 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 2, 2004, pp. 157-162 Letrozole induction of ovulation in clomiphene citrate resistant polycystic ovary syndrome: responders and non-responders Aboubakr Elnashar, M.D.,Hany Fouad, M.D.,Magdy Eldosoky, M.D.,Naser Abelgafar, M.S. BenhaUniversityHospital Clinic, Benha, Egypt. Reprint requests: Aboubakr Elnashar, M.D., 24 Gomhoria st., Mansoura, Egypt. Fax: +002502331911, E-mail: elnashar53@hotmail.com Received on December 14, 2003; Code Number: mf04027 ABSTRACT Objective: To evaluate the efficacy of Letrozole in induction of ovulation
in cases of CC-resistant PCOS and to compare between Letrozole responders and
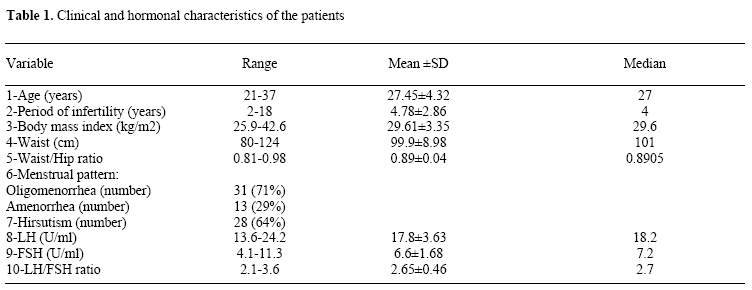
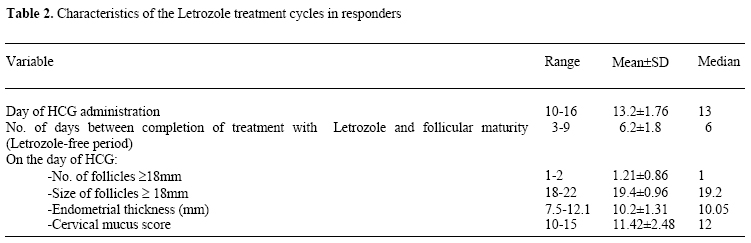
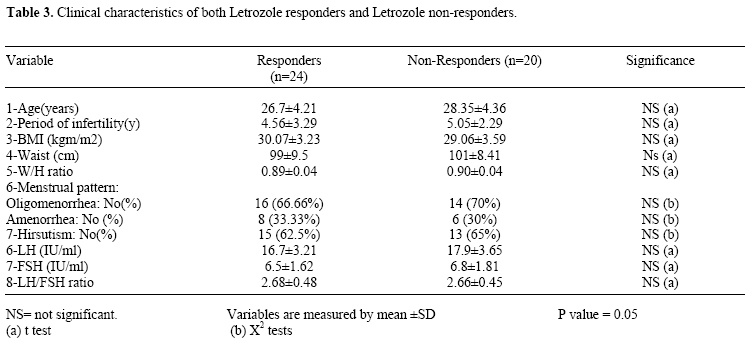
non-responders. Key Words: Letrozole, clomiphene citrate, PCOS, ovulation, infertility Clomiphene citrate (CC) is the traditional first-line treatment for the chronic anovulation that characterizes PCOS (1). CC is accumulated in the body with low clearance rate and long half-life (5 days). Significant plasma concentrations of the active zu isomer of CC can be detected up to 6 weeks after administration. However, 20-25% of PCOS women fail to ovulate with incremental doses of CC, in addition clinical data revealed a discrepancy between ovulation rates (75-80%) and conception rates (30- 40%) during CC treatment (2). For these patients, there are a few limited adjunctive therapies that can be tried before moving on to gonadotropin therapy or laparoscopic ovarian drilling including; bromocriptine (in the presence of hyperpolactinemia or galactorrhea), dexamethasone (to reduce adrenal androgen production), insulin sensitizers (to treat hyperinsulinemia), oral contraceptives (for pretreatment suppression of LH), pulsatile GnRH (to preserve physiologic interactive feedback) and extended doses of CC (3). However, their usefulness is limited to specific abnormalities, as many women with CC-failure do not present with any overt signs of a treatable disorder (4). Mitwally and Casper had reported the novel use of the aromatase inhibitor Letrozole for inducing ovulation in anovulatory women with PCOS and for augmenting ovulation in ovulatory infertile women (1). Letrozole belongs to a new group of very potent, non-steroidal aromatase inhibitor that is rapidly absorbed from the gastrointestinal tract and excreted by the kidney. The elimination half-life of Letrozole is about 2 days (5). Our objective was to evaluate the efficacy of Letrozole in induction of ovulation in cases of CC-resistant PCOS and to compare between Letrozole responders and non-responders. MATERIALS AND METHODS Forty-four infertile women were selected from the patients attending the outpatient clinic of Benha University Hospital. All patients were diagnosed as having anovulation due to PCOS. PCOS was diagnosed when the ultrasonographic findings of PCOS (>10 cysts, 2-8mm in diameter scattered either around or through an echodense, thickened central stroma) are present plus one or more of the following: oligo/amenorrhea with positive progesterone withdrawal bleeding, hirsutism/acne, obesity, raised LH/FSH ratio >2, or raised circulating androgens (Balen, 1999). All patients had previously received CC and diagnosed as having CC-failure (failure of ovulation after 6 cycles of CC reaching the dose of 150 mg daily) (3). Our inclusion criteria:1- Age: between 18-39 years. 2- Period of infertility > 2 years. 3- Serum level of FSH <12 U/L and serum prolactin level were within normal limits in the early follicular phase. Exclusion criteria were history of pelvic surgery or infertility factor other than anovulation. Hirsutism was diagnosed when the Ferriman & Gallwey score is >8 (3). A two-month washout period before the Letrozole treatment cycle was used to eliminate any post-treatment effect of CC. Patients were examined generally, abdominally and locally. Weight, height, waist and hip circumferences were measured. A transvaginal ultrasound examination was performed to exclude any pelvic pathology before treatment with Letrozole. Ultrasonography was performed using Medison Scan, Sonoace 5500 with a transvaginal transducer 6.5MHz (Medison, Korea). In all patients, Letrozole (Femara; Novartis, East Hanover, NJ) was given orally in a dose of 2.5 mg/day for 5 days starting from the third day of a spontaneous or progesterone induced menstrual bleeding (6). Ovarian follicular response was monitored by transvaginal sonography starting on the next day after finishing Letrozole and thereafter according to the growth of the follicles (usually every other day). Good response was achieved when at least one mature follicle becomes > 18 mm in diameter (Speroff et al, 1999). When the optimal follicle size was reached the endometrial thickness and cervical mucus score were assessed and HCG 10.000 U (Pregnyl; Organon, Holland) was given intramuscular and timed intercourse was advised. Endometrial thickness was assessed according to Gonen and Casper (7). Cervical mucus score was evaluated for each responding patient at the day of HCG administration. An evaluation of the cervical mucus was calculated according to Moghissi (8). Cervical mucus score was considered good if > 10. Two days after giving HCG, the patients were assessed for ultrasonographic signs of ovulation. Clinical pregnancy was defined as the detection of at least one gestational sac on transvaginal ultrasound examination starting one week after the missed period. Results of Letrozole treatment cycles were described as means ± SD, range and median of each variable. A group t-test was used for comparing two means and Chi-Square test to compare proportion. RESULTS Table 1 shows demographic, clinical and hormonal features of all women involved in this study. All patients were either overweight or obese with a mean BMI, 29.61±3.35 Kg/m2 (range 25.9-42.6) with android obesity as indicated by waist circumference (mean 99.9±8.98 cm) and waist/Hip ratio (mean= 0.98± 0.04). Table 2 shows the characteristics of the Letrozole treatment cycles where each patient had received one letrozole treatment cycle. The number of days between completion of treatment with Letrozole and follicular maturity (Letrozole-free period) was 6.2±1.8 days. On the day of HCG administration; the mean number of follicles> or = 18 mm was 1.21±0.86 (range, 1-2) distributed as follows; 19 patients had developed 1 follicle each and 5 patients had 2 follicles each. Letrozole was very well tolerated as no patients complained of any side effect. During Letrozole treatment, ovulation occurred in 24 cases (54.6%) and clinical pregnancy in 6 cases (25%). These pregnancies were single and resulted from timed intercourse in 6 couples; 4 of them developed one follicle each and two couples developed 2 follicles each. There were neither abortions nor multiple pregnancies. Table 3 shows the clinical characteristics of both Letrozole-responders and non-responders, there was insignificant difference between both groups as regards age, period of infertility, BMI, waist circumference, W/H ratio, LH, FSH and LH/FSH ratio. DISCUSSION A simple, inexpensive and safe alternative to CC that can cover the goal of ovulation induction to induce monofollicular development and subsequent ovulation is needed. In this study, the mean (±SD) day of HCG administration was 13.2±1.76 and this agrees with the results of Mitwally and Casper, as it was 14.2±2.1 (1). In this study, the mean (±SD) number of days between completion of treatment with Letrozole and the day of HCG administration was 6.2±1.8 days. Letrozole has a short half-life (around 2 days) leading to lower negligible levels of Letrozole in the body around the time of ovulation and early embryogenesis period (5). Letrozole was very well tolerated as no patients complained of any side effects. Because of the tolerability of Letrozole and its short half-life, Letrozole has been used as a single dose of 20mg on the third day of the menstrual cycle to ensure low levels around the time of ovulation without any side effects (9). In this study, the mean number of mature follicles ≥ 18 mm on the day of HCG administration was 1.21 (range 1-2) where 19 patients (79%) developed one mature follicle and 5 patients (21%) developed 2 mature follicles. This limited number of mature follicles (range 1-2) with Letrozole will decrease the risk of multiple pregnancy and ovarian hyperstimulation syndrome (OHSS). These results are in agreement with the results of Al-Omari et al (10) and Mitwally and Casper (5) Therefore, Letrozole treatment does not need intensive monitoring compared to CC and gonadotropins. In this study, the mean endometrial thickness on the day of HCG administration was 10.2±1.31 mm. Thus the endometrium was of adequate thickness to allow implantation. Letrozole induces ovulation but without estrogen receptors down-regulation. The adverse endometrial effect seen with CC, which is augmented by the relatively long half-life of CC (5 days), are not seen with Letrozole. This result is consistent with the results of other studies; in this study, the mean cervical mucus score was 11.42±2.48 according to the criteria of Moghissi (8). He considered a cervical mucus score of > 10 is a good one while a score of <10 is a poor one. This result indicates that, Letrozole has no adverse antiestrogenic effect on the cervical mucus. This result is consistent with the results of Metawie (11) Poor mucus at midcycle can be a physical barrier that decreases sperm penetration. In this study, ovulation occurred in 24 cases (54.6%). Administration of Letrozole in the early part of the menstrual cycle, would release the pituitary/hypothalamic axis from the estrogenic negative feedback, similar to the effect of CC but without estrogen receptors down-regulation, and the resulting increase in gonadotropin secretion could stimulate ovarian follicle development (1). Also, Letrozole may act locally in the ovary to increase the follicular sensitivity to FSH by increasing the local androgen in the ovary because conversion of androgen substrate to estrogen is blocked. The ovulation rate in this study is lower than that obtained by other studies using Letrozole in ovulation induction. Mitwally and Casper (5) had ovulatory rates of 75%, Al-Omari et al (10) had an ovulatory rate of 87.5% and Metawie (11) had a rate of 92.5%. However, the variable results can be explained by the smaller numbers of the patients of other studies; in our study, we administered Letrozole for only one cycle (i.e. ovulatory rate per cycle), while the 22 patients in Al-Omari study received Letrozole for 32 treatment cycles from the second day of the menstrual cycle (10). Metawie started Letrozole in a dose of 5mg/day for 5 days (11). In this study, pregnancy occurred in 6 patients; thus the percent of pregnancies per induced ovulatory cycle is 25%. This result is comparable with the results of Mitwally and Casper (25%), Al-Omari et al (27.27%) and Metawie (17.5%) (5,10,11). All these pregnancies were single, which is consistent with the results of other studies. This may be due to the limited number of mature follicles (range 1-2). Compared to other methods of ovulation induction, the multiple pregnancy rate is approximately 10% with CC, almost entirely twins (12), about 15-25% with gonadotropins (13) and about 2 % with laparoscopic ovarian drilling (14). Compared to laparoscopic ovarian drilling, there is no risk of operative interference as the anesthetic risk, adhesion formation and the possibility of ovarian destruction and premature ovarian failure (15). Comparing both groups of Letrozole responders and non-responders as regards clinical and laboratory characteristics we found that, there were no significant differences as regards BMI, waist circumference and W/H ratio, hirsutism, LH, FSH and LH/FSH ratio. Thus we can give Letrozole to all patients with CC-resistance, as its efficacy is not limited to a specific abnormality. So it can be used whatever the BMI. Achieving weight reduction is extremely difficult, particularly as the metabolic status of patients with PCOS conspires against weight loss (16). Also, Letrozole can be used with good results in patients with hirsutism and there is no need to add dexamethasone to reduce adrenal androgen production. Dexamethasone can worsen diabetic tendencies because of its effect on blood sugar and as a result, it may not be a suitable treatment for patients with diabetes, insulin resistant or glucose intolerance, conditions present in many PCOS patients (3). Also from these results, Letrozole can be used in case of high LH without the need to add oral contraceptives for pretreatment suppression of LH. Oral contraceptive pills exacerbate insulin resistance and since many patients are overweight and obesity is a relative contraindication, this treatment may be unsuitable (17). Also, there is a doubt about the short and long term safety of ovarian suppression in polycystic ovary with oral contraceptives (18). In conclusion; induction of ovulation with Letrozole in CC-failure PCOS is associated with limited number of mature follicles, no adverse effect on endometrium or cervix, ovulation and pregnancy in a significant number of patients. Induction with Letrozole is not dependent on age, period of infertility, BMI, waist circumference, LH, FSH or LH/FSH ratio. Further studies are necessary to confirm our results. REFERENCES
© Copyright 2004 - Middle East Fertility Society The following images related to this document are available:Photo images[mf04027t3.jpg] [mf04027t1.jpg] [mf04027t4.jpg] [mf04027t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}