evaluate the PCOS, the ultrasonic criteria for diagnosis of PCOS including a number of factors must be further evaluated in a prospective study including a large series of patients with special emphasis on abnormal ovarian stroma. Being highly improved by vaginal endosonography, it is recommended to search carefully for this sign in all hyperandrogenic, and/or, anovulatory patients and not only in these previously suspected to have PCOS on the basis of an arbitrary clinical and/or endocrine classification. This is especially if a proper quantitative method is used. REFERENCES
© Copyright 2004 - Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}