 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
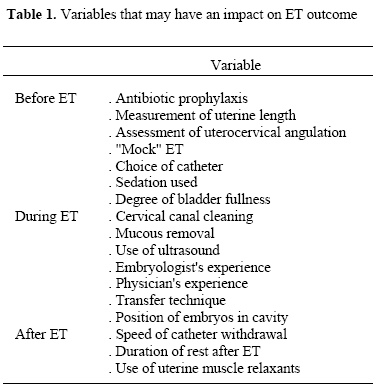
Middle East Fertility Society Journal, Vol. 9, No. 3, 2004, pp. 212-214 DEBATE Embryo transfer techniques: what affects the results? Comment by: Tarek El-Toukhy, M.D., M.R.C.O.G. Mohamed Taranissi, F.R.C.O.G. London, UK. Code Number: mf04039 Until recently, embryo transfer (ET) has received limited clinical attention despite being one of the most critical steps in any IVF cycle (1). Arguably, ET accounts for 20% of the chances of success of IVF treatment (2) and poor ET technique is responsible for up to 30% of all IVF failures (3). Attempts at standardisation of the procedure have encountered great difficulties because of the limited data available in the literature, the large number of variables involved in the procedure (Table 1) and, more importantly, because operator's experience is a major confounding variable (4) that is likely to introduce bias when comparing data from various studies. This debate will focus on two variables involved in the procedure of ET; the first, because it is pivotal in the success of ET and the second because it has been the subject of numerous recent studies. a) Cervical canal cleaning and mucous removal If dragged into the endometrial cavity with the transfer catheter, cervical canal mucous can entangle the embryos, interfere with implantation and increase the risk of cervical expulsion of the embryos (5, 6). It has also been suggested that the presence of cervical mucous can prevent the embryos from leaving the catheter by acting as a "plug" at the catheter tip (1). Although this latter theory is credible, embryo retention is unlikely to compromise significantly the chances of treatment success since implantation rate is not reduced when the embryos are immediately transferred into the cavity in a second attempt (7, 8). Another benefit of cervical cleaning and mucous removal is to reduce the risk of bacterial contamination of the catheter and endometrial cavity. Evidence that endocervical pathogens are present in a considerable number of patients at the time of ET exists. Furthermore, contamination of the catheter tip with micro-organisms such as streptococci (groups B and D), E. coli, staphylococci, mycoplasma and ureaplasma has been shown to reduce implantation and pregnancy rates by 40%-60% (9-13) even when prophylactic antibiotics have been used. Cleaning the cervical canal, therefore, can play a beneficial role by modifying the cervical micro-environment and reducing the risk of introducing pathogens into the endometrial cavity. b) Use of ultrasound guidance Interest in the use of ultrasound (US) has arisen from knowledge that position of the catheter in the uterine cavity can influence the chances of pregnancy. Mid fundal transfer ensuring a distance of about 20 mm from the uterine fundus has been shown to be associated with significantly improved implantation and pregnancy rates compared to high fundal transfers(14, 15). Consequently, clinicianstended to use abdominal US to guide embryo placement in the cavity. Some authors even went further and evensuggested theuse of transvaginal US (16) and transfer catheter with an echogenic tip to improve visualization (17). At least 10 comparative studies have been conducted so far to assess the value of using US during ET (14, 18-26). Although four of those studies showed an improvement in pregnancy rates when ET was guided with US, there were six studies which included over 2500 transfers and failed to show significant improvement in pregnancy rate when US was compared to "clinical touch". This lack of universal agreement on the value of using US to guide ET is intriguing and suggests that precise placement of embryos at a specific level within the uterine cavity perhaps is not as important as originally perceived. Indeed, one recent randomized study (27) looked at the distance between the uterine fundus and the catheter tip in 400 transfers and concluded that implantation and pregnancy rates were similar whether the embryos were deposited in the upper or lower half of the endometrial cavity. Furthermore, experience at the clinic with the highest live birth rate in the United Kingdom for eight consecutive years (28), where US is seldom used to guide ET, confirms that notion. This implies that, excluding the uppermost 1.5 cm and the lowermost 1.5 cm of the cavity, embryo placement at any intermediate level in the cavity is likely to yield similar results. It is imperative, however, that some form of cavity length assessment is performed. As the uterine cavity length is known to be remarkably similar in all normal uteri, most cases in our practice will have a transfer at six cm from the external os. However, if preliminary US assessment suggests deviation of the cavity length from normality, the uterine cavity is assessed and its length accurately measured via hysteroscopy (preferably) or at least a "mock" ET (29). Ultrasound monitoring of ET is thus limited to cases where there is cervical or uterine (congenital or acquired) anomaly. One of the main advantages of using US in those unusual cases is to ensure passage of the ET catheter into the uterine cavity past the internal cervical os. In conclusion, many confounding variables seem to influence the outcome of ET. This makes analysis of the limited published data difficult. Standardization of the steps of the procedure may enable better comparison of the different studies in the literature. Total elimination of bias, however, is unlikely since physician's expertise, a major confounder, cannot be standardised. Nevertheless, certain factors appear to be more important than others. These include prior assessment of cavity length and direction, cleaning of the cervical canal and removal of all mucous encountered and finally adopting an atraumatic gentle technique to deliver the embryos to mid cavity, with or without US guidance. REFERENCES
Tarek El-Toukhy, M.D., M.R.C.O.G. Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04039t1.jpg] |
| |||||||||

{kind=link}