 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
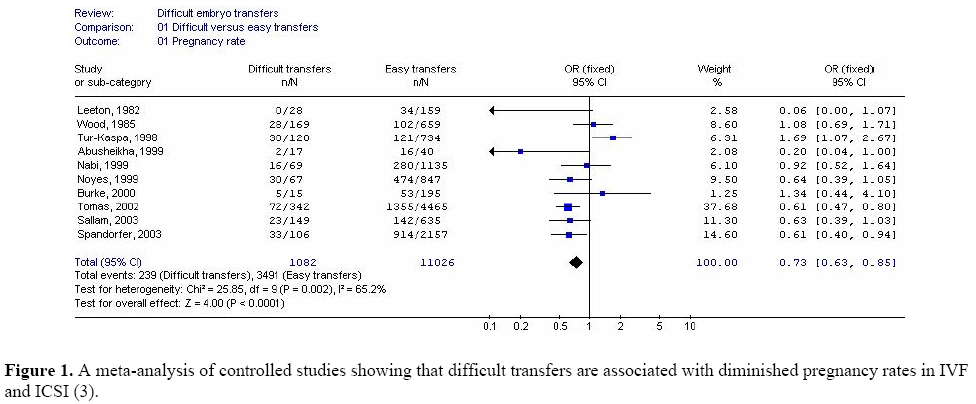
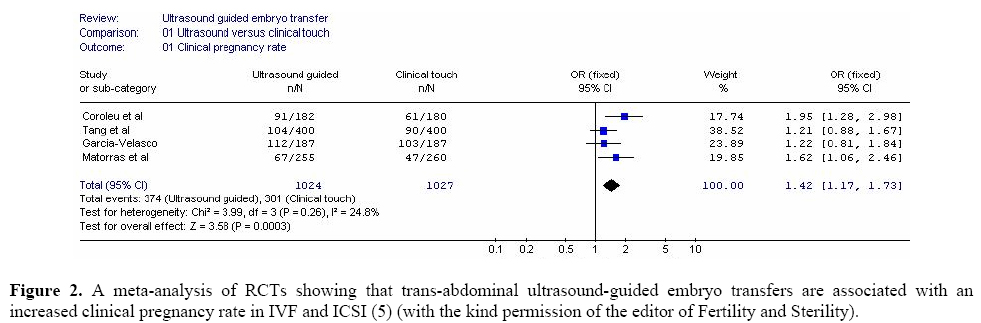
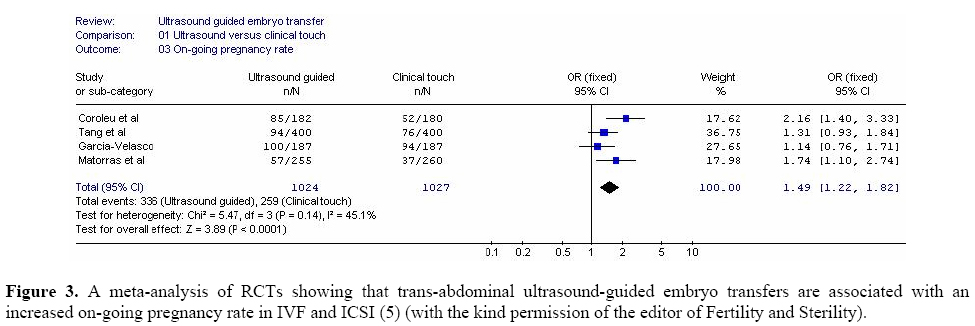
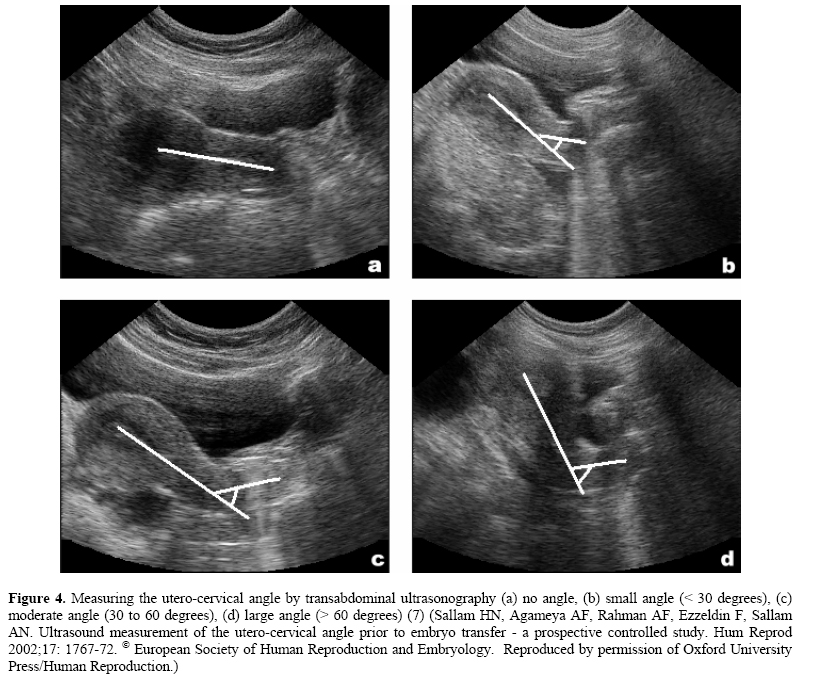
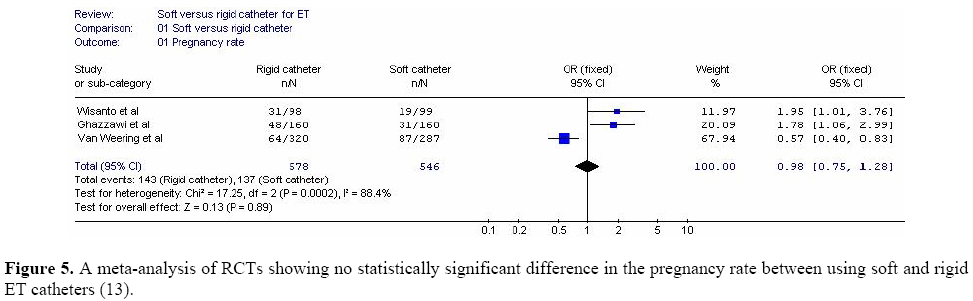
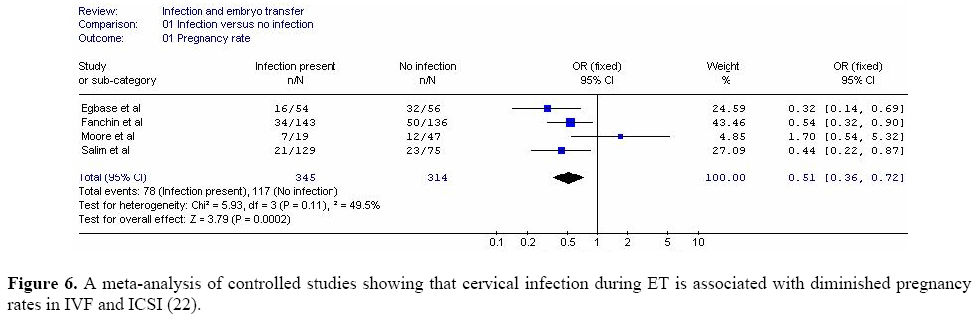
Middle East Fertility Society Journal, Vol. 9, No. 3, 2004, pp. 204-209 DEBATE Embryo transfer techniques: what affects the results? Comment by: Hassan Sallam, M.D., F.R.C.O.G, Ph.D. (London) Alexandria, Egypt Code Number: mf04037 Embryo transfer (ET) is arguably the most critical step in assisted reproduction. Despite numerous developments in IVF and ICSI, the implantation rate of replaced embryos remains low and it is estimated that 85% of the embryos replaced fail to implant (1). This low implantation rate has been blamed on diminished implantation capacity of the embryo, diminished endometrial receptivity but a suboptimal embryo transfer technique has also received much of the blame. Various aspects of the technique are thought to affect affect the results but not all of them have been studied by randomized controlled trials (RCTs). For example, a gentle and atraumatic technique is thought to be necessary during ET and difficult ETs are associated with diminished pregnancy and implantation rates. We have recently reported that changing the catheter and the presence of blood on the catheter tip during ET significantly diminish the pregnancy and implantation rates (2). In a recent meta-analysis, we have also found that difficult transfers are indeed associated with significantly diminished pregnancy [(OR = 0.73, 95% CI (0.63-0.85)] and implantation rates [(OR = 0.64, 95% CI (0.52-0.77)] compared to easy transfers (figure 1) (3). Performing a trial (mock or dummy) ET before the actual transfer has also been suggested in an effort to increase the pregnancy and implantation rates and various studies have been published in this respect. However, only one of these studies was a RCT where the authors reported that the pregnancy and implantation rates were significantly higher in the dummy-transfer group compared to the no-dummy transfer group (4). Performing embryo transfer under ultrasound guidance has also been shown to improve pregnancy and implantation rates over the clinical-feel method. We have recently conducted a meta-analysis of RCTs and found that, compared to the clinical touch method, abdominal ultrasound-guided transfer significantly increases the clinical pregnancy rate [OR = 1.42 (95% CI = 1.17, 1.73)] and the on-going pregnancy rate [OR = 1.49 (95%CI = 1.22, 1.82)] (figure 2 and 3) (5). Performing ET with a full bladder to straighten the utero-cervical angle has been claimed to improve pregnancy and implantation rates (6). We have also found that the utero-cervical angle measured by ultrasound is related to the pregnancy and implantation rates (figure 4) and that patients with acute utero-cervical angles (>60 degrees) had significantly lower pregnancy rates compared to patients with no angles [OR= 0.36, 95% CI (0.16 - 0.52) (7). Moulding the catheter according to the measured angle resulted in a lower incidence of difficult transfers [(OR= 0.25, 95% CI (0.16 - 0.40)] as well as higher pregnancy rates [(OR= 1.57, 95% CI (1.08 - 2.27)]. However, no RCTs have been published so far, to evaluate performing ET with and without a full bladder. In a non-randomized study, Nabi et al found that embryos were significantly more likely to be retained when the ET catheter was contaminated with mucus (3.3 versus 17.8%, P = 0.000001) (8). Consequently, the removal of the cervical mucus prior to ET has been claimed to improve the pregnancy and implantation rates, but no RCTs have so far been published on the routine aspiration of the mucus prior to ET. It has also been claimed that vigorous flushing of the cervical canal with culture medium prior to ET could improve implantation in assisted reproduction. In 1999, MacNamee (9) reported that vigorous flushing of the cervical canal and the use of a soft catheter improved the pregnancy and implantation rates. However, in a RCT, we have found no statistically significant difference with and without flushing in pregnancy rates (25.5% and 34.5 %, P=0.4053) or implantation rates (15.38 % and 17.46 %, P=0.7687) (10). Avoiding the use of a tenaculum (volsellum) has also been suggested as this was found to stimulate uterine junctional zone contractions (11) and to increase plasma oxytocin levels (12). However, the relationship between this practice and pregnancy and implantation rates remains to be studied. The effect of the type of catheter used in ET remains unresolved. Some studies have reported better results with soft catheters. Other studies found the complete opposite and a third group reported no difference. We have recently conducted a meta-analysis of RCTs comparing soft to rigid catheters and found no statistically significant differences in the pregnancy rates between the two types [OR = 0.98, 95% CI (0.75 - 1.28)] (figure 5) (13). The site of embryo deposition is also important. In a RCT, the implantation rate was found to be significantly higher when the embryos were deposited 2 cm below the uterine fundus compared to when deposited 1 cm below the fundus (14). It has also been suggested that midfundal deposition of the embryos results in a lower incidence of ectopic pregnancies compared to deep fundal deposition but these claims have not been substantiated in large RCTs (15). On the contrary, slow withdrawal of the embryo transfer catheter seems to be of no importance. In a RCT, Martinez et al found no statistically significant difference in pregnancy rate when the catheter was withdrawn immediately after ET compared to when it was left for 30 seconds in the uterus before its withdrawal (16). They concluded that either that the waiting interval was insufficient to detect differences or that the retention time before withdrawing the catheter is not a factor influencing pregnancy rate. Adding a fibrin sealant (glue) to the culture medium containing the embryos during ET has also been suggested in a case control study. (17) However, two RCTs failed to confirm these findings (18,19). Bed rest after embryo transfer seems to be of no importance. In a non-randomized study, Sharif et al reported that the clinical pregnancy rate in their patients who had no bed rest following ET was significantly higher than the national data (30% versus 22.9%) (20). These findings were confirmed in a RCT conducted by Botta and Grudzinskas who found no statistically significant differences in the clinical pregnancy rate between patients who had a 24 hour period of bed rest following ET compared to those who had bed rest for 20 minutes only (21).On the contrary, cervical infection was found to be a cause of diminished pregnancy and implantation rates. We have recently conducted a meta-analysis of controlled studies and found that the clinical pregnancy [OR = 0.51, 95% CI (0.36-0.72)] and implantation rates [OR = 0.43, 95% CI (0.31-0.61)] were indeed diminished in the presence of cervical infection (figure 6) (22). However, the effect of routine administration of antibiotics following oocyte retrieval or ET has not been studied by RCTs and is still a matter of debate. Finally, sexual intercourse around the time of embryo transfer is not associated with low success rates. In a RCT conducted by Tremellen et al (23), the clinical pregnancy rate was not affected by sexual intercourse and, contrary to expectations, the implantation rate was significantly increased for patients who had sexual intercourse around the time of embryo transfer. In summary, RCTs have shown that the pregnancy rate in assisted reproduction is significantly increased by performing a dummy ET before the actual transfer, by ultrasound-guided ET and by depositing the embryos 2 cm below the uterine fundus. Similarly, RCTs have shown that bed rest after ET, flushing the cervical canal before ET, sexual intercourse around the time of ET, the use a fibrin sealant, using a soft catheter as opposed to a rigid catheter and slow withdrawal of the ET catheter did not affect the pregnancy rate. The value of removing the cervical mucus prior to ET, performing ET with a full bladder, avoiding the use of a volsellum and the routine administration of antibiotics following ET remains to be studied by RCTs. REFERENCES
Hassan N. Sallam, MD, FRCOG, PhD (London) Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04037f4.jpg] [mf04037f2.jpg] [mf04037f1.jpg] [mf04037f5.jpg] [mf04037f6.jpg] [mf04037f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}